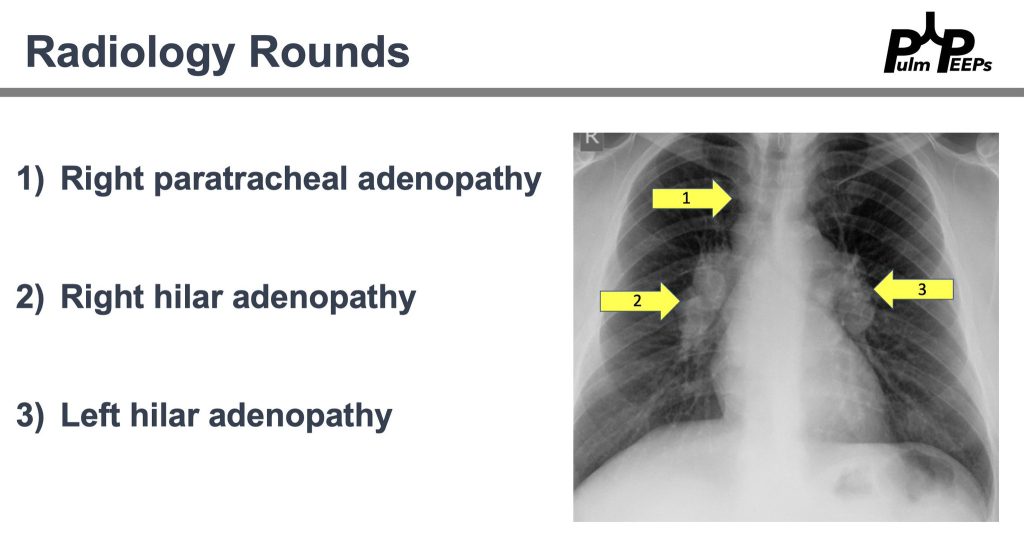
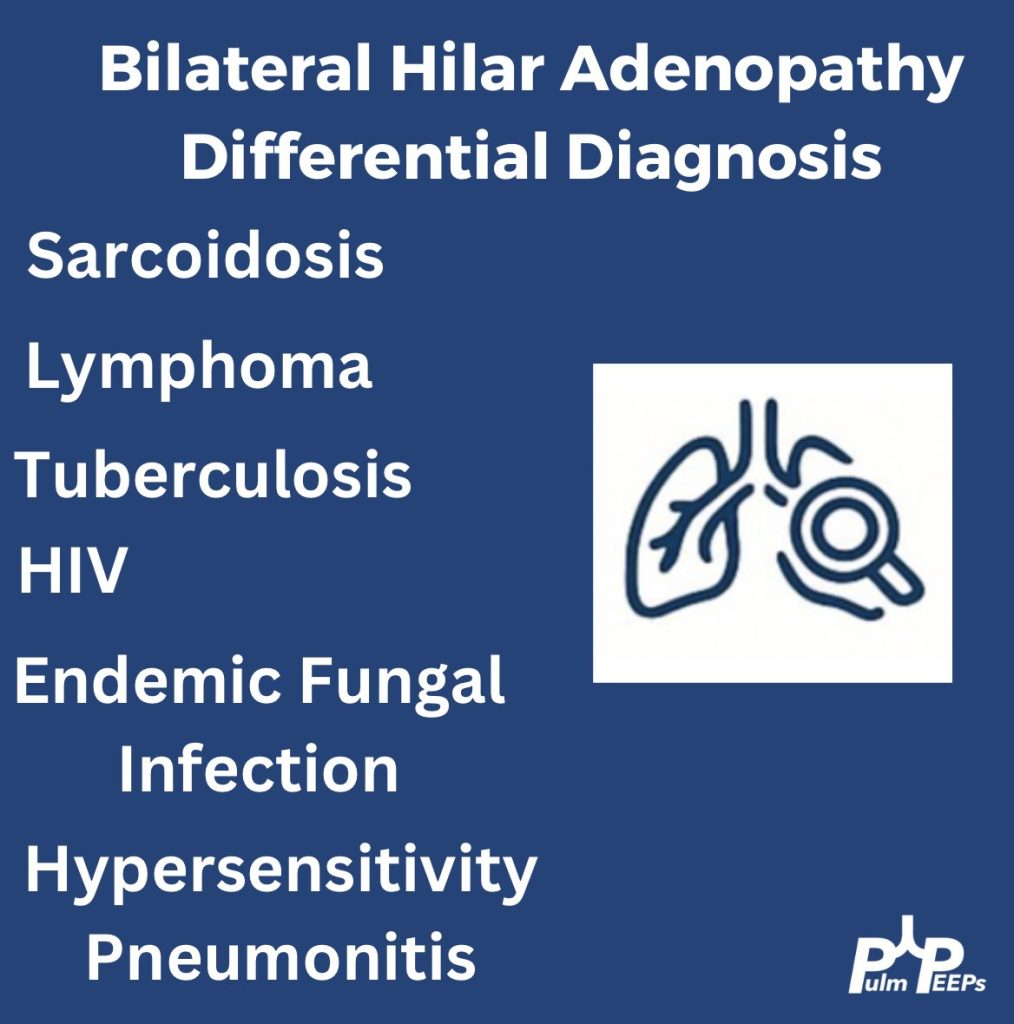
History and physical exam are essential. Here are a few can’t miss diagnoses when working up a young adult with bilateral hilar adenopathy.
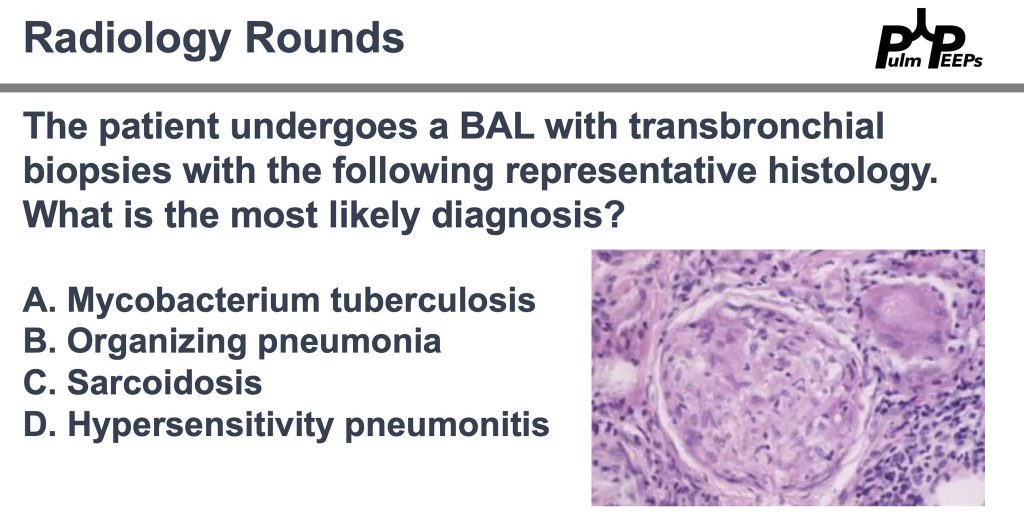
Pathology is consistent with a non-caseating granuloma. What is the most likely diagnosis?
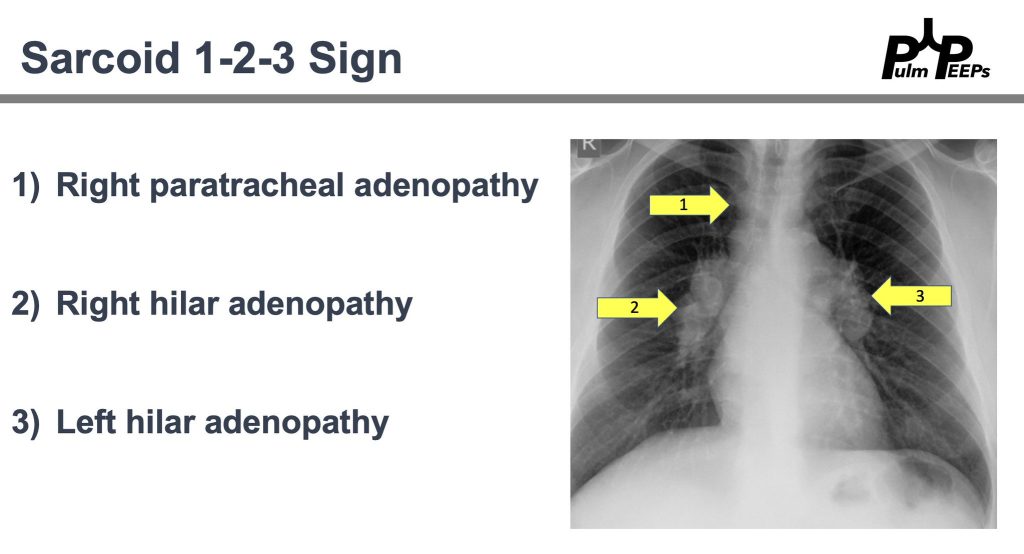
Imaging and pathology were consistent with sarcoidosis and after negative work-up for alternative causes. The patient will follow-up with outpatient pulmonary for sarcoidosis management. Don’t forget about the Sarcoid 1-2-3 sign!
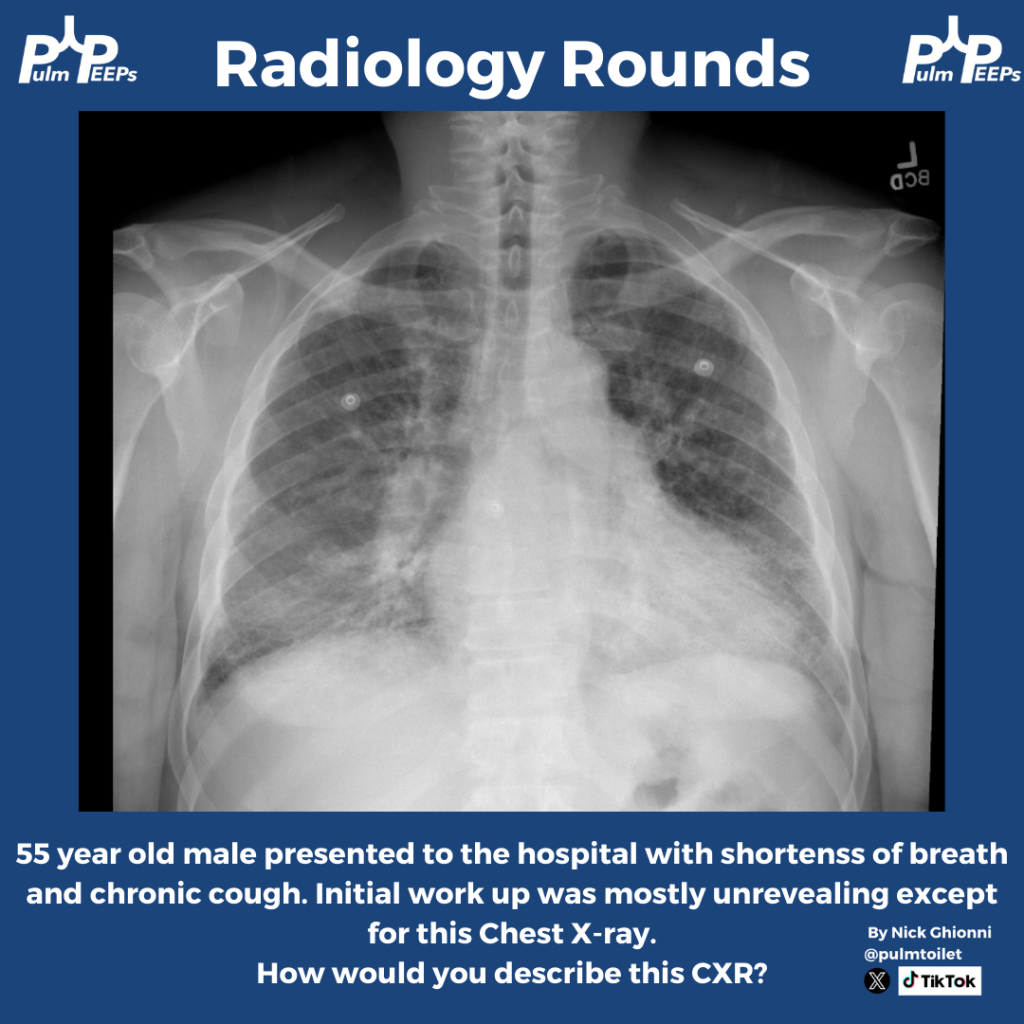
Time for another Radiology Rounds! This case is brought to you by our Associate Editor Nick Ghionni @pulmtoilet ! A 55 year old man presents to the hospital with progressive dyspnea and a chronic cough. Here is his initial CXR.
