In this podcast episode, we continue our summer series reviewing landmark ARDS studies. Today, Dave and Luke discuss the Driving Pressure trial (published in NEJM in 2015) which evaluated the impact of driving pressure on survival in patients with ARDS.
Article and Reference
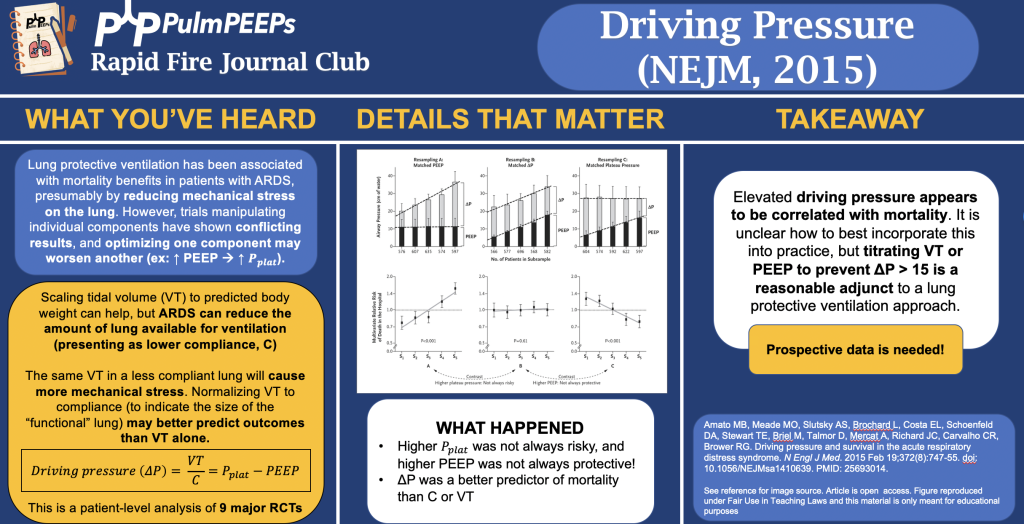
We are talking about the Driving Pressure trial today which evaluated the impact of driving pressure, as an independent variable, on survival in patients with ARDS.
In the penultimate episode in our ARDS Rapid Fire Journal Club Summer Series we are talking about the DEXA-ARDS trial (published in Lancet Respiratory Medicine in 2020). This trial evaluated the impact of dexamethasone in the treatment of ARDS.
Article and Reference
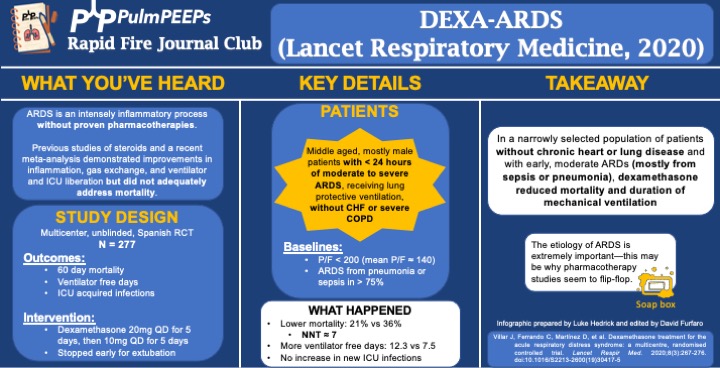
Today we’re discussing the DEXA-ARDS trial published in Lancet Respiratory Medicine in 2020. This trial evaluated the impact of dexamethasone on mortality and duration of mechanical ventilation for patients with ARDS.
Background: ARDS is an intense inflammatory process without proven, specific pharmacotherapies. Previous work and a recent meta-analysis demonstrated improvements in inflammation, gas exchange, and ventilator and ICU liberation but did not adequately address mortality.
Study Design (design, primary outcome, participants, etc)
Design: investigator-initiated, multicenter, unblinded, randomized controlled trial in 17 academic ICUs in Spain, conducted from 3/2013 to 12/2018
Primary Outcome
VFD at 28d
Secondary:
60d mortality
Actual duration of ventilation in ICU survivors
ICU acquired infections
Participants
Inclusion ARDS with P/F < 200 for < 24hr on LTVV
Exclusion:
Already receiving steroids or immunosuppression
CHF
Severe COPD
DNR
Summary: Middle aged, mostly male patients with < 24hr of moderate to severe ARDS receiving LPV without chronic heart or lung disease
Like many ARDS trials, just over 3/4 of patients’ ARDS was caused by PNA or sepsis. Mean P/F was ~140
Intervention/Limitations
N = 277, stratified by center and then randomized
Intervention: dexamethasone 20mg qd for 5d followed by 10mg qd for 5d
Stopped early for extubation before day 10
First dose given no more than 30 hours after P/F < 200
Control: no placebo, just SOC
All patients received LTVV
Outcomes/Safety
Power: with N = 314 (actual N = 277), 80% power to detect 2 additional VFD and 15% mortality reduction
As an aside, this seems to be a theme in ICU trials: massively ambitious proposed benefits during power calculations and then under-enrolling for that power calculation ultimately resulting with a point estimate that favors the intervention but is not statistically significant.
Efficacy:
60d mortality: 21% vs 36%, P = 0.0047
NNT of just < 7!
VFD at 28d: 12.3 vs 7.5, P < 0.0001
Actual duration of ventilation in ICU survivors: 14.2d vs 19.5d (P = 0.0009)
Safety:
Hyperglycemia: 76% vs 70%, P = 0.33
Always interesting in steroid trials when no change in glucose control is seen. This isn’t the most EBM thing I’ll ever say, but frankly I disregard this and assume steroids will cause hyperglycemia regardless of the trial results.
ICU acquired infections: 24% vs 25%, P = 0.75
Takeaway
In a narrowly selected population of patients without chronic heart or severe lung disease and with early, moderate ARDS (mostly from sepsis or pneumonia), dexamethasone reduced mortality and duration of mechanical ventilation.
If time, insert soap-box about etiology of ARDS being very important (EG, flu, fungal, parasitic, mycobacterial infections)
We have another great case in our Fellows’ Case Files coming today from UMass Chan. Listen in for a great discussion about a fascinating case with interesting physical exam and radiographic findings.
Meet Our Guests
Dr. Jen Kodela completed her residency training at UMass Memorial Medical Center and is currently a third year PCCM fellow at UMass Chan.
Dr. Ariel McKenna completed her residency training at Maine Medical Center and is also currently a third year PCCM fellow at UMass Chan.
Dr. Will Wong is an Assistant Professor of Medicine and is the Program Director of the PCCM fellowship at UMass Chan
Case Presentation
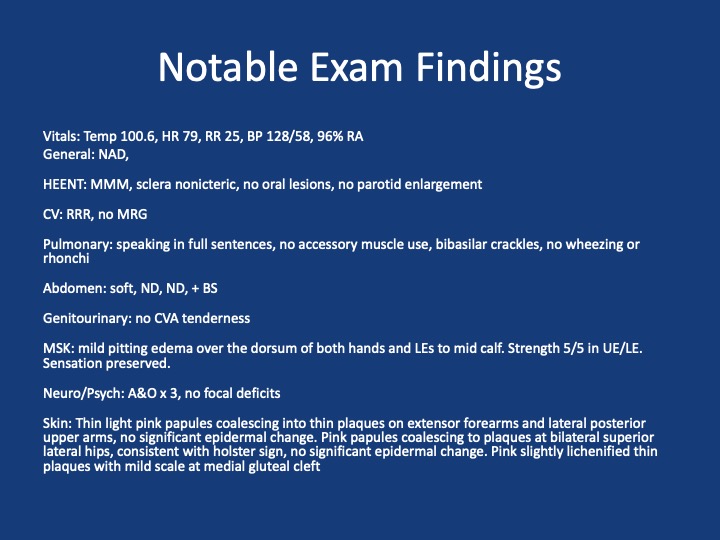
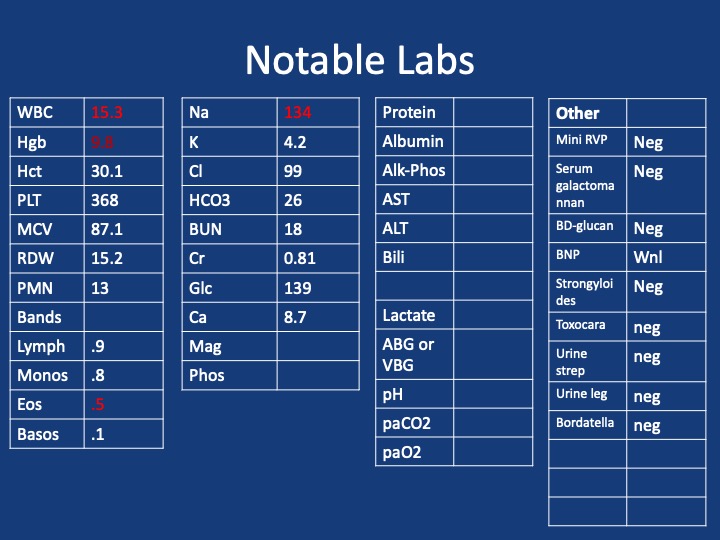
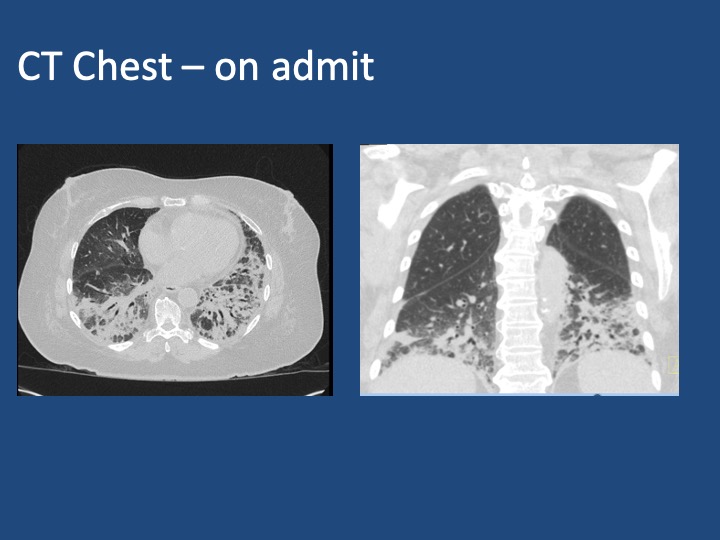
A 75 y/o F presenting with acute on chronic SOB, cough, L sided chest pain and rash. She has had ~7 months of progressive dyspnea, now a/w 2 months of productive cough, and several weeks of L sided chest pain and rash. She has been seen multiple times in the past two months for these sxs. During that time she received multiple antibiotic courses (urgent care, outpatient providers), including augmentin, azithromycin and levaquin, and asthma directed therapy (no steroids). Imaging throughout that time (CXRs, CTPE) show progression from a LLL infiltrate to bibasilar infiltrates. Despite these interventions, sxs continue to worsen. One month prior she was admitted to an OSH w/ continued worsening, vitals stable, exam nonfocal, mild leukocytosis but infectious w/u bland. Received broad spectrum abx. Bronch w/ BAL offers negative cultures, cytology, cell count w/ 66% neutrophils, 14% eosinophils. Discharged w/ dx of PNA on a 10 day course of levaquin and new exertional oxygen requirement of 2L. She then presents to Umass ~1 month later w/ continued progression of sxs
Key Learning Points
1. Formulate a differential diagnosis for non-resolving pneumonia
2. Evaluate the utility of transbronchial biopsy in the workup of undifferentiated ILD
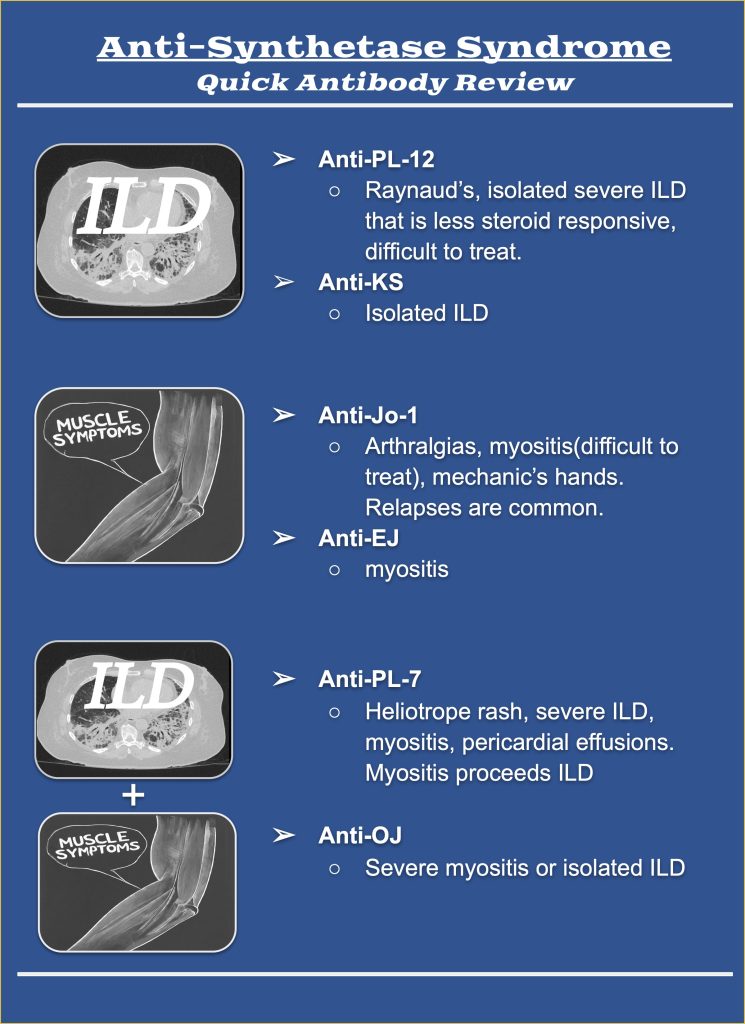
3. Describe the clinical manifestations of antisynthetase syndrome and identify the differences in presentation associated with PL-12 positivity
References and Further Reading
1. Kuru T, Lynch JP 3rd. Nonresolving or slowly resolving pneumonia. Clin Chest Med. 1999 Sep;20(3):623-51. doi: 10.1016/s0272-5231(05)70241-0. PMID: 10516909.
2. Troy LK, Grainge C, Corte TJ, Williamson JP, Vallely MP, Cooper WA, Mahar A, Myers JL, Lai S, Mulyadi E, Torzillo PJ, Phillips MJ, Jo HE, Webster SE, Lin QT, Rhodes JE, Salamonsen M, Wrobel JP, Harris B, Don G, Wu PJC, Ng BJ, Oldmeadow C, Raghu G, Lau EMT; Cryobiopsy versus Open Lung biopsy in the Diagnosis of Interstitial lung disease alliance (COLDICE) Investigators. Diagnostic accuracy of transbronchial lung cryobiopsy for interstitial lung disease diagnosis (COLDICE): a prospective, comparative study. Lancet Respir Med. 2020 Feb;8(2):171-181. doi: 10.1016/S2213-2600(19)30342-X. Epub 2019 Sep 29. PMID: 31578168.