Further history and exam is taken and is notable for
Progressive dyspnea, especially with exertion
Has received courses of steroids and antibiotics in the past
Breeds pigeons
Tachypneic on exam, scattered rales, and rare faint wheeze
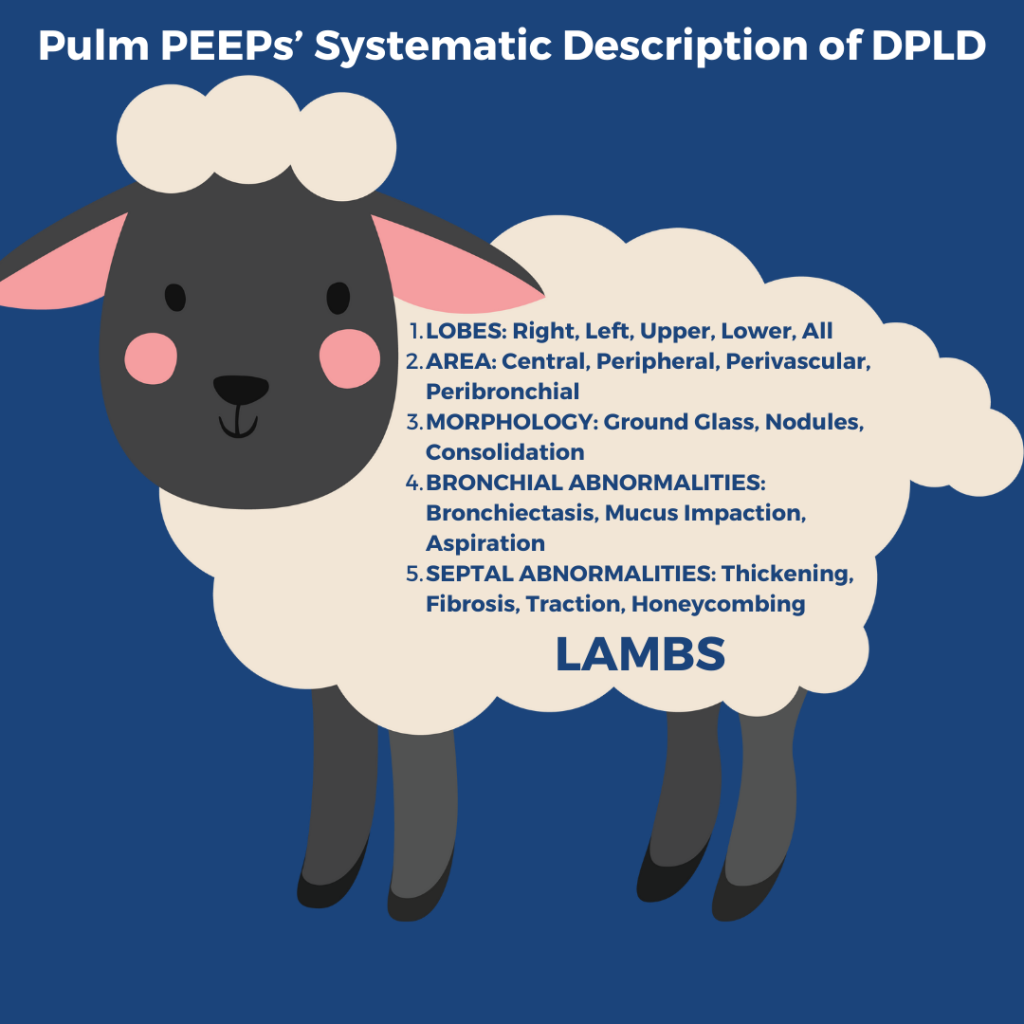
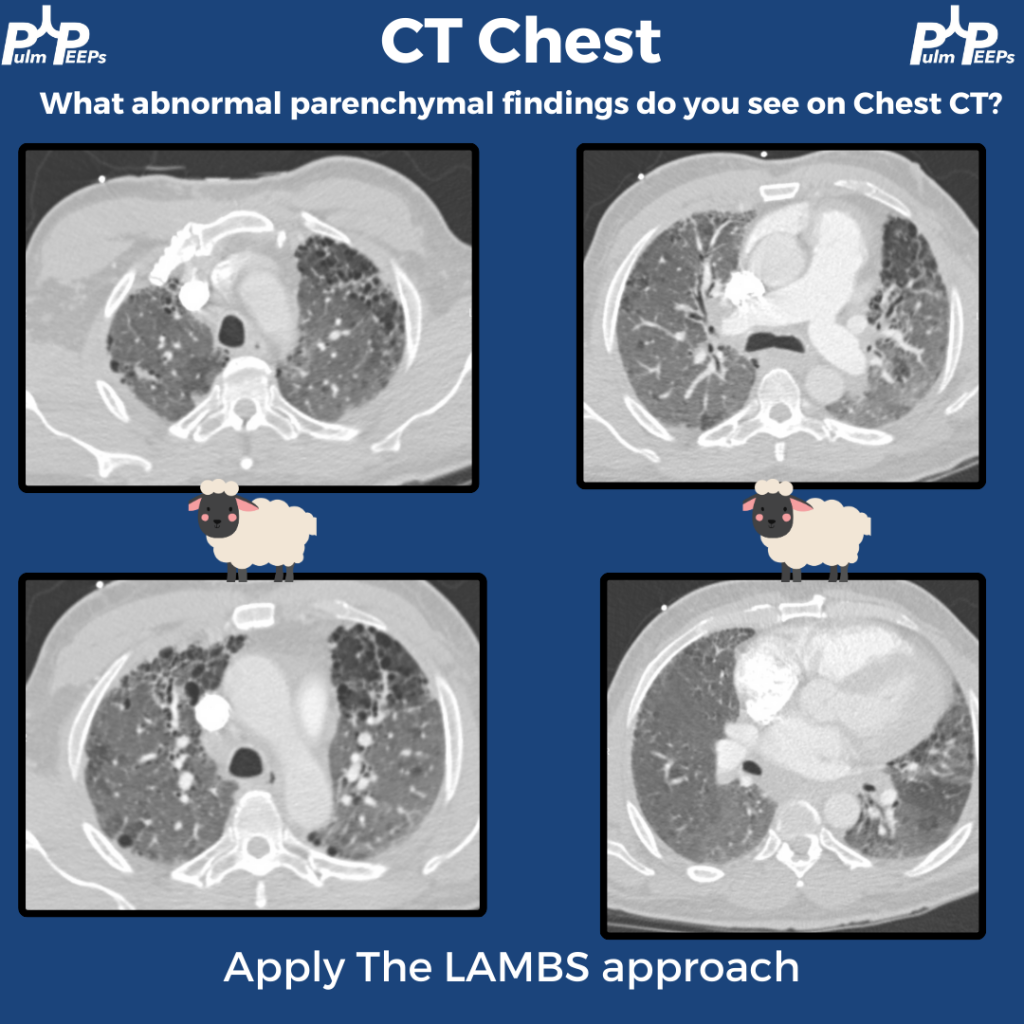
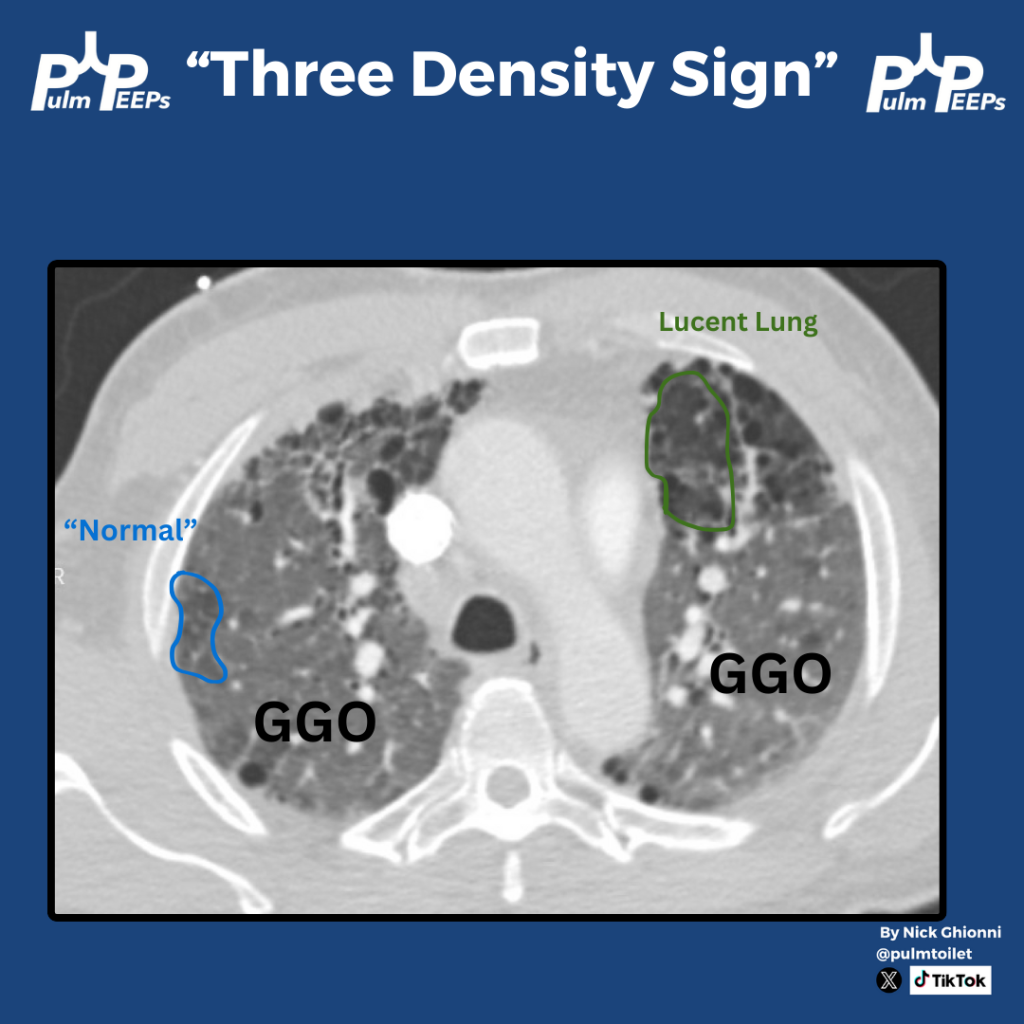
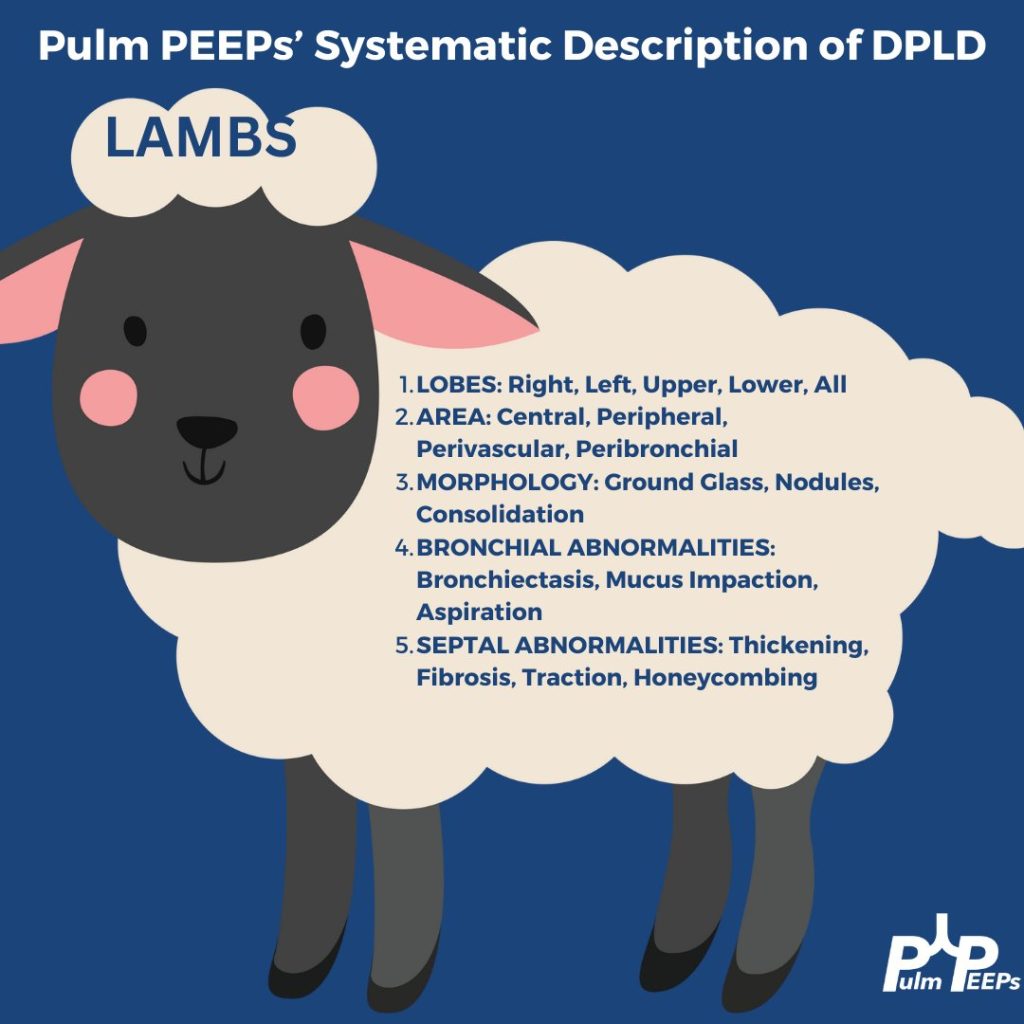
A high resolution, thin cut, CT w/out contrast inspiratory and expiratory, and prone and supine is performed. Here are some key images Remember to apply Pulm PEEPs’ LAMBS approach to reading CTs with diffuse parenchymal findings
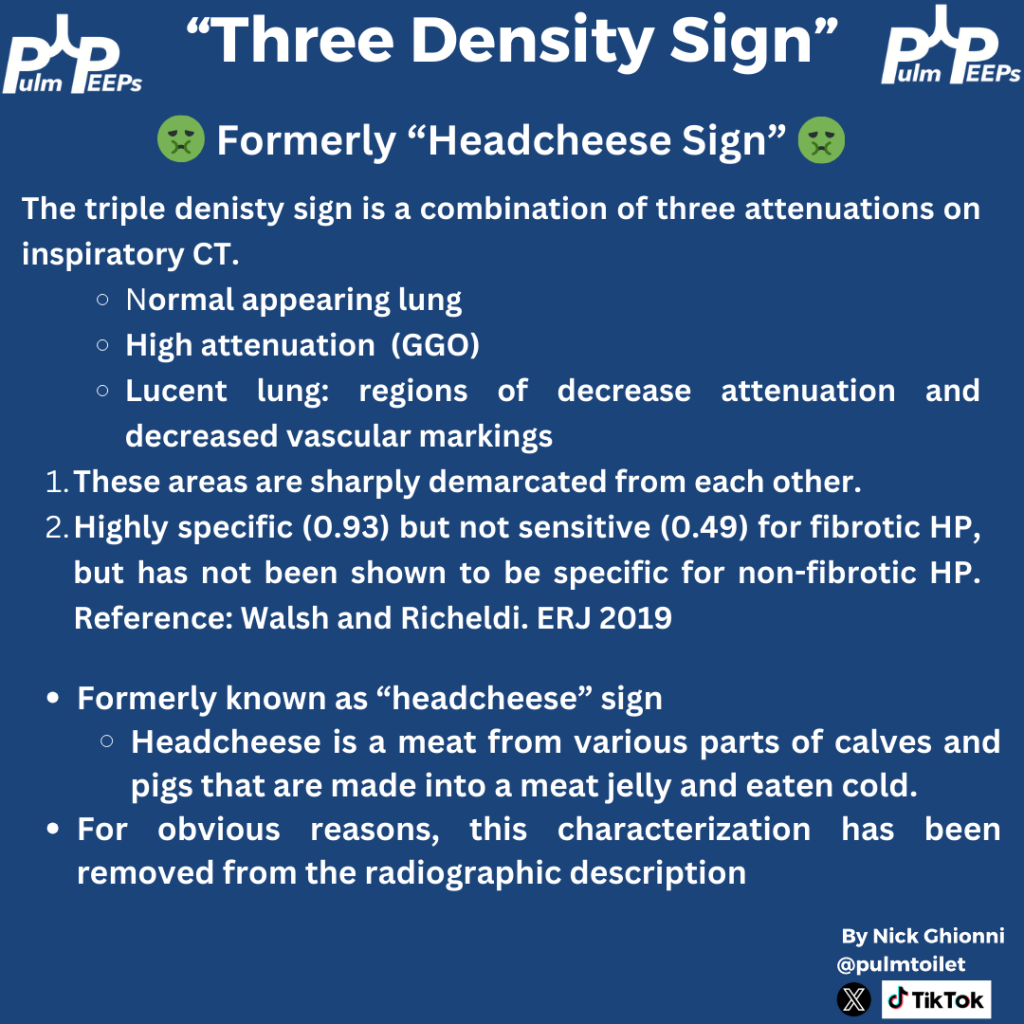