3. Hallowell RW, Danoff SK. Diagnosis and Management of Myositis-Associated Lung Disease. Chest. 2023 Jun;163(6):1476-1491. doi: 10.1016/j.chest.2023.01.031. Epub 2023 Feb 9. PMID: 36764512.
4. Hallowell RW, Paik JJ. Myositis-associated interstitial lung disease: a comprehensive approach to diagnosis and management. Clin Exp Rheumatol. 2022 Feb;40(2):373-383. doi: 10.55563/clinexprheumatol/brvl1v. Epub 2021 Mar 25. PMID: 33769263; PMCID: PMC8855729.
5. Marie I, Josse S, Decaux O, Dominique S, Diot E, Landron C, Roblot P, Jouneau S, Hatron PY, Tiev KP, Vittecoq O, Noel D, Mouthon L, Menard JF, Jouen F. Comparison of long-term outcome between anti-Jo1- and anti-PL7/PL12 positive patients with antisynthetase syndrome. Autoimmun Rev. 2012 Aug;11(10):739-45. doi: 10.1016/j.autrev.2012.01.006. Epub 2012 Feb 3. PMID: 22326685.
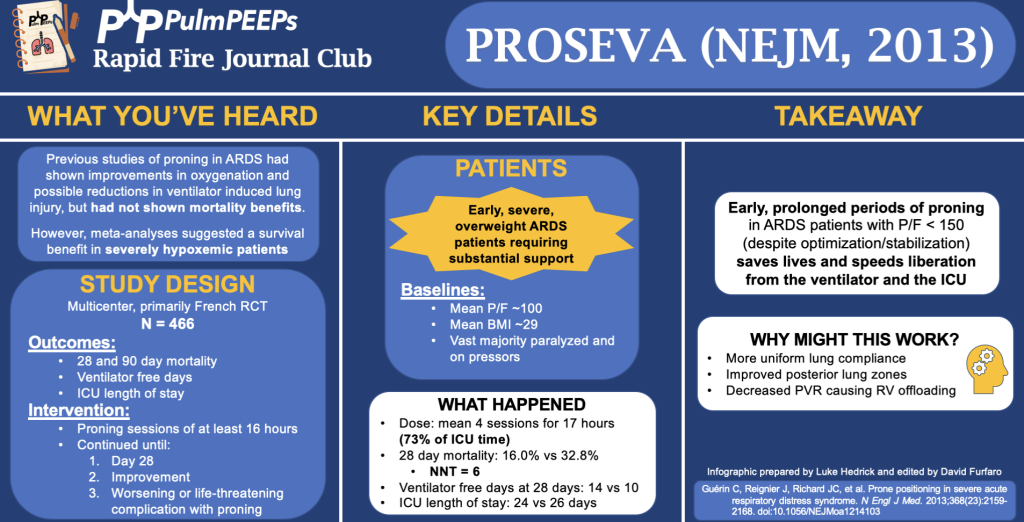
In this podcast episode, we continue our summer series reviewing landmark ARDS studies. Today, Dave and Luke discuss the PROSEVA trial (published in NEJM in 2013) which evaluated the impact of early, prolonged proning in patients with severe ARDS.
Article and Reference
We are talking about the PROSEVA trial today which evaluated the patients with severe ARDS (P/F < 150) to undergo prone-positioning sessions of at least 16 hours or to be left in the supine position.
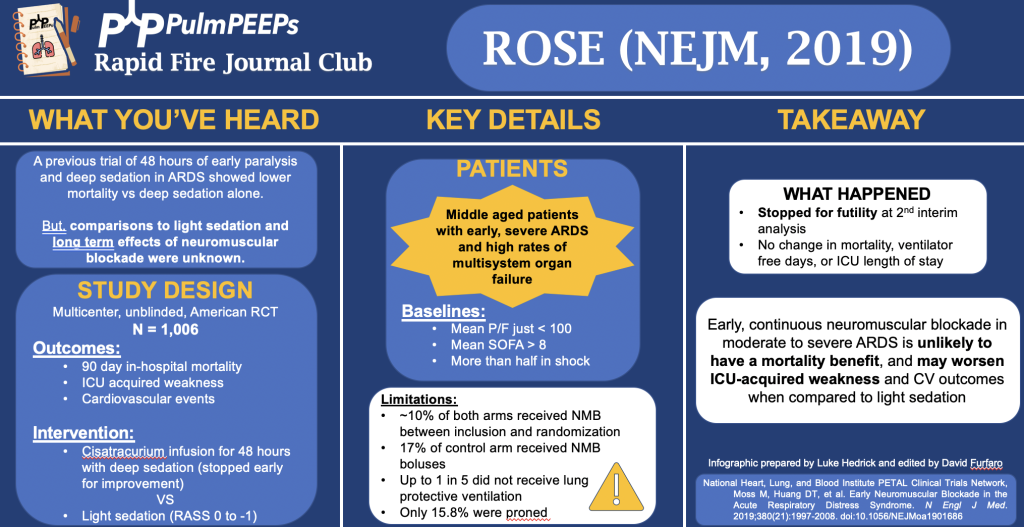
In this podcast episode, we continue our summer series reviewing landmark ARDS studies. Today, Dave and Luke discuss the ROSE trial (published in NEJM in 2019) which investigated use of continuous neuromuscular blockade in moderate to severe ARDS.
Article and Reference
We are talking about the ROSE trial today which was a comparison of early continuous neuromuscular blockade in patients with ARDS who were receiving mechanical ventilation.
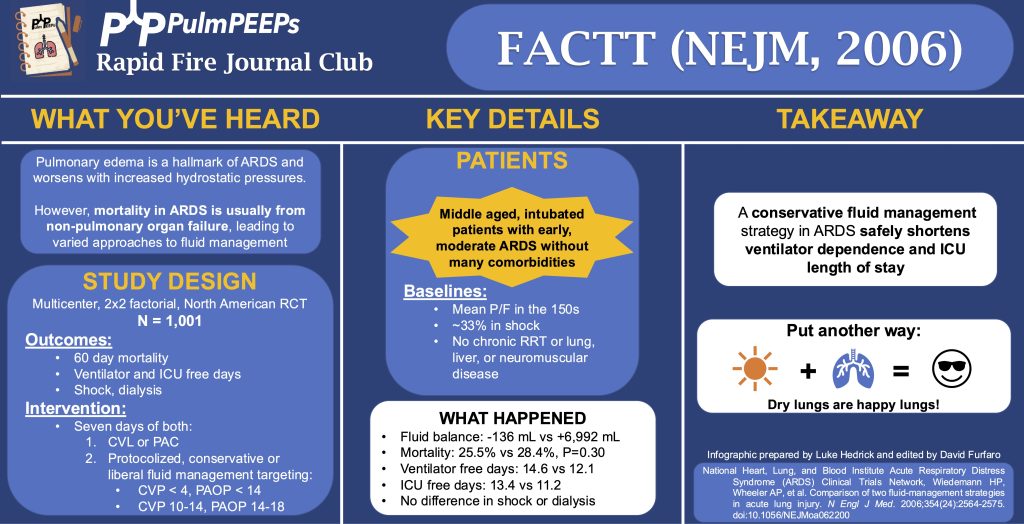
Background: The FACT trial aimed to address fluid balance in ARDS, given the complexity of managing pulmonary edema and systemic organ failure. The challenge has been finding the right balance between managing fluid to optimize cardiac function and avoiding exacerbation of pulmonary edema.
Study Design:
Randomized Controlled Trial: Conducted at 20 North American medical centers from 2000 to 2005.
Participants: Included intubated ARDS patients who required or were planned to receive a central venous catheter. Excluded patients with chronic diseases, recent MI, or irreversible conditions. Shock was not an exclusion criterion.
Interventions: Patients were randomly assigned to either a liberal or conservative fluid management strategy, and also received either a PA catheter or a central line.
Fluid Management Protocol:
Liberal Strategy: Aimed for higher filling pressures (CVP of 10-14 or wedge pressure of 14-18).
Conservative Strategy: Aimed for lower filling pressures (CVP less than 4 or wedge pressure under 14).
Fluid Balance: The liberal group had a net positive fluid balance of around 7 liters, while the conservative group had a net negative balance of about 130 cc.
Results:
Mortality: No statistically significant difference in 60-day mortality between the liberal and conservative groups (25.5% vs. 28.4%, respectively).
Ventilator and ICU-Free Days: The conservative strategy resulted in more ventilator-free and ICU-free days.
Shock and Dialysis: There was no difference in shock rates, but the conservative group had a trend toward fewer dialysis requirements (10% vs. 14%, p=0.06).
Conclusion: The trial indicated that a conservative fluid management strategy in ARDS patients can reduce ventilator dependence and ICU length of stay without worsening shock or end-organ function. It underscores the benefit of managing fluid conservatively to protect lung function, even though it didn’t significantly reduce mortality.
Overall, the FACT trial supports the practice of conservative fluid management in ARDS, advocating that “dry lungs are happy lungs” for improving patient outcomes.
Today, we’re going to be talking about pre-oxygenation methods for endotracheal intubation and the PREOXI Trial which is hot off the presses in the New England Journal of Medicine in June of 2024. This trial has potentially widespread, practice changing results and we’re lucky enough to be joined by two of the authors to discuss.
Meet Our Guests
Dr. Kevin Gibbs is an Associate Professor of Medicine at Wake Forest University School of Medicine. He obtained his MD at George Washington University School of Medicine, and completed his residency and fellowship training at Johns Hopkins. He is an active researcher in critical care, ARDS, mechanical ventilation, and pragmatic trial design.
Dr. Jon Casey is an Assistant Professor of Medicine for the Division of Allergy, Pulmonary, and Critical Care Medicine at Vanderbilt University Medical Center. He obtained his MD from the University of Louisville School of Medicine, and completed his residency training at Brigham and Women’s Hospital before going to Vanderbilt for fellowship training. He is a physician scientist and also has his Masters of Science in Clinical Investigation. His research is focused on comparative effectiveness of ICU treatments and he also has a focus on pragmatic trials. He is supported with NIH funding and is active in the American Thoracic Society Critical Care Assembly.
Summarized Key Points
Significance of the Problem: Tracheal intubation in emergency and ICU settings is common, with significant risks such as hypoxemia (10-20% incidence) and cardiac arrest (2% incidence) associated with the procedure. This makes effective pre-oxygenation crucial.
Methods of Pre-oxygenation: Common methods include face mask oxygen (e.g., non-rebreather, bag-mask devices) and more advanced techniques like non-invasive ventilation (used in about 15% of cases globally). Each method has pros (e.g., simplicity, no risk of aspiration for face masks; 100% oxygen delivery, positive pressure for non-invasive ventilation) and cons (e.g., potential for gastric insufflation with non-invasive ventilation).
Study Design: The study discussed in the podcast is a pragmatic trial aiming to optimize pre-oxygenation strategies to prevent peri-intubation hypoxemia. Eligibility criteria were broad, encompassing most patients undergoing tracheal intubation in the ED or ICU, with exclusions mainly for safety reasons.
Primary Outcome: The primary outcome of the trial was hypoxemia, defined as oxygen saturation < 85%. This threshold was chosen because it signifies a critical point on the oxygen dissociation curve, where patients are at higher risk of further desaturation and adverse outcomes.
Secondary Outcomes: Secondary exploratory outcomes included more severe levels of hypoxemia (oxygen saturation < 80% and < 70%), aiming to capture varying degrees of oxygenation failure during intubation. Rates of cardiac arrest during intubation were an additional outcome.
Intervention Comparison:
The trial compared two methods of pre-oxygenation: non-invasive ventilation (NIV) and oxygen mask (face mask)
Both methods aimed to provide at least three minutes of pre-oxygenation before intubation.
NIV group specifics: Expiratory pressure of 5 cm H2O, Inspiratory pressure of 10 cm H2O, respiratory rate of 10 breaths per minute, and 100% oxygen delivery
Oxygen mask group specifics: Non-rebreather or bag mask device with at least 15 liters per minute oxygen flow.
Nasal cannulas and HFNC could be used in both groups.
Logistics and Equipment Use:
The trial allowed flexibility in using available equipment (invasive ventilator capable of NIPPV vs. dedicated BiPAP machine).
Sites were encouraged to use the same ventilator for both pre-oxygenation and subsequent ventilation to streamline workflow and reduce logistical challenges.
Primary and Secondary Outcomes:
Results showed a significant reduction in hypoxemia incidents in the NIV group compared to the oxygen mask group.
There was also a reduction in severe hypoxemia and a notable decrease in cardiac arrest incidents in the NIV group.
Aspiration Safety:
There was no statistical difference in aspiration-related outcomes between the NIV and oxygen mask groups, indicating that NIV did not increase the risk of aspiration.
Conclusions:
The trial concluded that NIV for pre-oxygenation significantly reduced the incidence of hypoxemia and possibly cardiac arrest during tracheal intubation.
It also dispelled concerns about increased aspiration risk with NIPPV as pre-oxygenation, suggesting it can be safely used in clinical practice.
This episode is launching our 2024 Rapid Fire Journal Club summer series on ARDS! This summer we will be talking about landmark ARDS trials that have defined the literature and shaped patient care. Journal clubs often focus on new trials, and so learners may have a less thorough understanding of the baseline literature that defines many of our ICU practices. The goal of this series is to provide a quick, but in-depth look at these papers so that learners understand the modern landscape of ARDS.
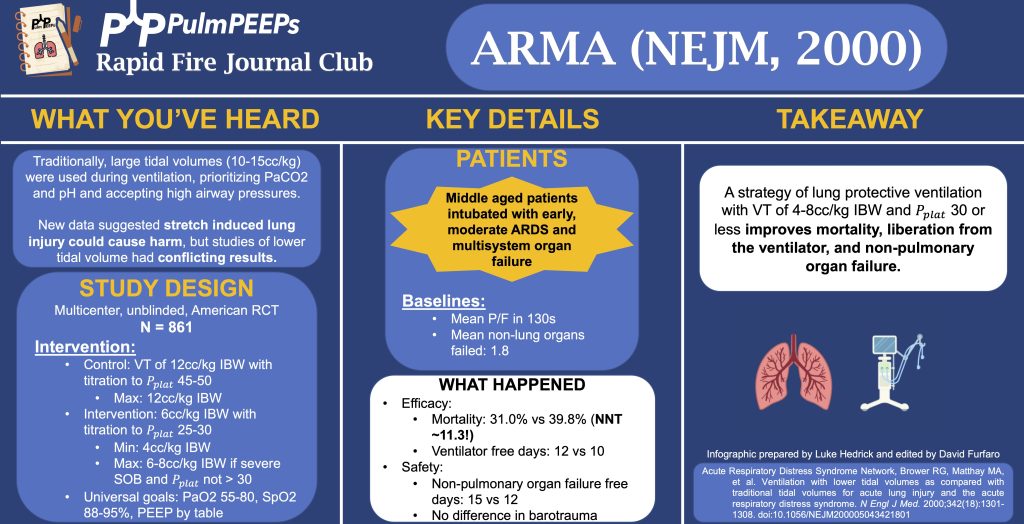
We’re talking about the ARMA trial today which examined “Ventilation with Lower Tidal Volumes as Compared with Traditional Tidal Volumes for Acute Lung Injury and the Acute Respiratory Distress Syndrome.”