The CT scan shows an example of Triple Density Sign (formerly Headcheese Sign). This finding of areas of normal lung, high attenuation GGOs, and lucent regions of air trapping scattered throughout the lung is a specific, but not sensitive sign for fibrotic HP
We are excited to start the month off with a new #RadiologyRounds
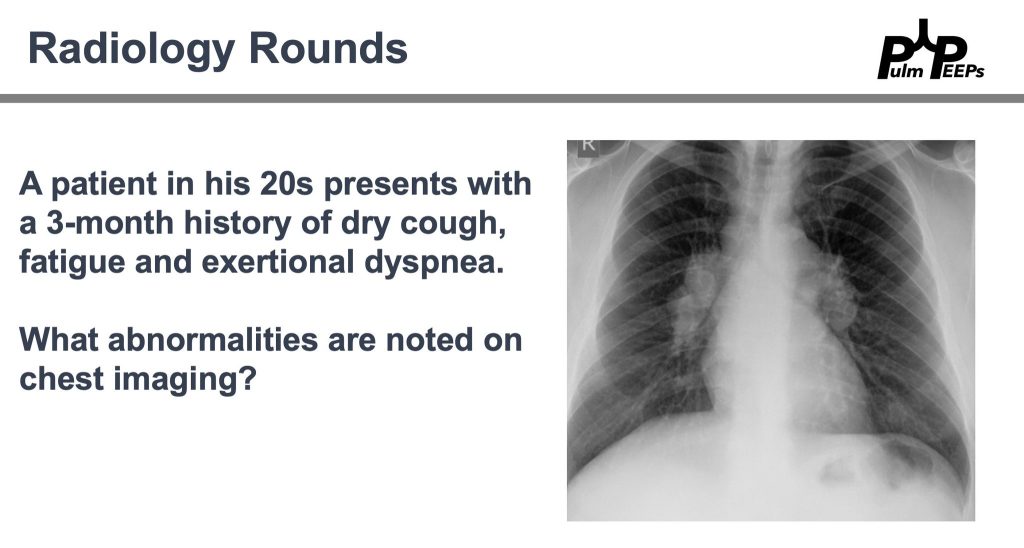
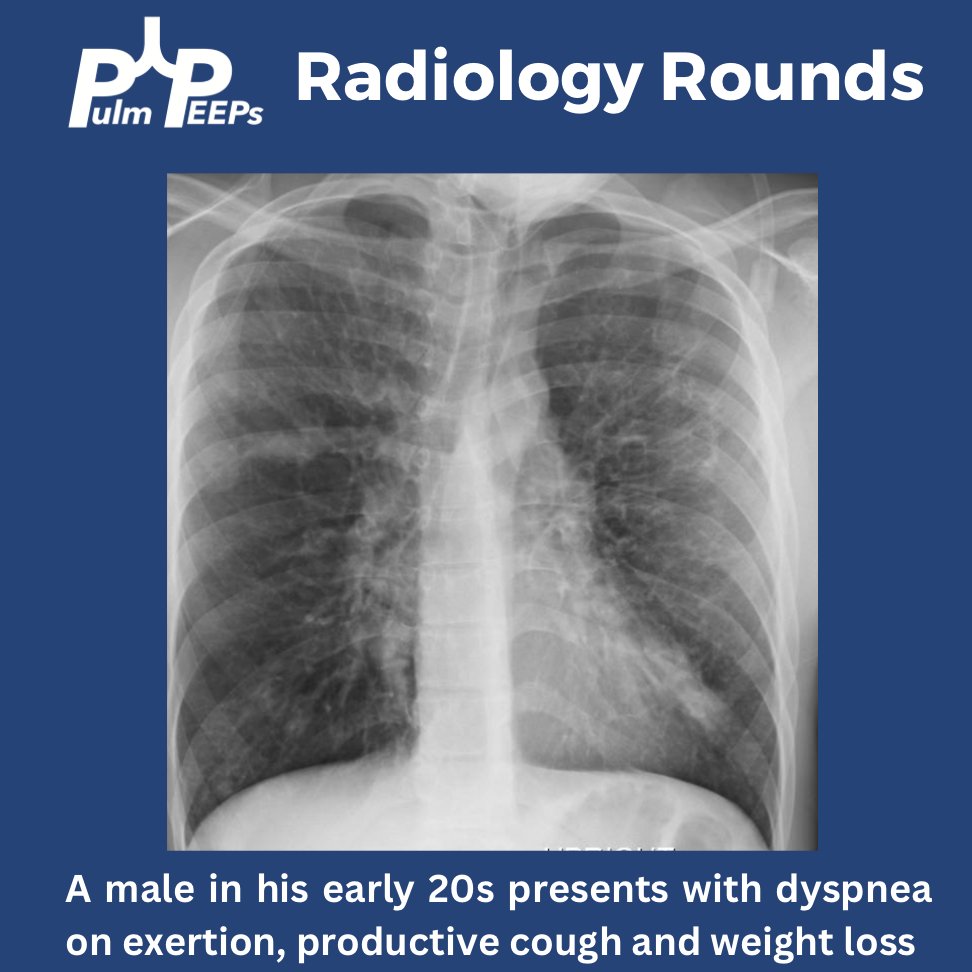
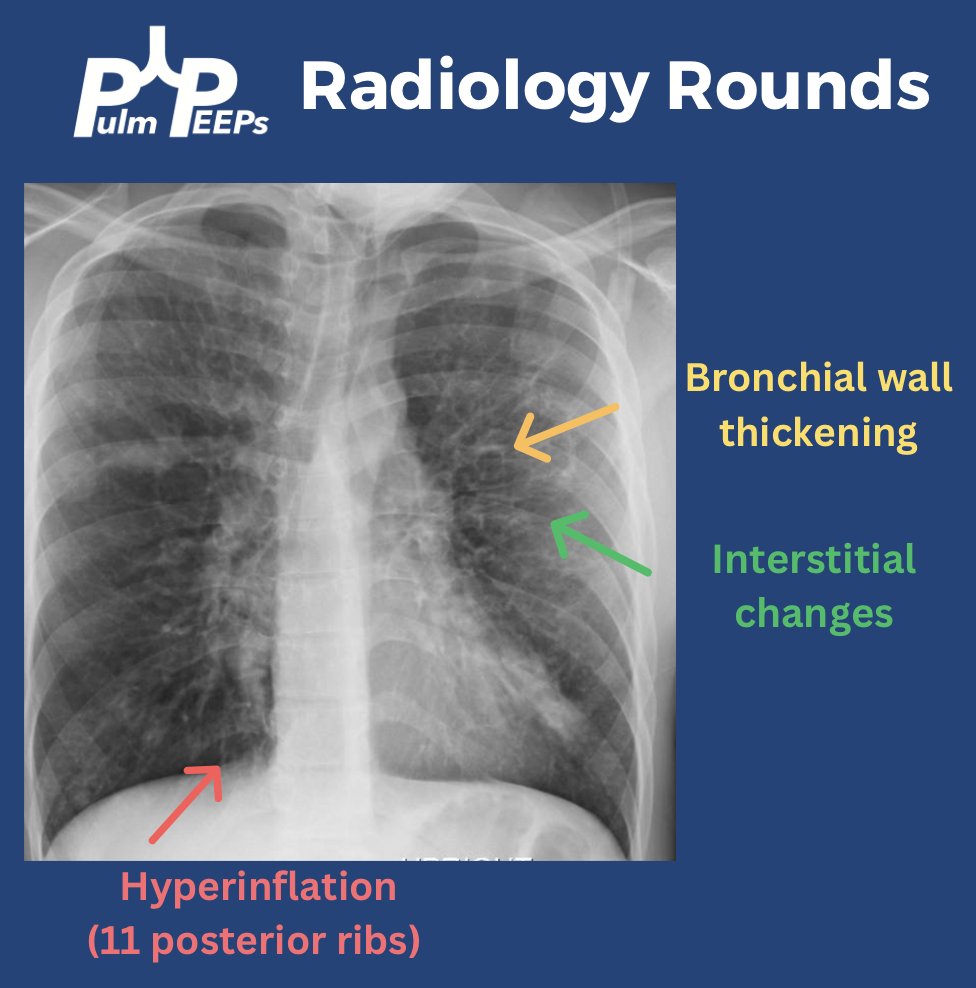
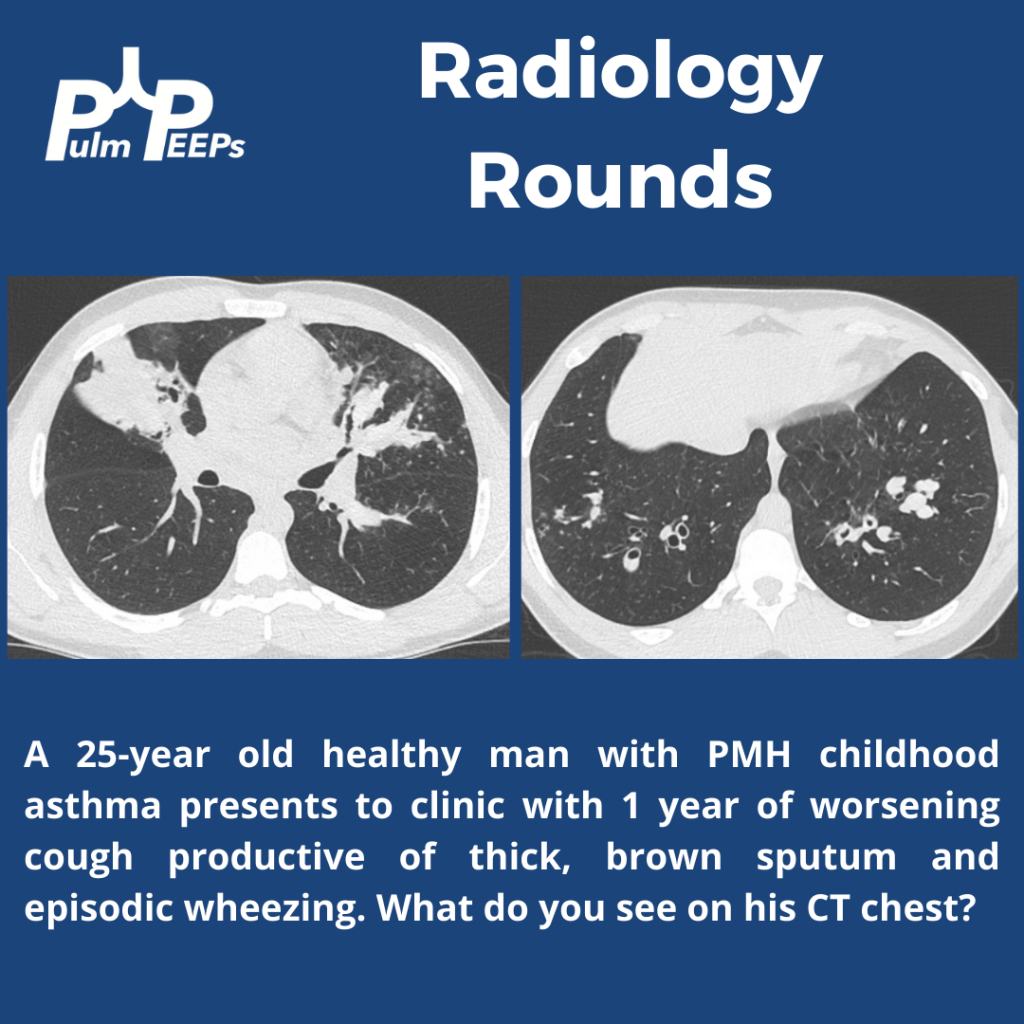
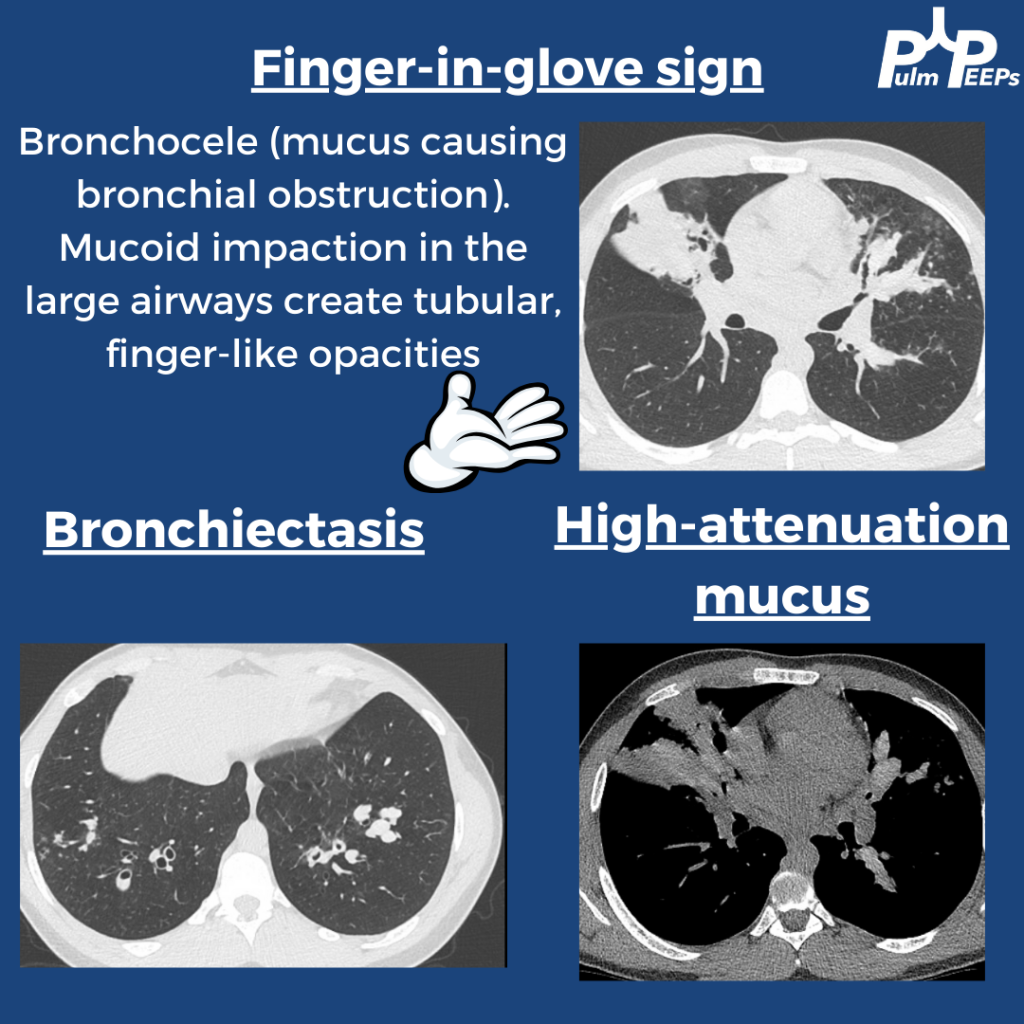
A young adult man in his 20s presents with dyspnea on exertion, productive cough, intermittent wheezing and general fatigue. A chest x-ray was obtained as part of his work-up.