We mention a step-wise titration of tidal volume in the control group to achieve Pplats of 45-50. To clarify, there was no adjustment of Vt in the traditional Vt group unless Pplat > 50. If Vt had been decreased in the traditional Vt group because Pplat was > 50, it would not be subsequently increased back to 12 unless Pplat < 45 (to avoid a cycle of corrections and re-adjustments). Similarly in the lower Vt group, there was no adjustment (“titration”) of Vt unless Pplat > 30, and there was a similar protocol in place not to increase the Vt again unless the Pplat was < 25.
Today we’re back with another stop on our Fellows’ Case Files journey and making our way to the University of Rochester. Tune in to hear about this fascinating case and learn some key teaching points along the way.
Meet Our Guests
Dr. Shiv Patel completed his IM residency and a Chief year at the California Pacific Medical Center- Van Ness Campus and is currently a second-year PCCM fellow at the University of Rochester.
Dr. Mary Anne Morgan is an Associate Professor of Medicine and the Fellowship Program Director for the PCCM Fellowship at the University of Rochester. Her clinical interests range from the care of critically ill patients in the ICU to the diagnosis and management of rare lung disease in her role as Director of the University of Rochester LAM Clinic. She loves unwrapping clinical reasoning with trainees, exploring issues around communication and teamwork in the ICU, and is excited about curriculum revitalization in the growing URMC PCCM fellowship program.
Case Presentation
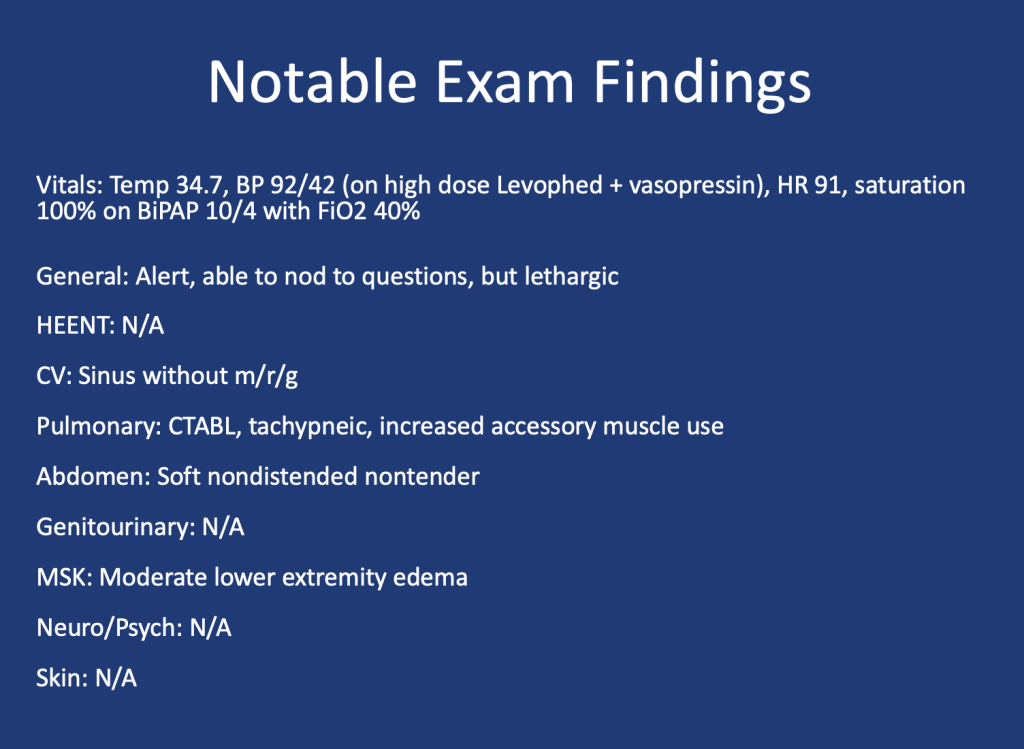
A 75 y.o. female with a history of Hypertension, Hyperlipidemia, and Type 2 Diabetes presented for evaluation of hypoglycemia and generalized fatigue. She had felt poorly for about a week with symptoms of back pain, generalized weakness, and dyspnea, all of which acutely worsened on the day of presentation.
She was found to be hypoglycemic with a blood glucose level in the to 40’s. Initial vital signs included a heart rate of 56, blood pressure of 70/40, respiratory rate of 30, and temperature of 28.5 degrees Celsius.
Key Learning Points
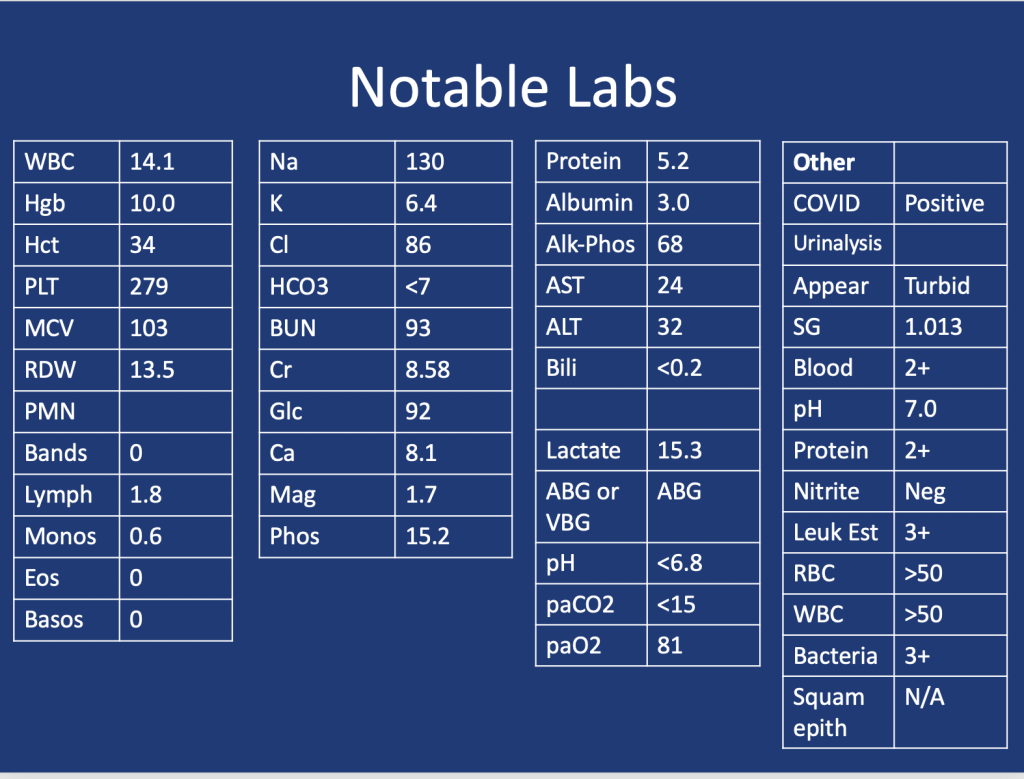
Lactic Acidosis: Type A, Type B and Type D
Type A: Typically secondary to conditions that impair oxygen delivery (respiratory failure, PE) to tissues or decrease tissue perfusion (severe anemia, shock). Patients typically present with hypotension, tachycardia, tachypnea, altered mental status, and signs of organ dysfunction.