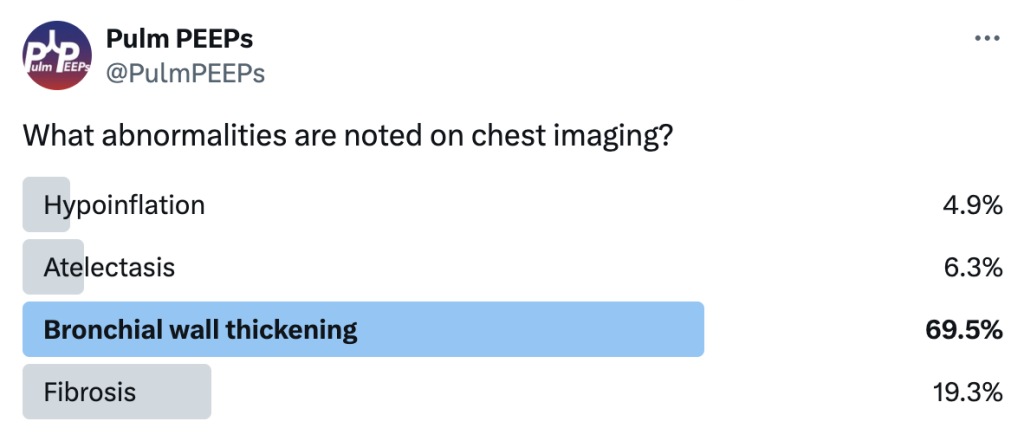
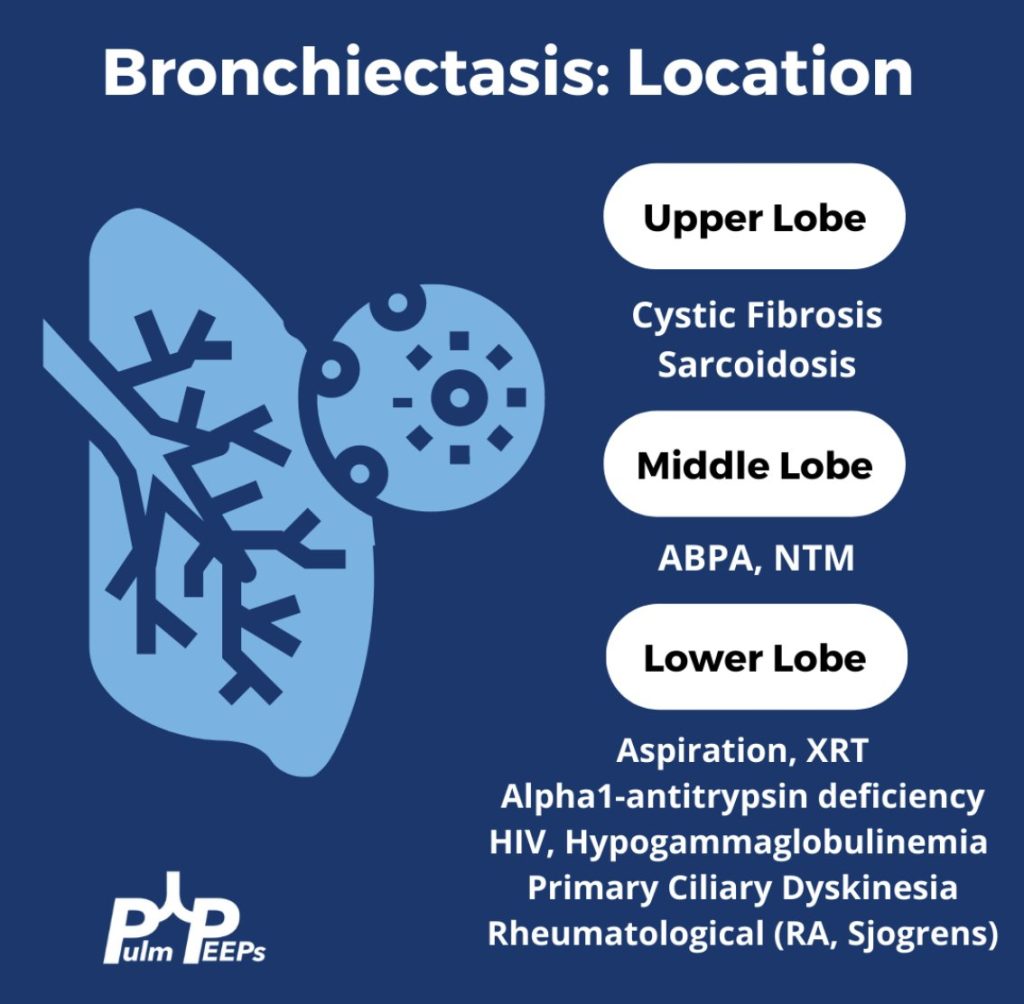
You can identify hyperinflation, interstitial changes and bronchial wall thickening on this image with concern for associated bronchiectasis
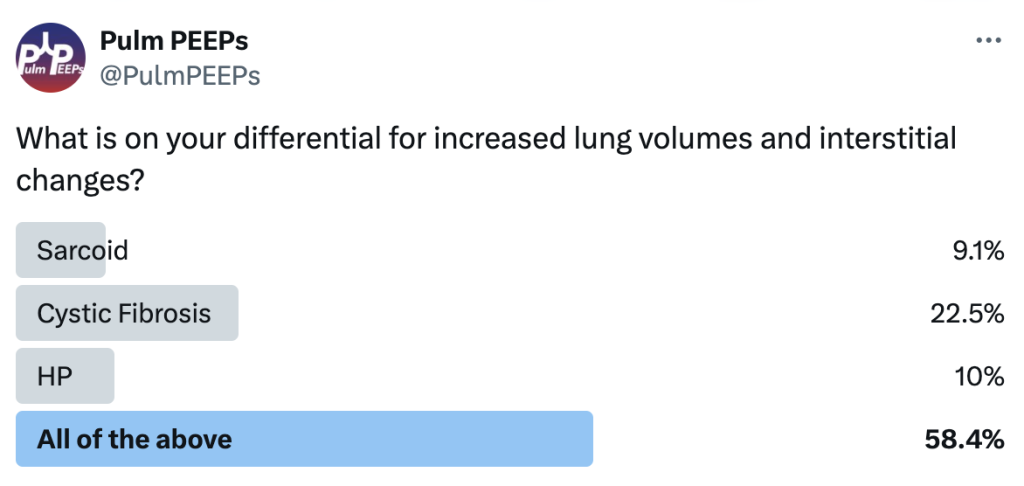
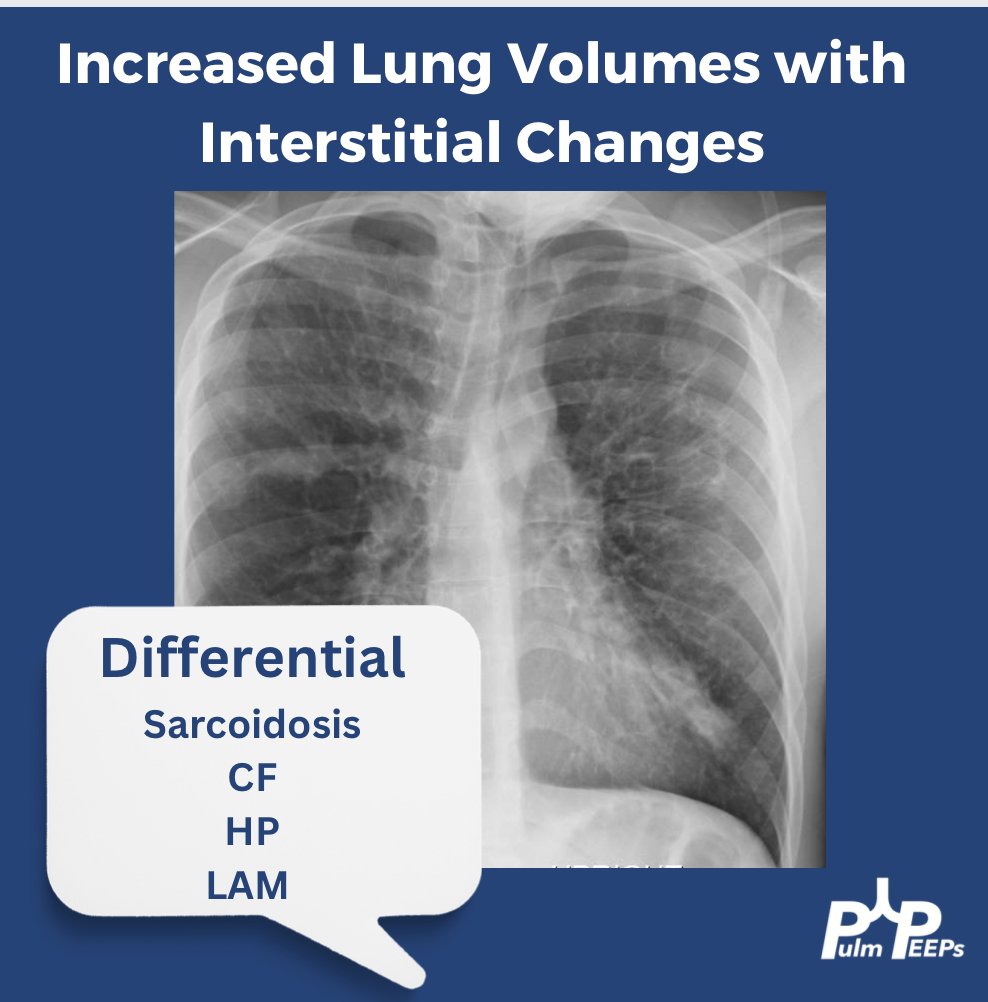
You should have Sarcoidosis, Cystic Fibrosis (CF), Hypersensitivity Pneumonitis (HP) and Lymphangioleiomyomatosis (LAM) on the differential
A CT chest is obtained given his abnormal chest x-ray and representative images are shown below
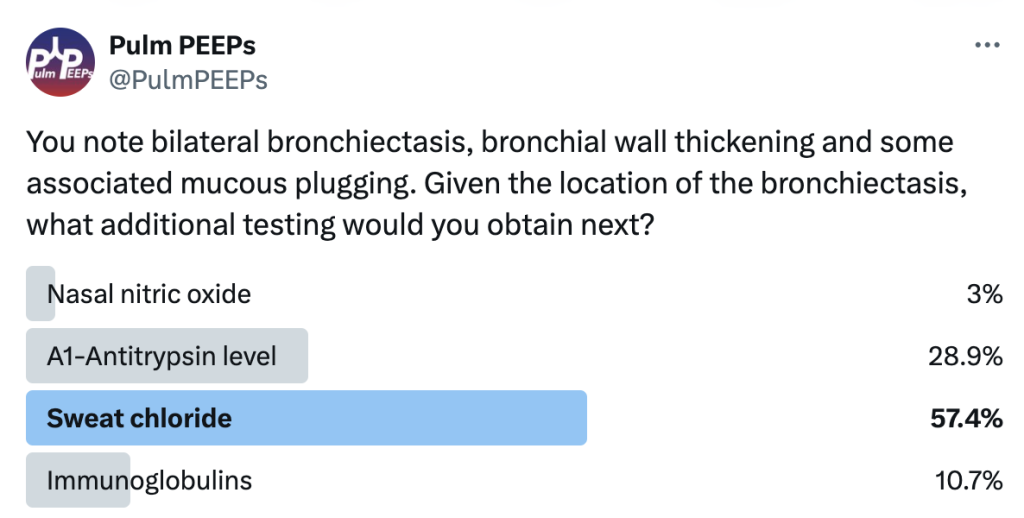
Given upper lobe bronchiectasis you are concerned for cystic fibrosis. A sweat chloride test is obtained and was elevated suggesting CF and further genetic testing was sent to confirm the diagnosis.
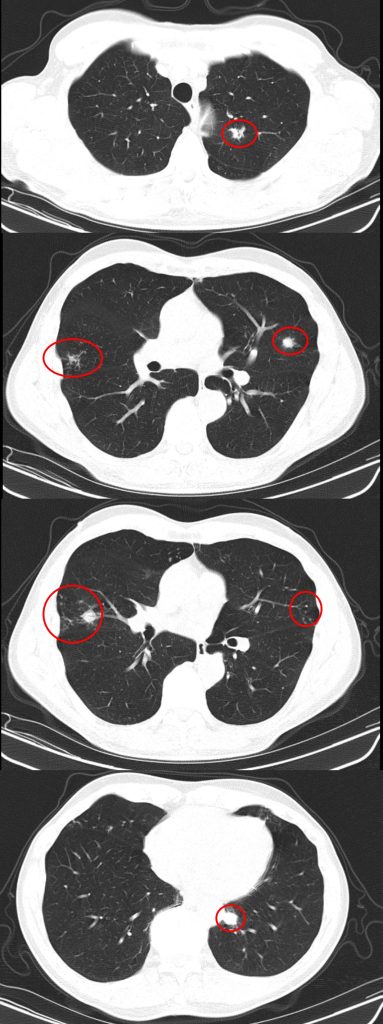
A #RadiologyRounds case with 3 different imaging modalities! A 65+ year old man never smoker, former marathoner has had 2-3 years of progressive non-productive, incessant cough with decreasing exercise tolerance. Some select CT scan slices are below
You are considering multiple etiologies including airway bleeding, pneumothorax, and hemothorax. You grab an ultrasound and perform a lung / pleural POCUS. Here is what you see
The long POCUS shows an area of lung sliding and an area without any lung sliding. This is called lung point and is diagnostic of a pneumothorax. To get a better look at this, you can use M-mode.
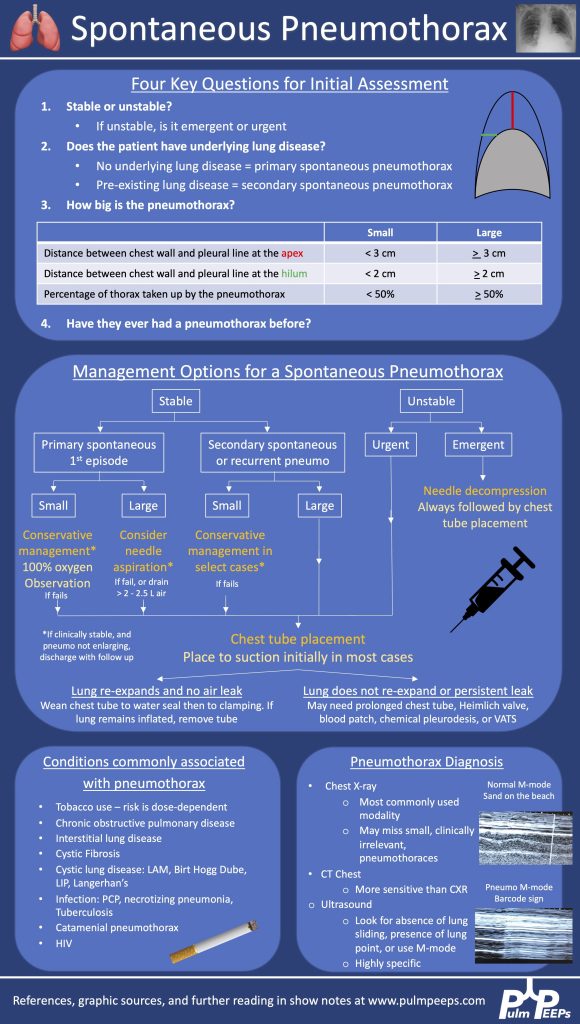
A CXR confirmed the finding of a pneumo. He was trialed on 100% oxygen but repeat CXR showed the pneumothorax was expanding. He had a chest tube placed with re-expansion of his lung and no air leak. It was able to be removed the next morning without incident
Here is our algorithm for pneumothorax!