Type B: Typically secondary to conditions that directly affect cellular metabolism or lactate clearance and characterized by the presence of hyperlactatemia without evidence of tissue hypoperfusion or hypoxia. Conditions associated include liver dysfunction (e.g., liver failure, cirrhosis), malignancies (especially hematological malignancies), medications/toxins (e.g., metformin, cyanide poisoning), inborn errors of metabolism, and mitochondrial disorders.
Type D: Less common presentation and can be seen in patients with short gut syndrome.
References
1.Blough B, Moreland A, Mora A Jr. Metformin-induced lactic acidosis with emphasis on the anion gap. Proc (Bayl Univ Med Cent). 2015 Jan;28(1):31-3. doi: 10.1080/08998280.2015.11929178. PMID: 25552792; PMCID: PMC4264704.
2.Callelo et al. Extracorporeal Treatment for Metformin Poisoning: Systematic Review and Recommendations From the Extracorporeal Treatments in Poisoning Workgroup. DOI: 10.1097/CCM.0000000000001002
3.Friesecke, S., Abel, P., Roser, M. et al. Outcome of severe lactic acidosis associated with metformin accumulation. Crit Care14, R226 (2010). https://doi.org/10.1186/cc9376
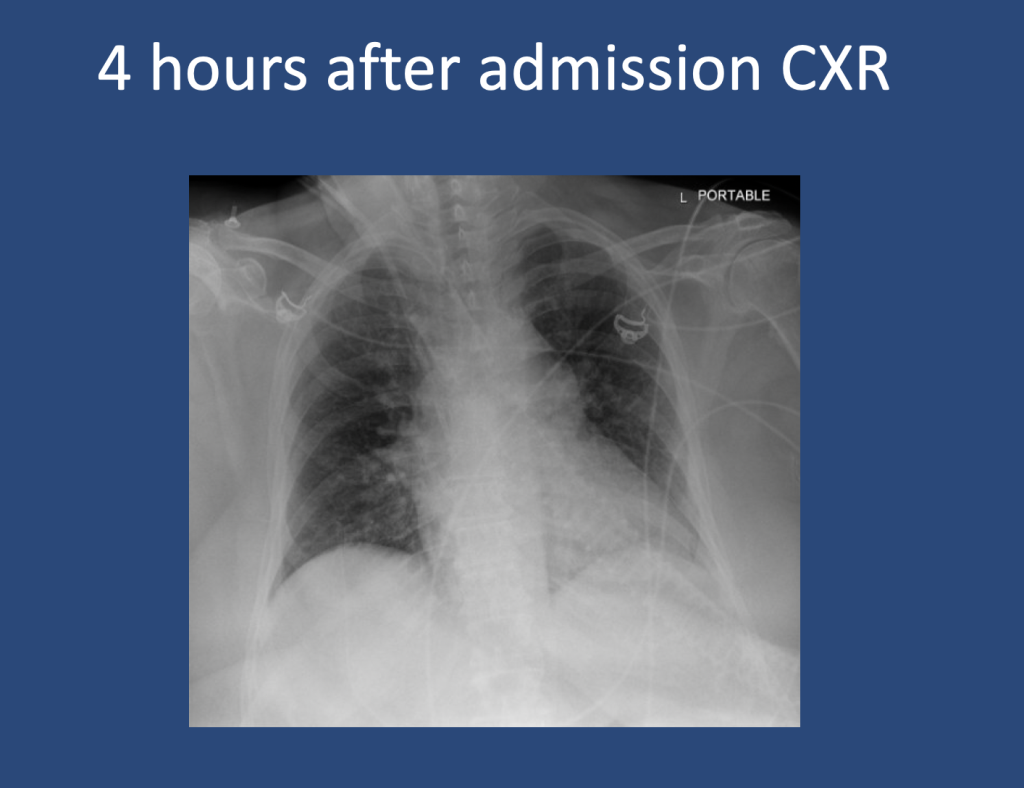
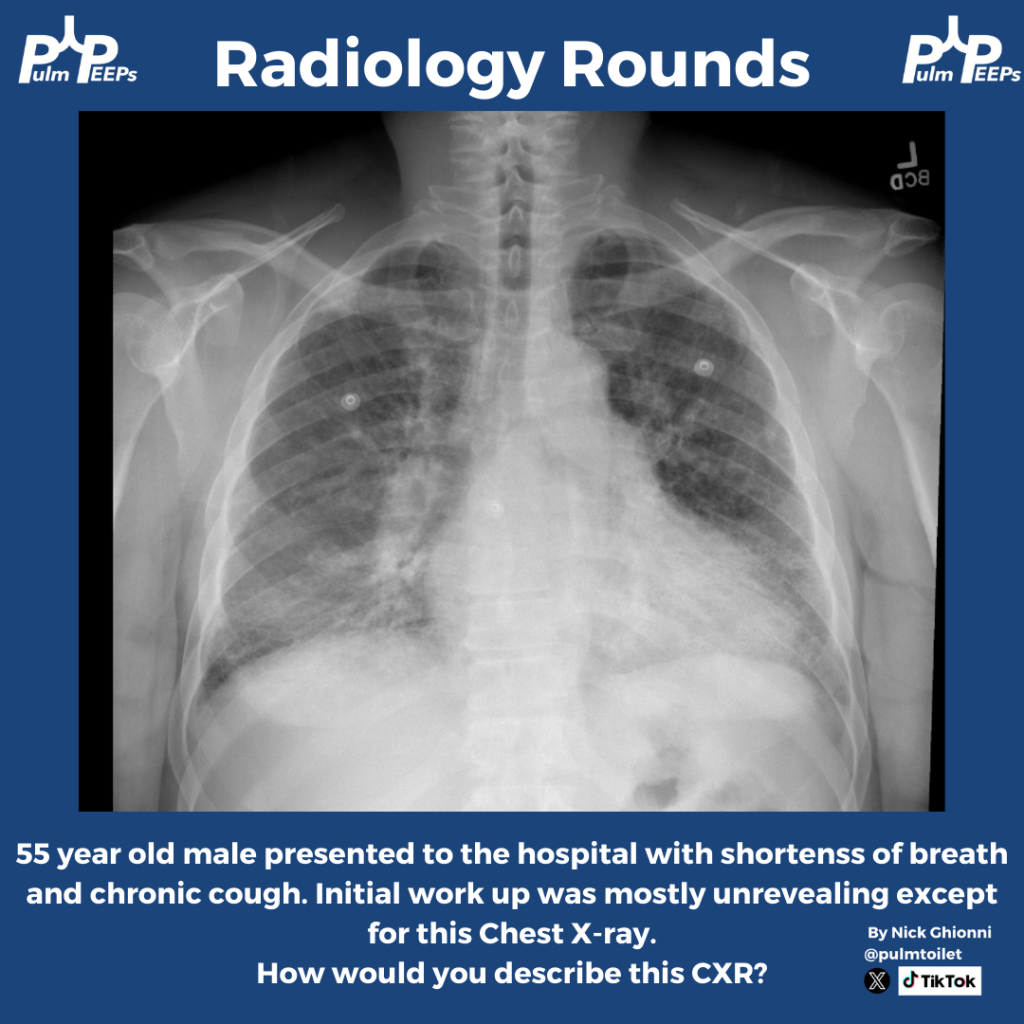
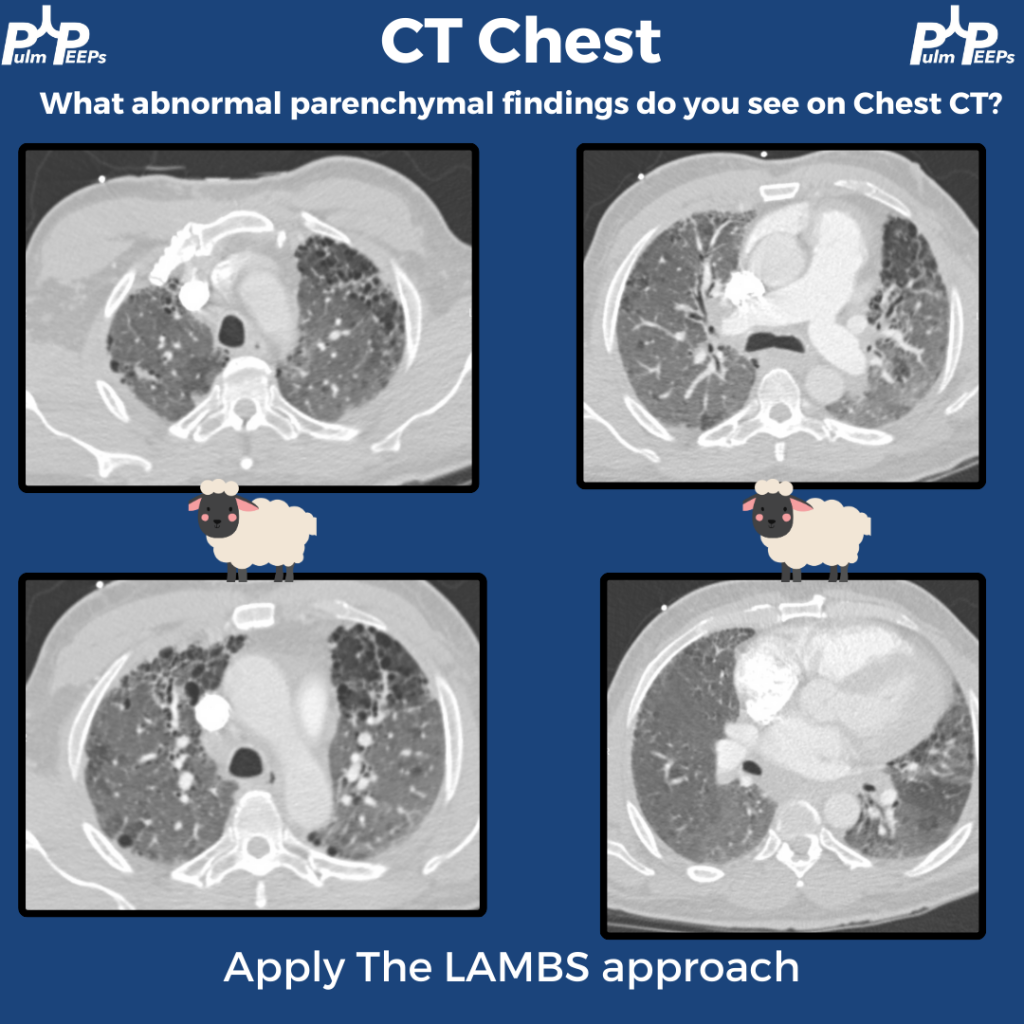
Time for another Radiology Rounds! This case is brought to you by our Associate Editor Nick Ghionni @pulmtoilet ! A 55 year old man presents to the hospital with progressive dyspnea and a chronic cough. Here is his initial CXR.
Further history and exam is taken and is notable for
Progressive dyspnea, especially with exertion
Has received courses of steroids and antibiotics in the past
Breeds pigeons
Tachypneic on exam, scattered rales, and rare faint wheeze
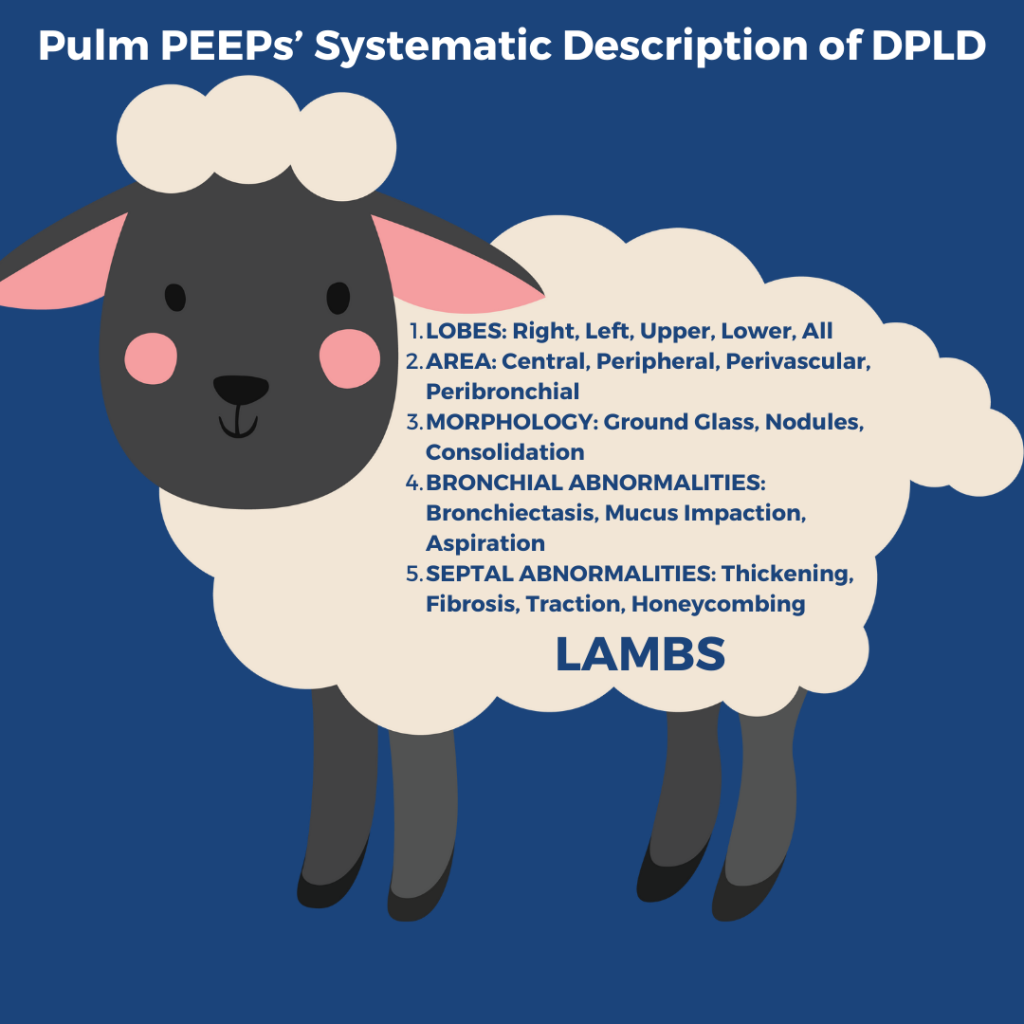
A high resolution, thin cut, CT w/out contrast inspiratory and expiratory, and prone and supine is performed. Here are some key images Remember to apply Pulm PEEPs’ LAMBS approach to reading CTs with diffuse parenchymal findings
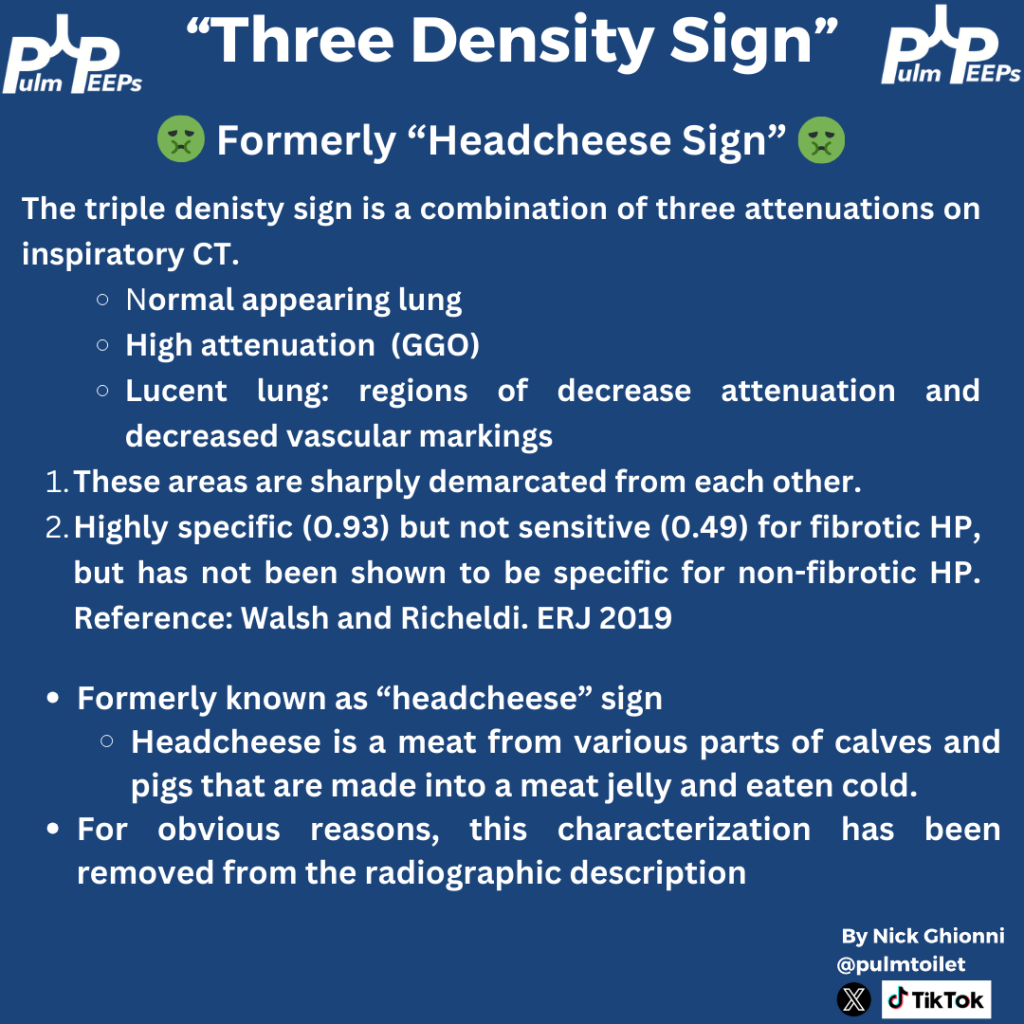
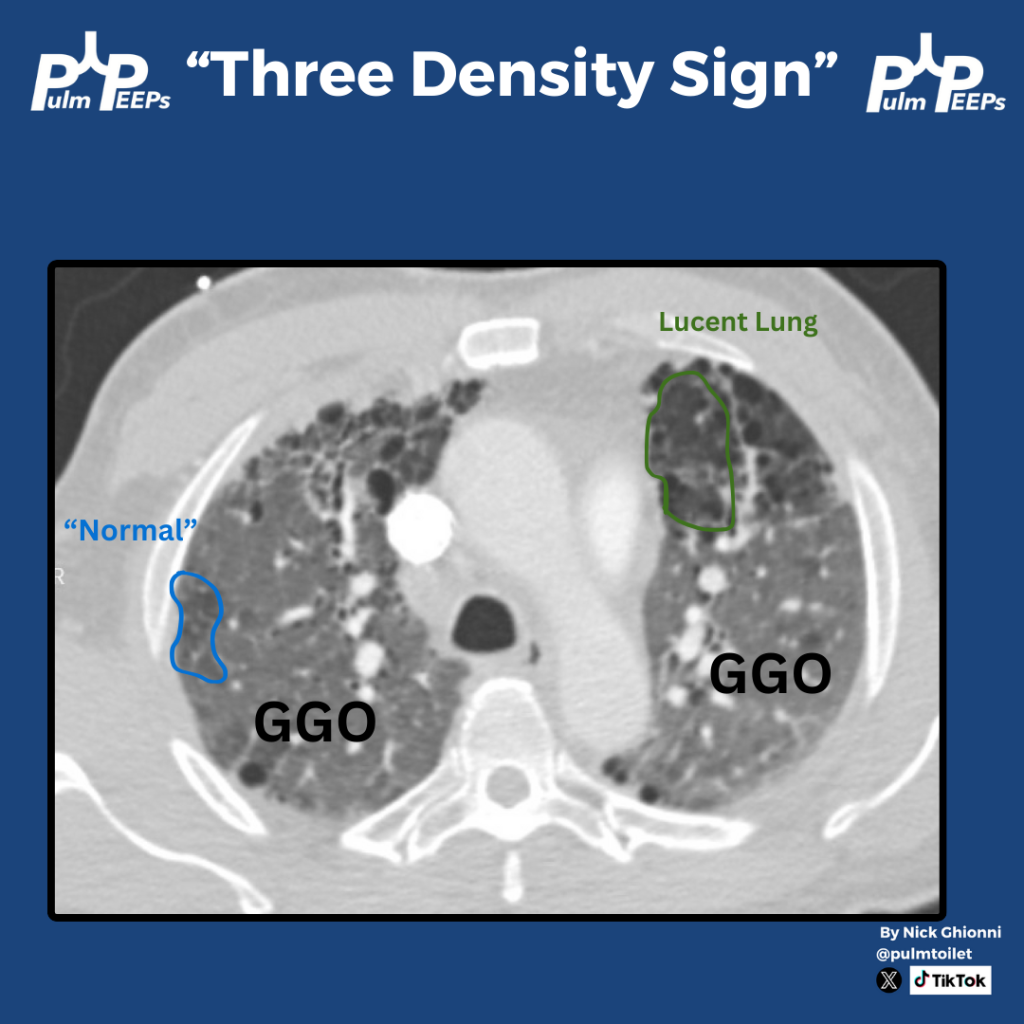
The CT scan shows an example of Triple Density Sign (formerly Headcheese Sign). This finding of areas of normal lung, high attenuation GGOs, and lucent regions of air trapping scattered throughout the lung is a specific, but not sensitive sign for fibrotic HP