Both BAL and tbbx returned positive for MAI complex. He was HIV neagative. Given his persistent and bothersome symptoms, he was started on treatment for pulmonary MAC with a macrolide, ethambutol and a rifamycin with plan for 6 months of therapy. He improved with this
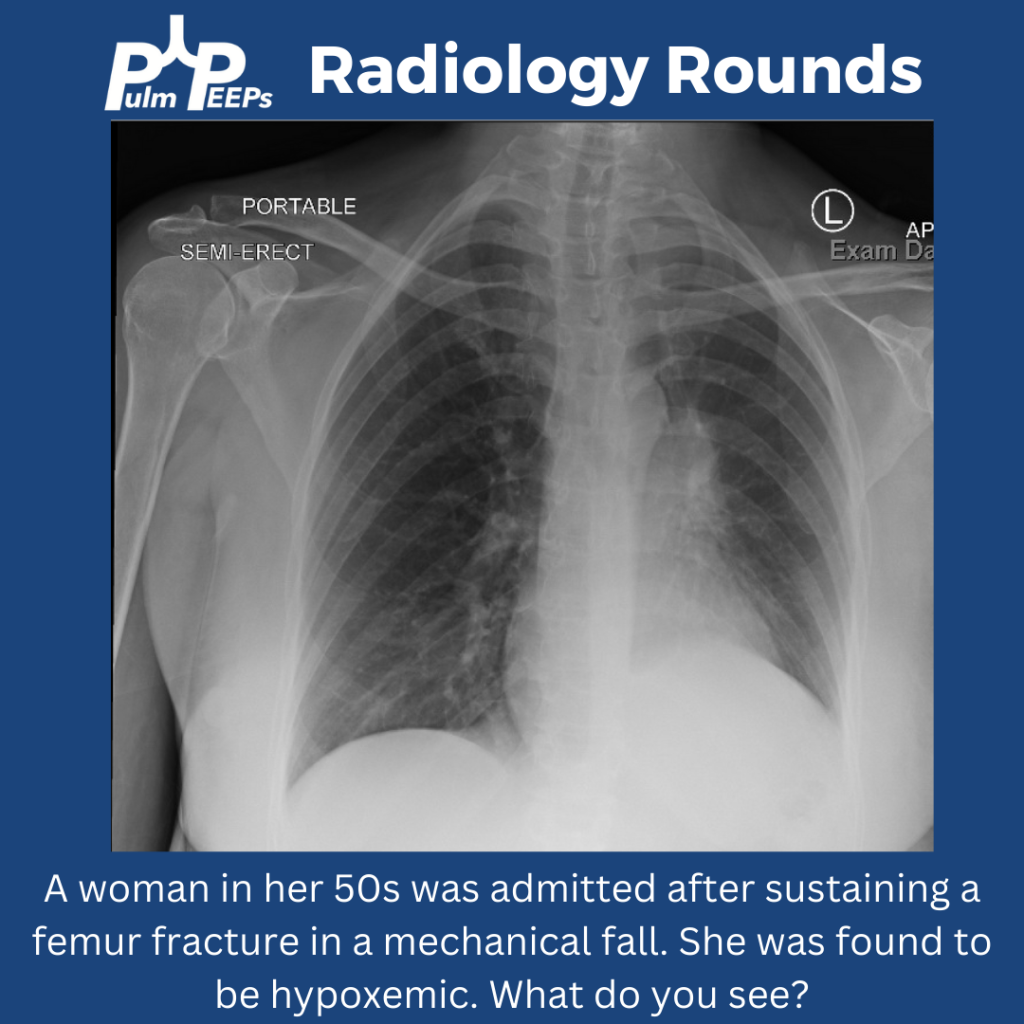
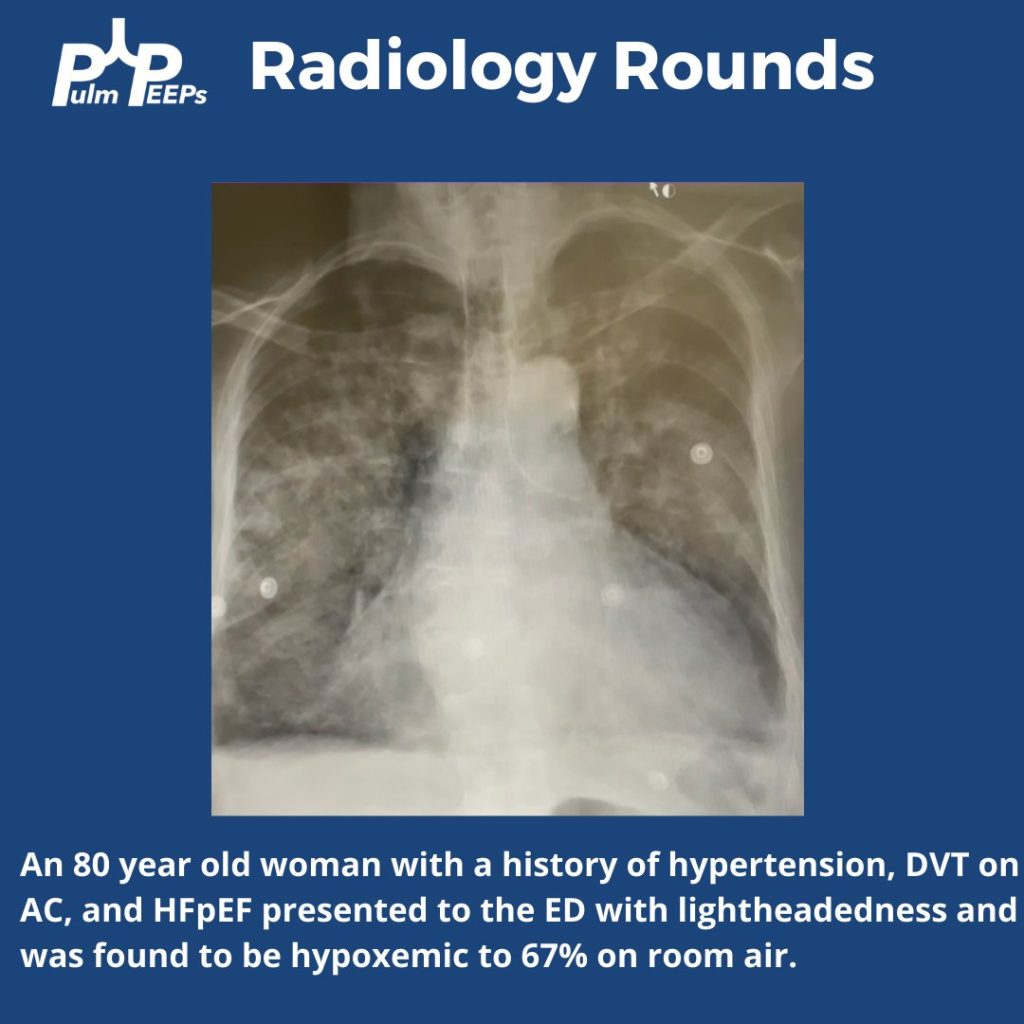
As we approach the end of the year, we know that the hospital and clinic keep on rolling, so here is a CXR and pulmonary differential based #RadiologyRounds if you’re on for the holiday blocks A woman in her 50s has hypoxemia after being admitted with a femur fracture
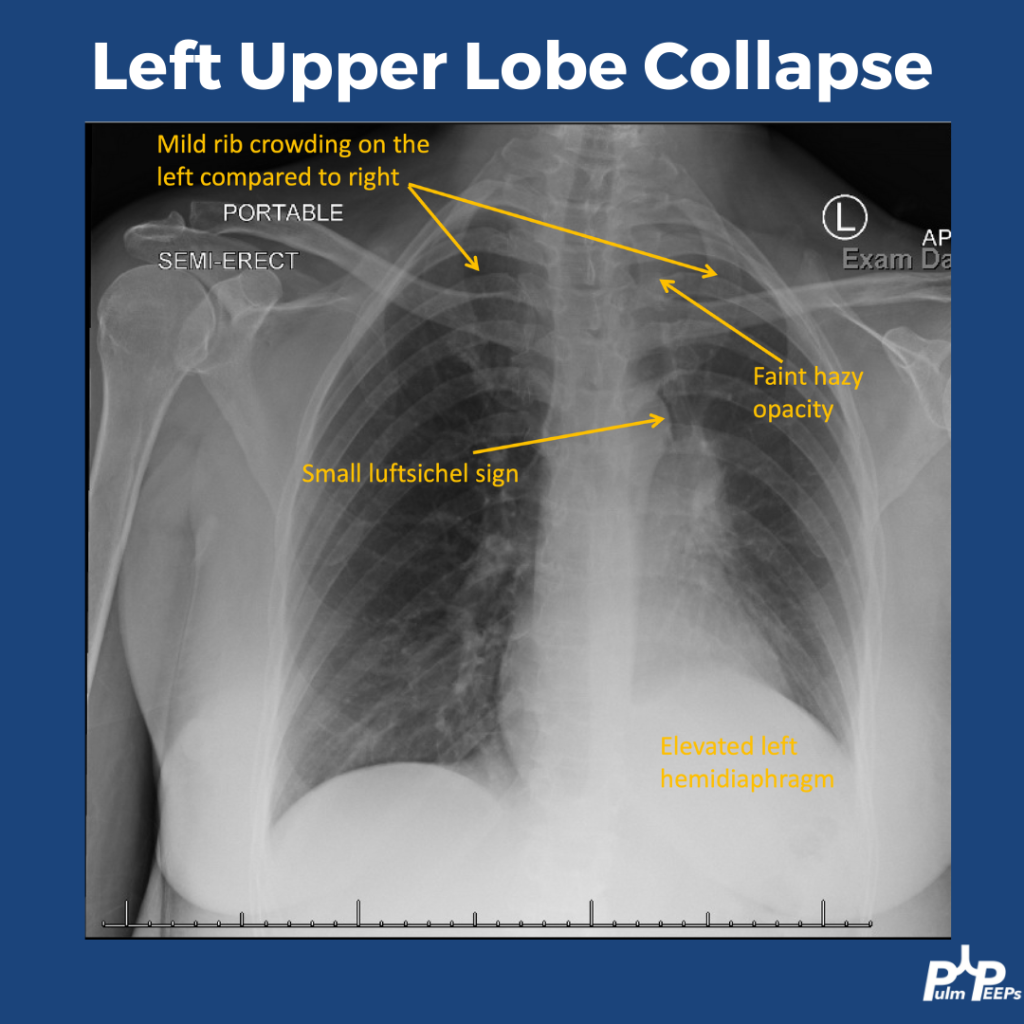
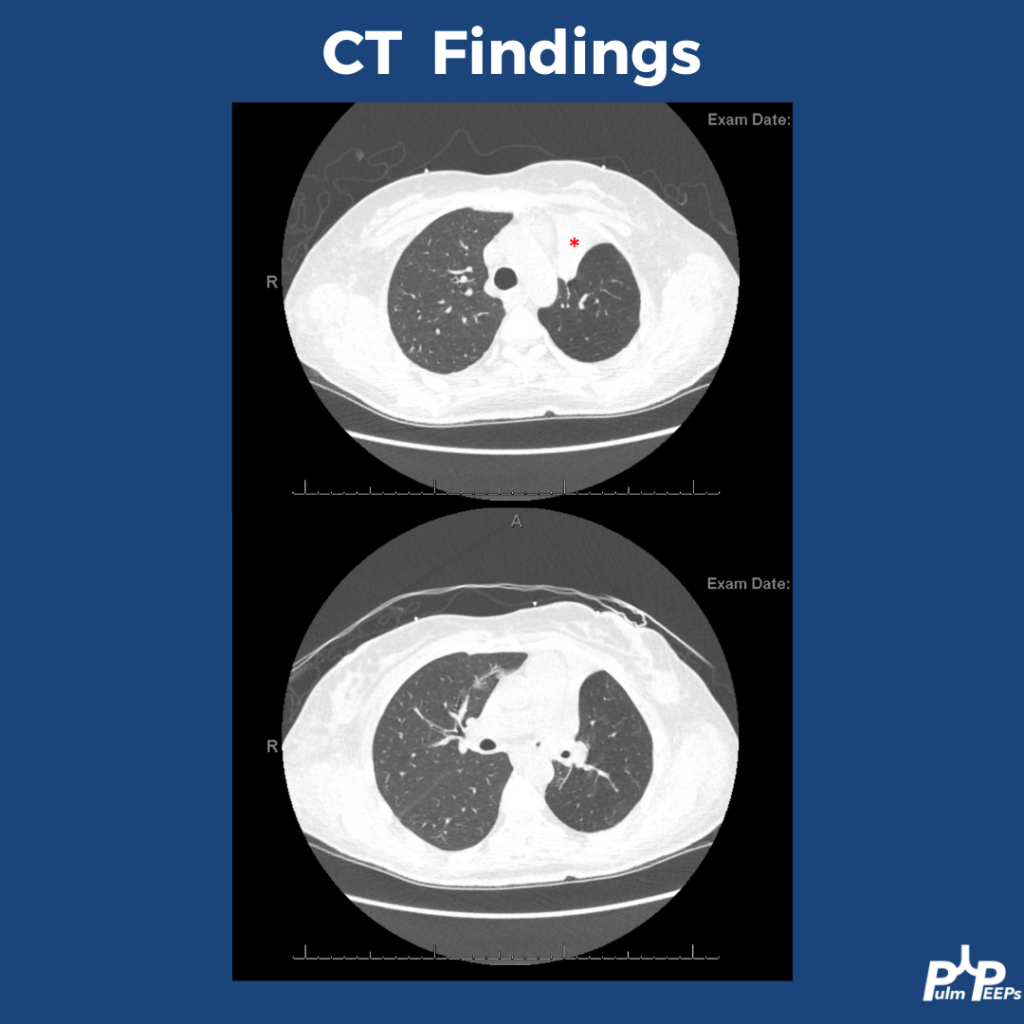
The CXR shows signs of a left upper lobe collapse. The upper lungs should be the most lucent, with increased opacity as you go down. LUL collapse can be subtle, but you can see increased haziness at the lung apex. There is also rib crowding and left hemidiaphragm elevation. You can also see a small luftsichel sign. Luftsichel sign is a thin strip of air that can be seen between the collapsed LUL and the superior mediastinum created by the still-aerated superior segment of the lower lobe. The collapse is better appreciated on CT.
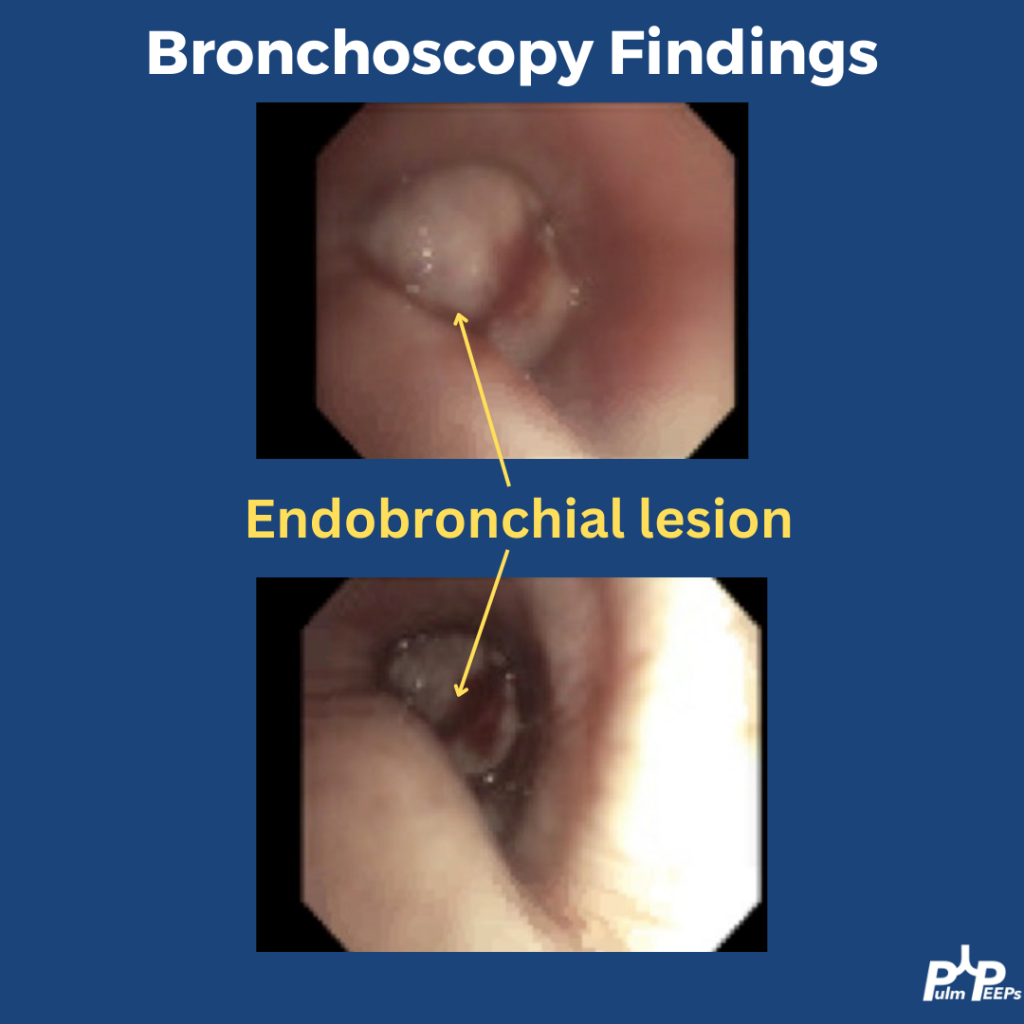
Bronchoscopy was performed to investigate the etiology of the lobar collapse. On the bronchoscopy there was an endobronchial lesion completely occluding the left upper lobe bronchus. The mass was biopsied and sent for histopathology
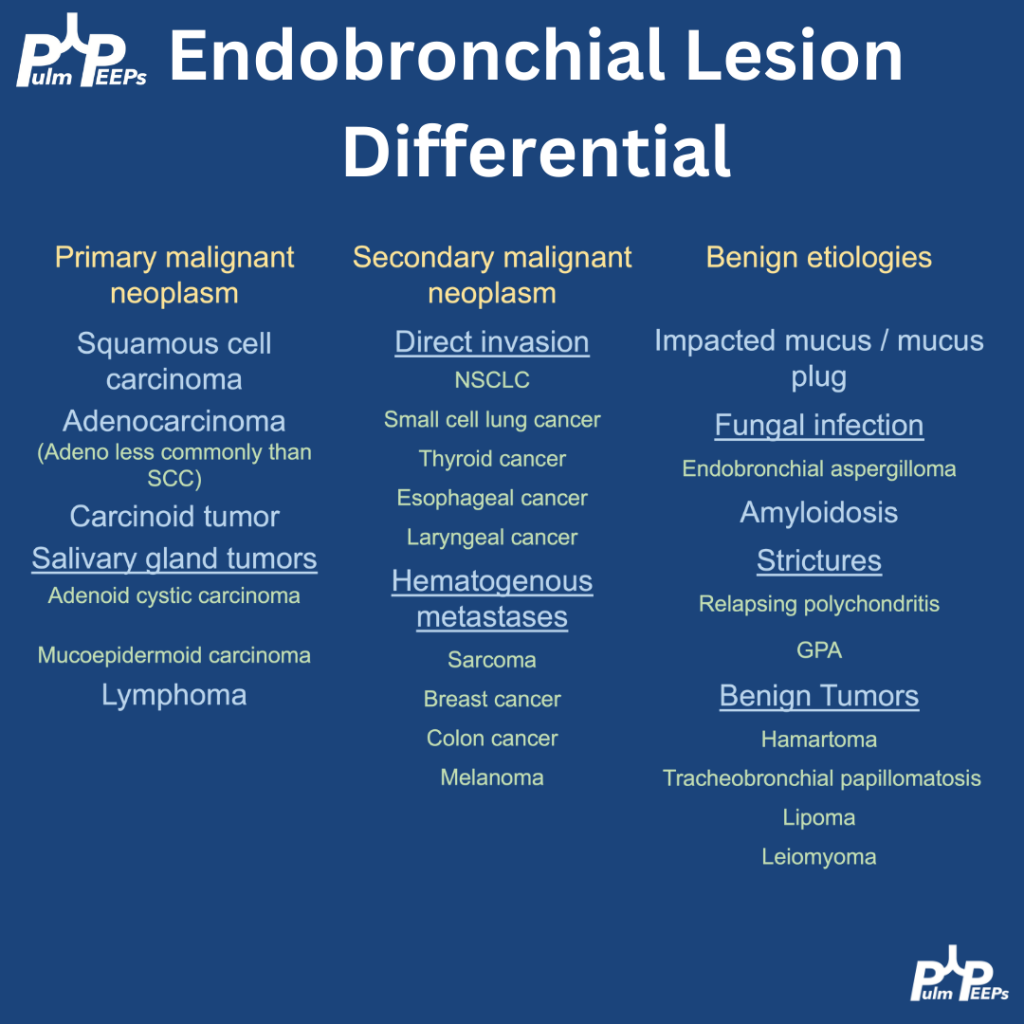
Endobronchial lesions can be malignant or benign, and within malignancy then can be primary or secondary. This patient had no clinical signs of pneumonia and no clear reason to mucus plug so malignancy was top of the differential. Here are differential considerations:
The pathology returned positive for a carcinoid tumor, which can typically arise as endbronchial lesions. PET/CT showed only local disease (femur fracture unrelated), and she is planned for rigid bronchoscopy with laser therapy and corecath ablation for definitive resection.
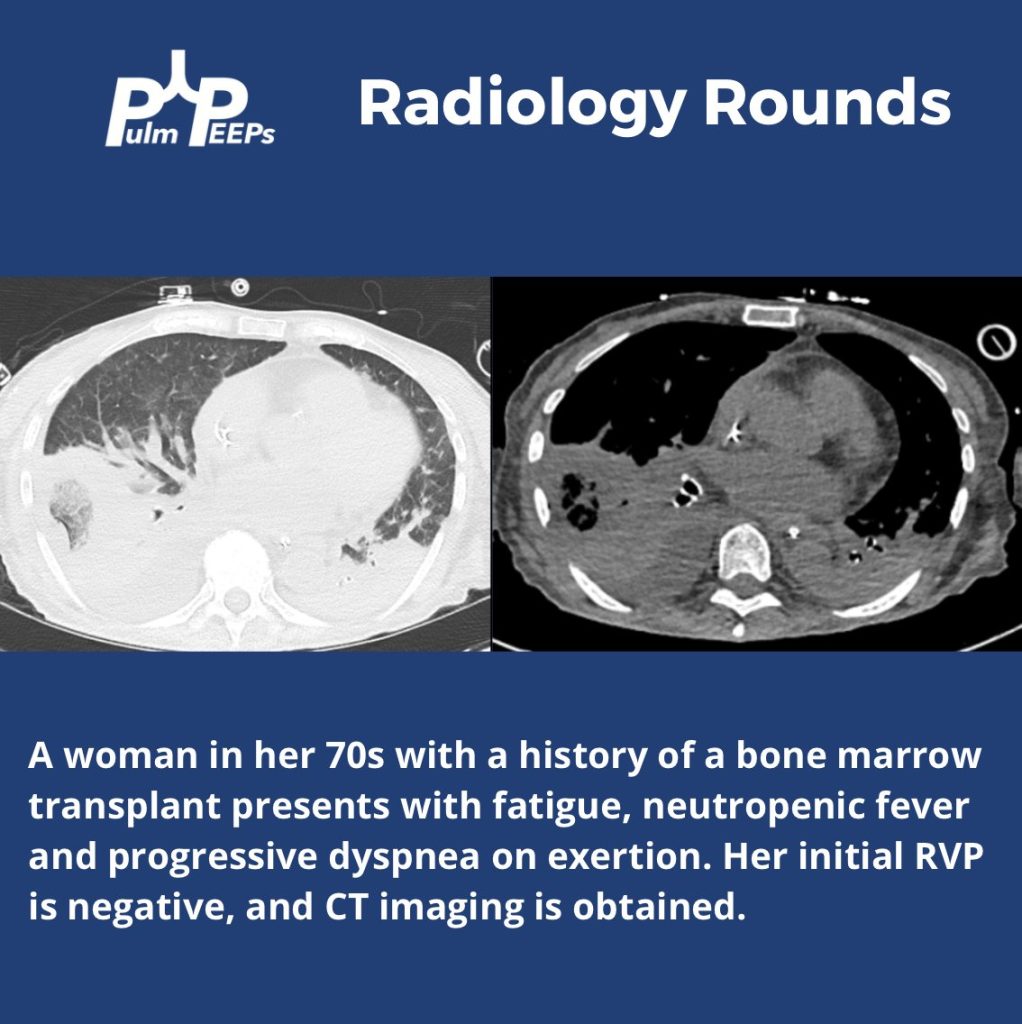
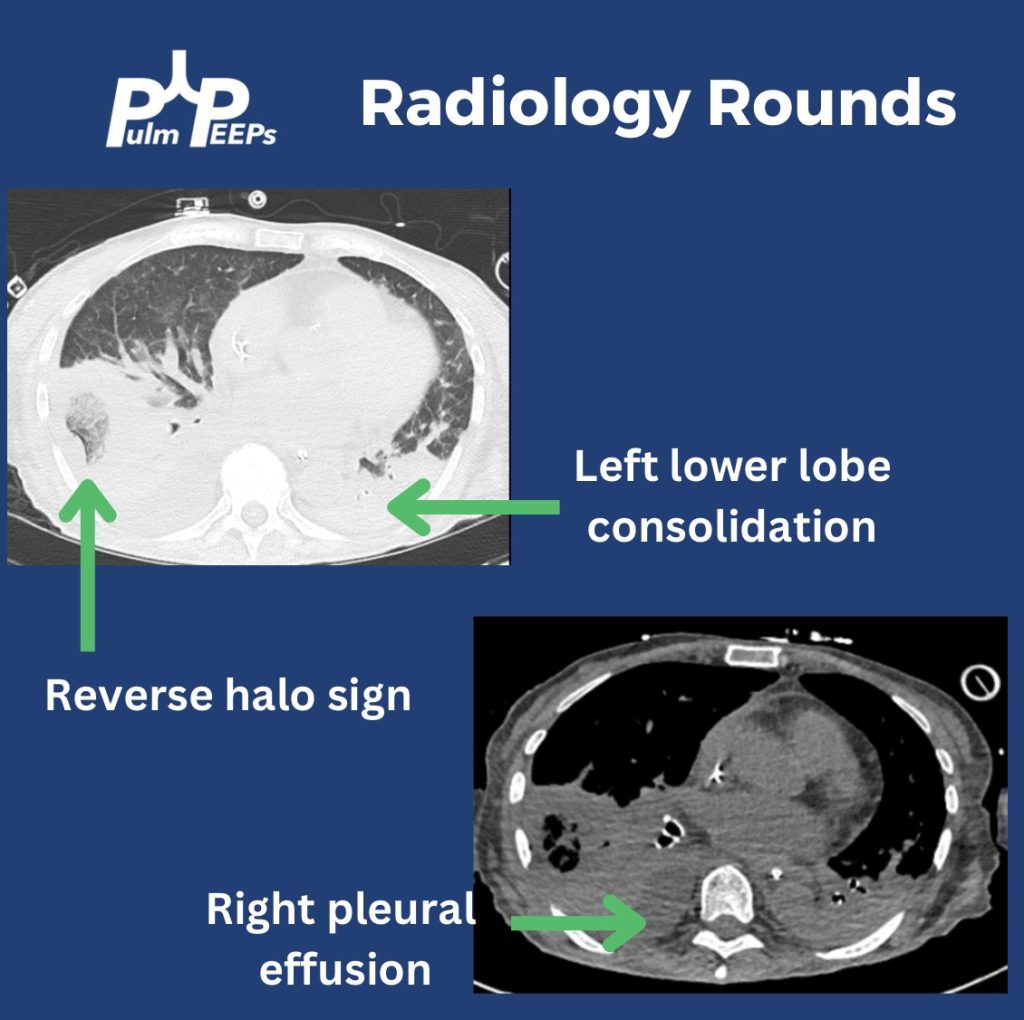
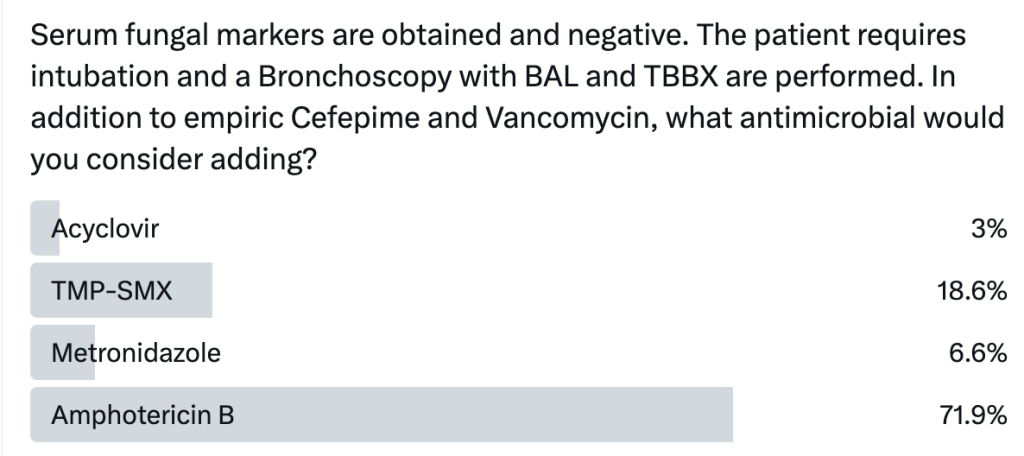
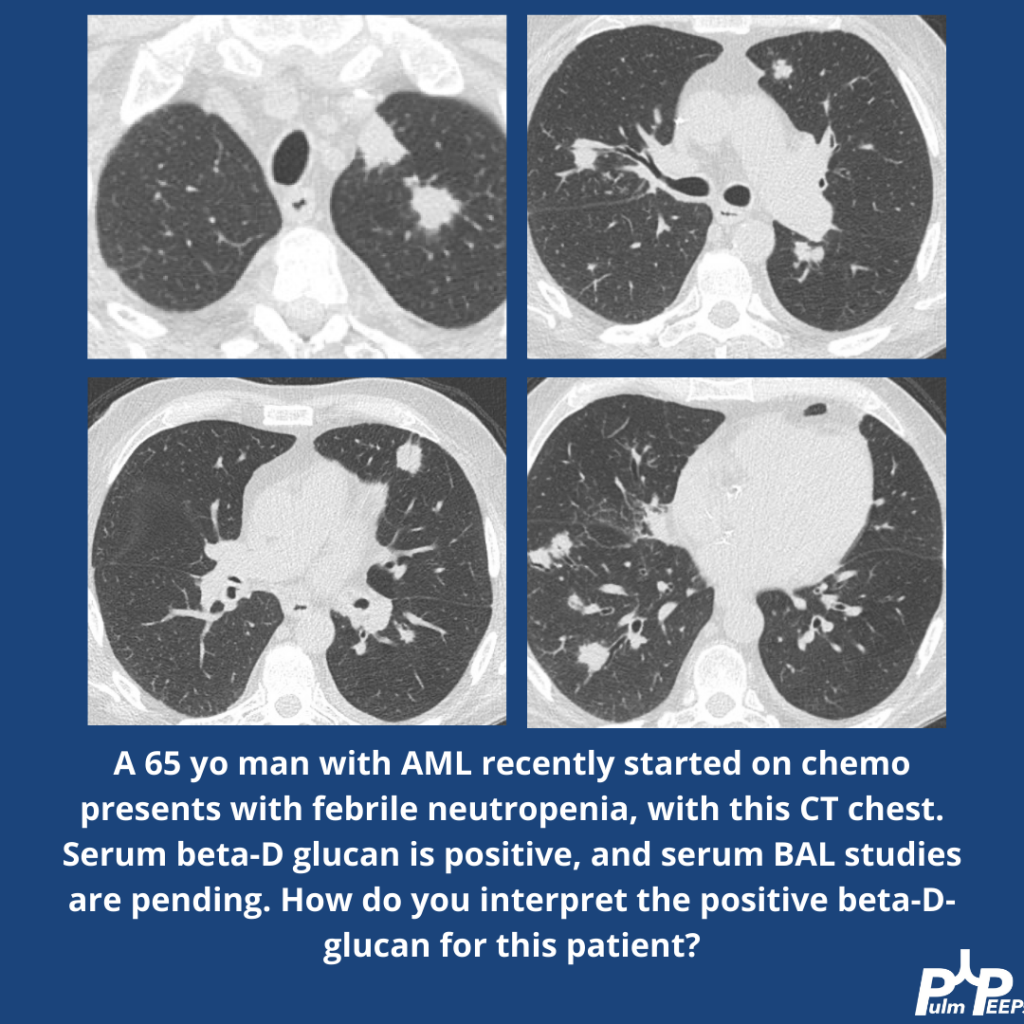
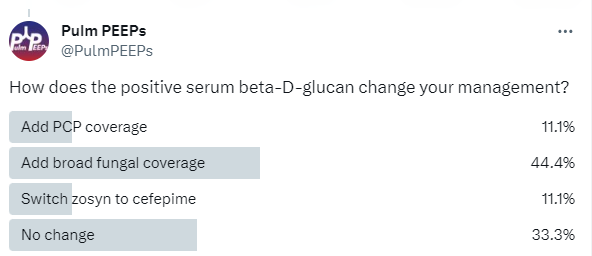
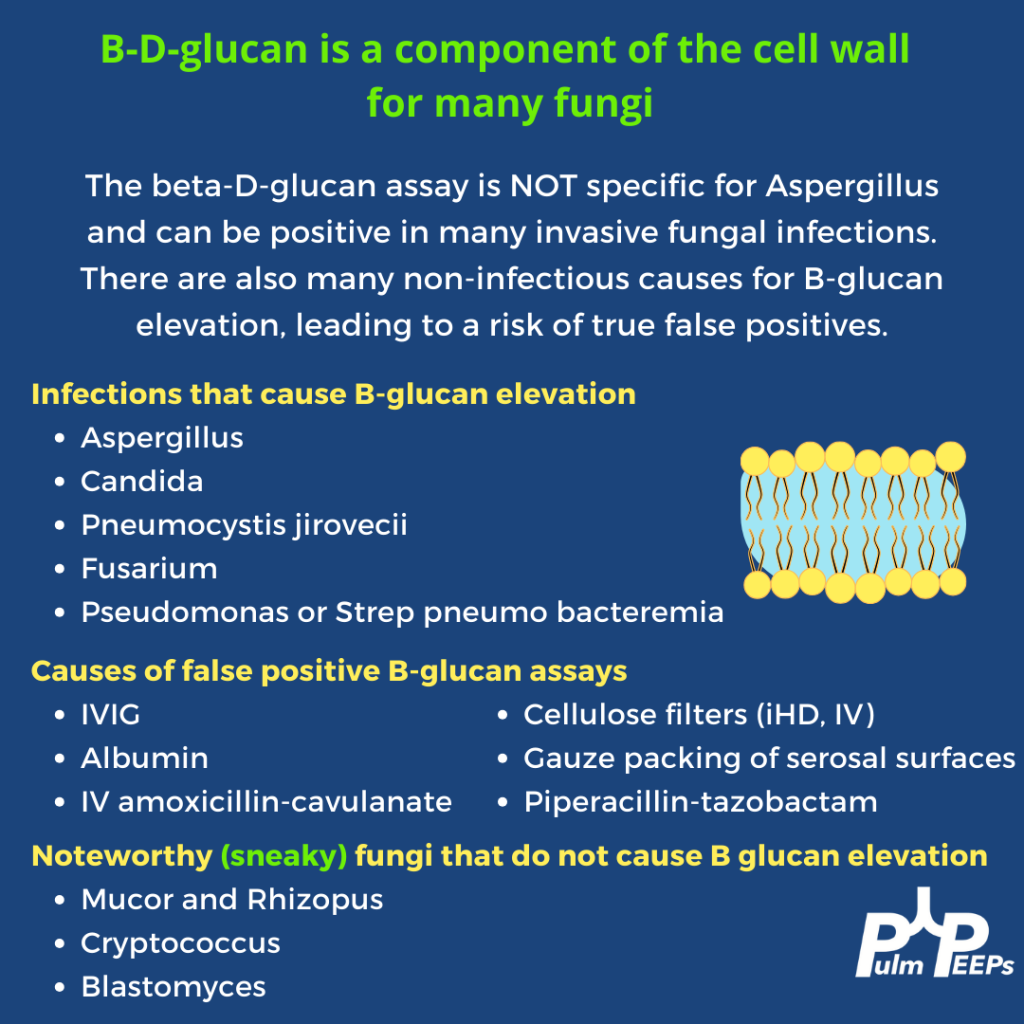
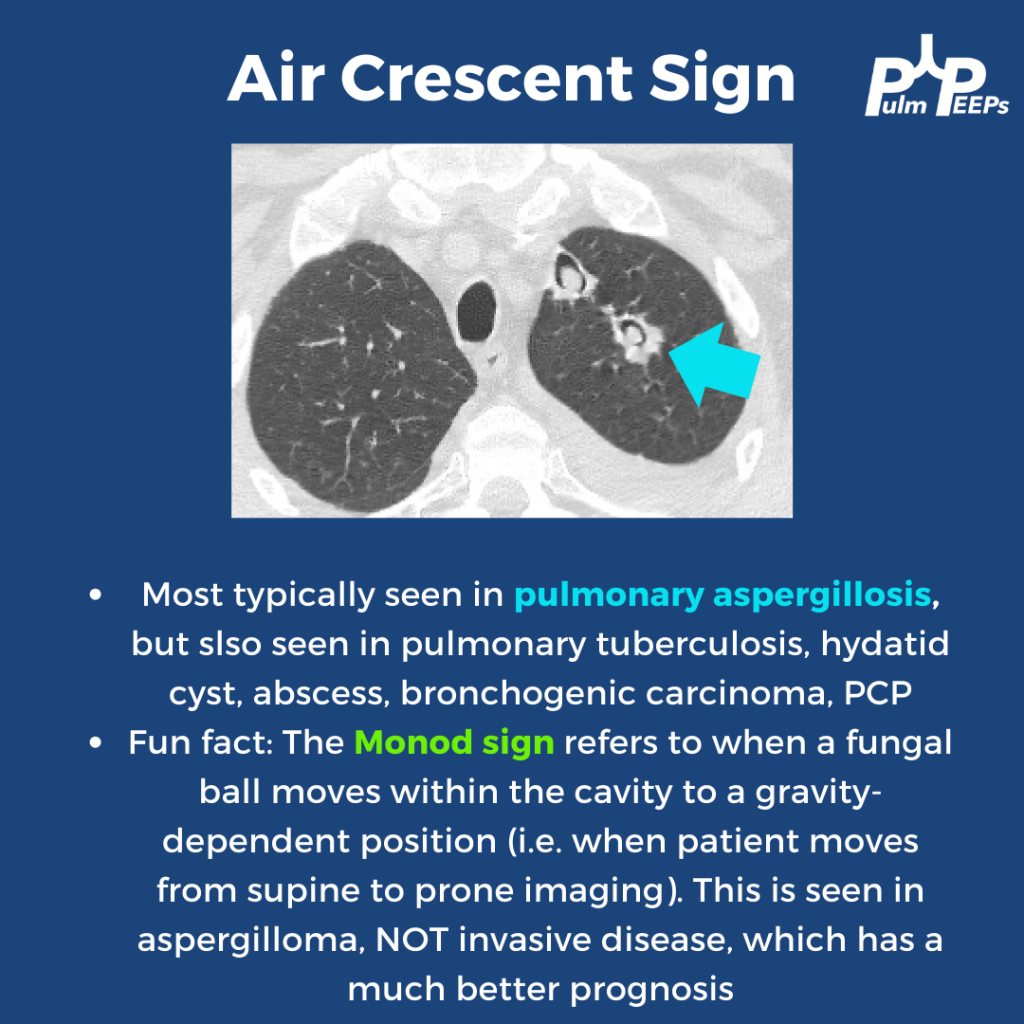
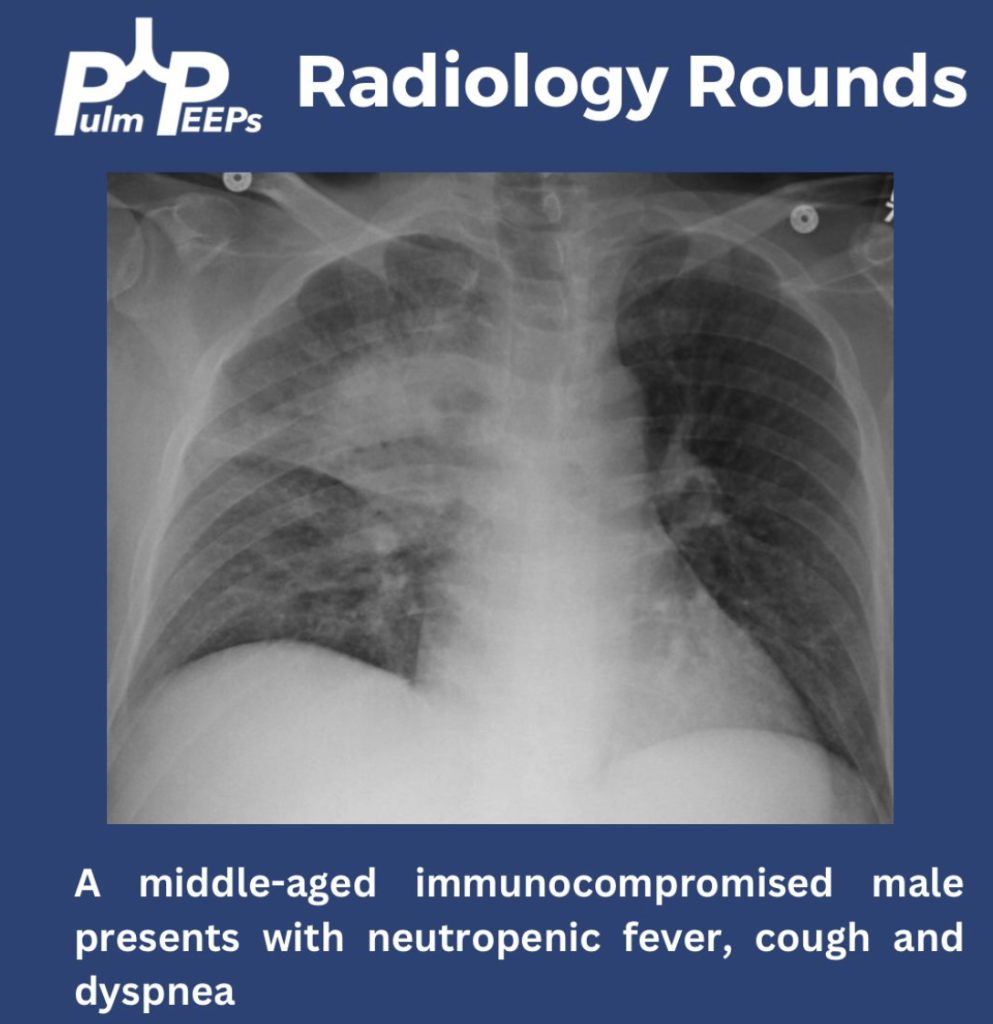
We’re back with another #RadiologyRounds by Pulm PEEPs Associate Editor Tess Litchman. An immunosuppressed 65-year-old man presents with neutropenic fever. He is started on empiric broad-spectrum antibiotics with vancomycin and zosyn. Serum beta-D-glucan is positive.
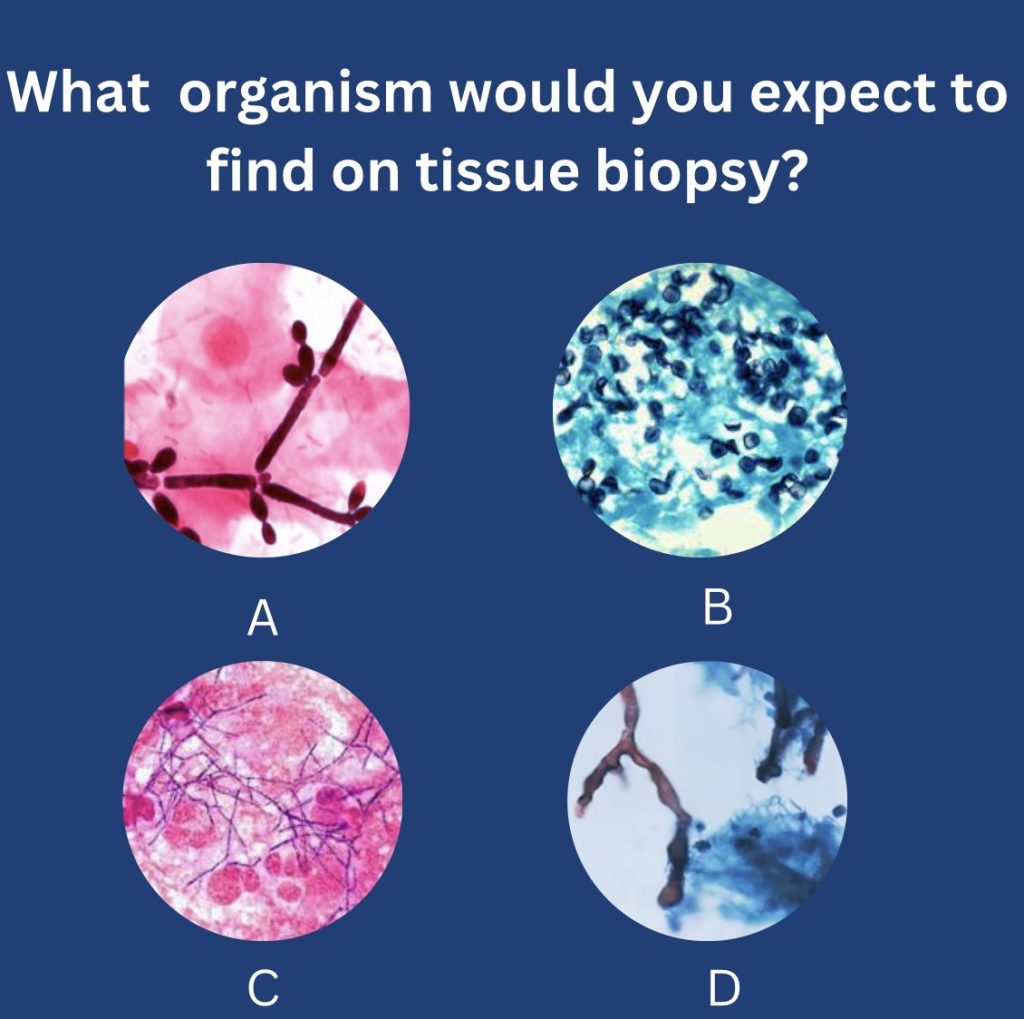
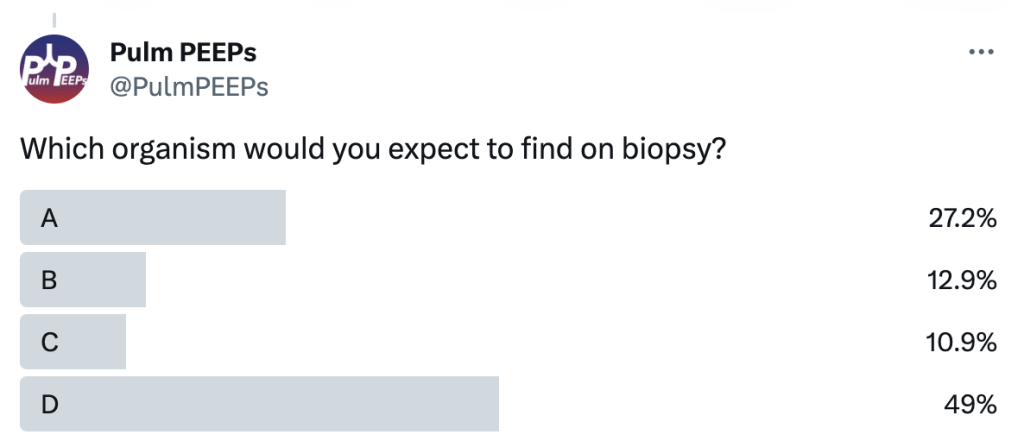
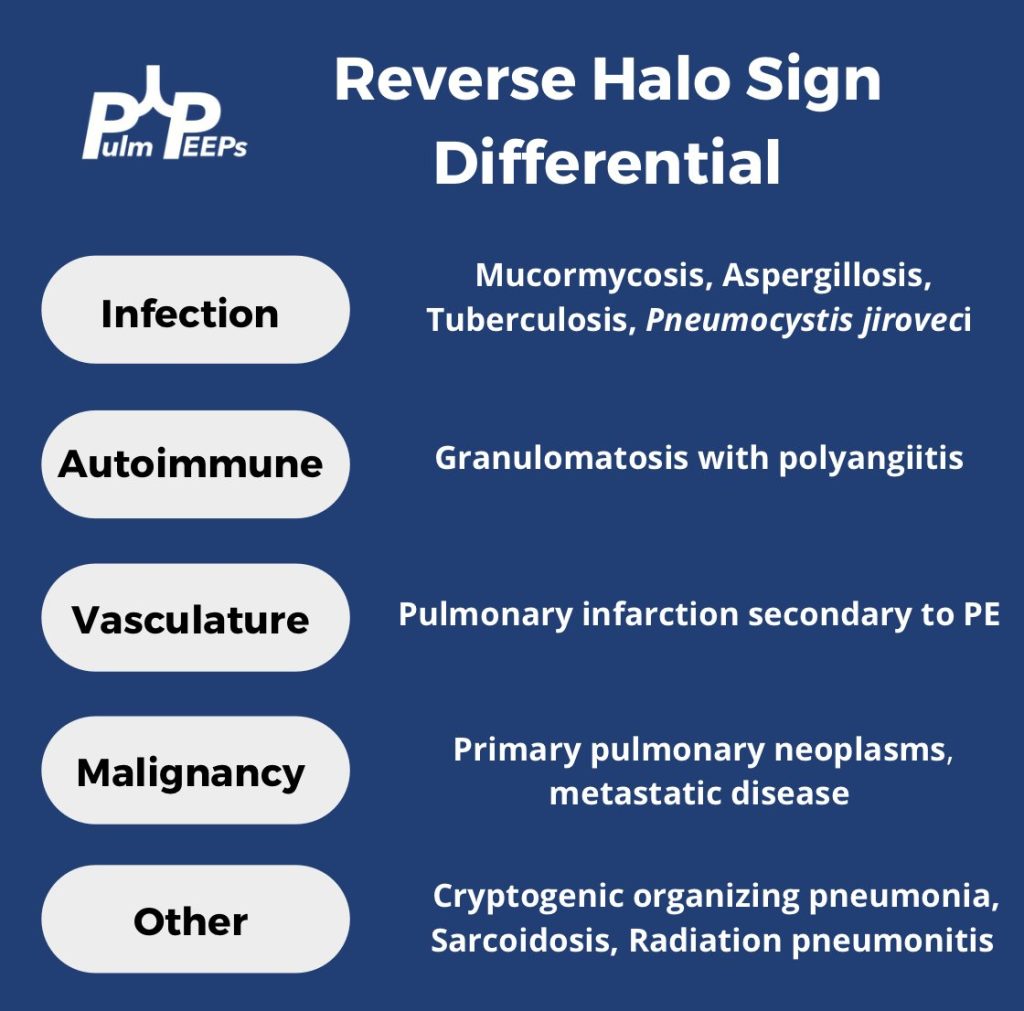
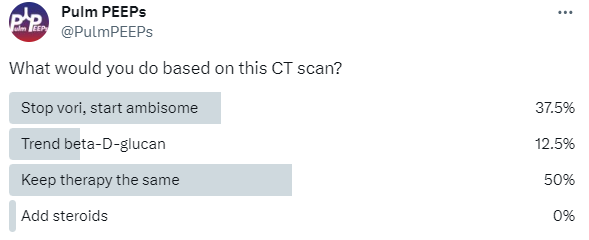
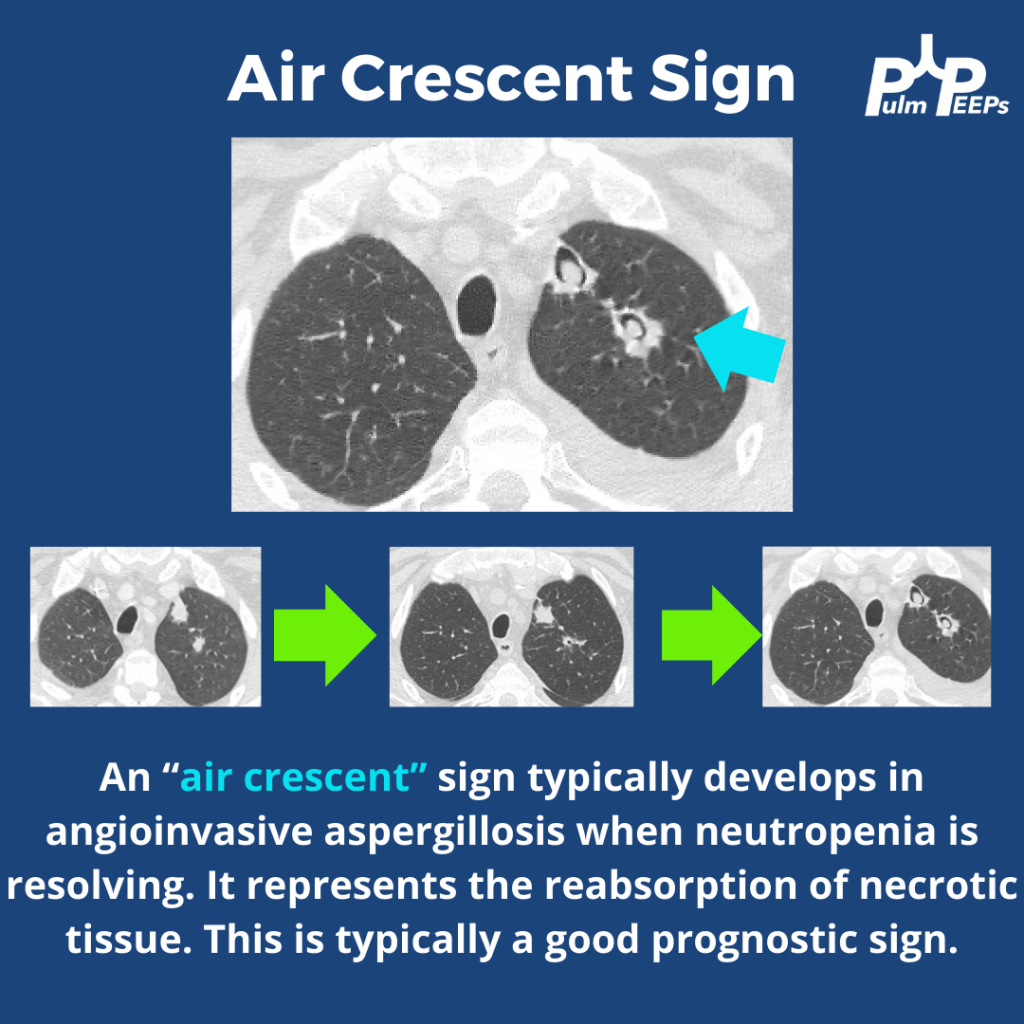
Further, workup reveals a positive serum galactomannan and a BAL PCR that is positive for Aspergillus. The patient is diagnosed with invasive aspergillosis and started on voriconazole. A repeat CT is obtained in 3 weeks. What do you think of the evolving findings?
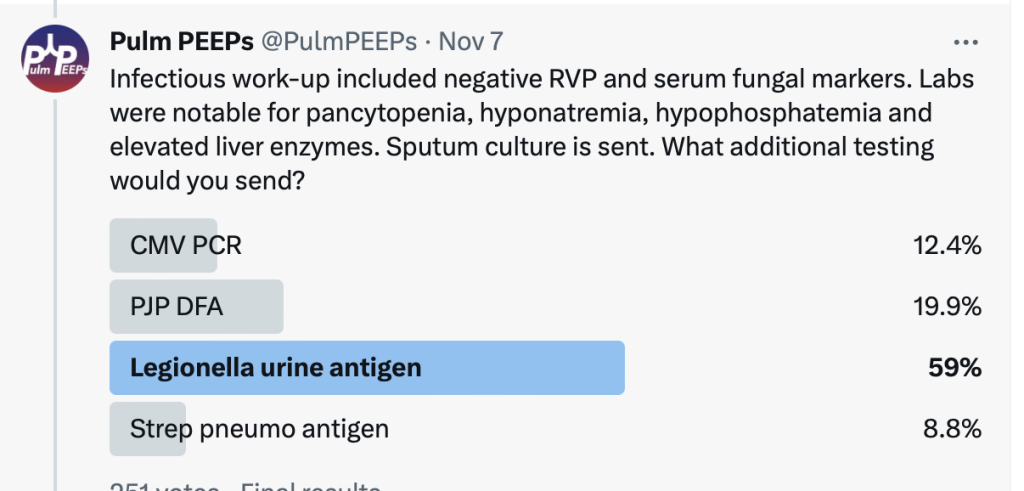
We have a middle-aged immunocompromised male presenting with neutropenic fevers, progressive cough and dyspnea. He has no sick contacts or recent travel.
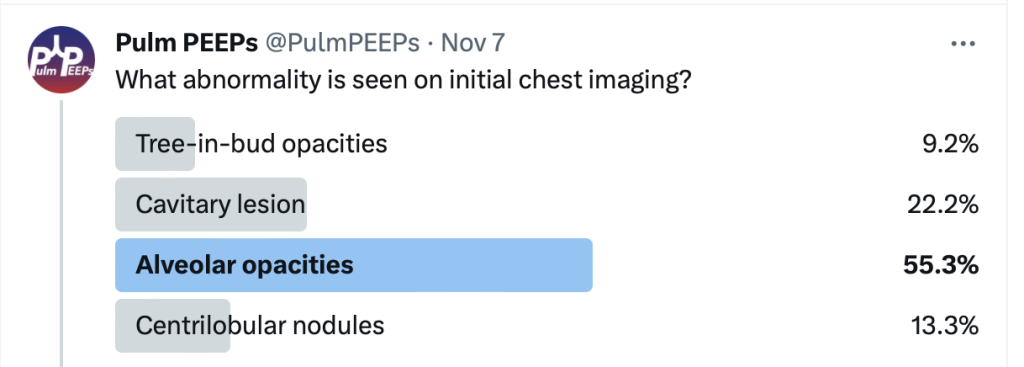
He was found to have primarily right upper alveolar opacities and blunting of the right costophrenic angle. He rapidly decompensated with acute hypoxemic respiratory failure requiring mechanical ventilation. A CT chest showed dense consolidations with air bronchograms.
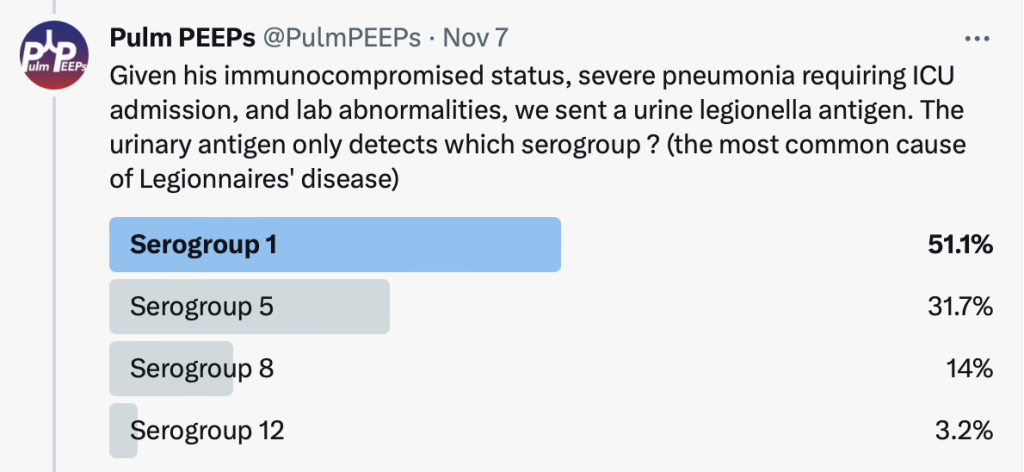
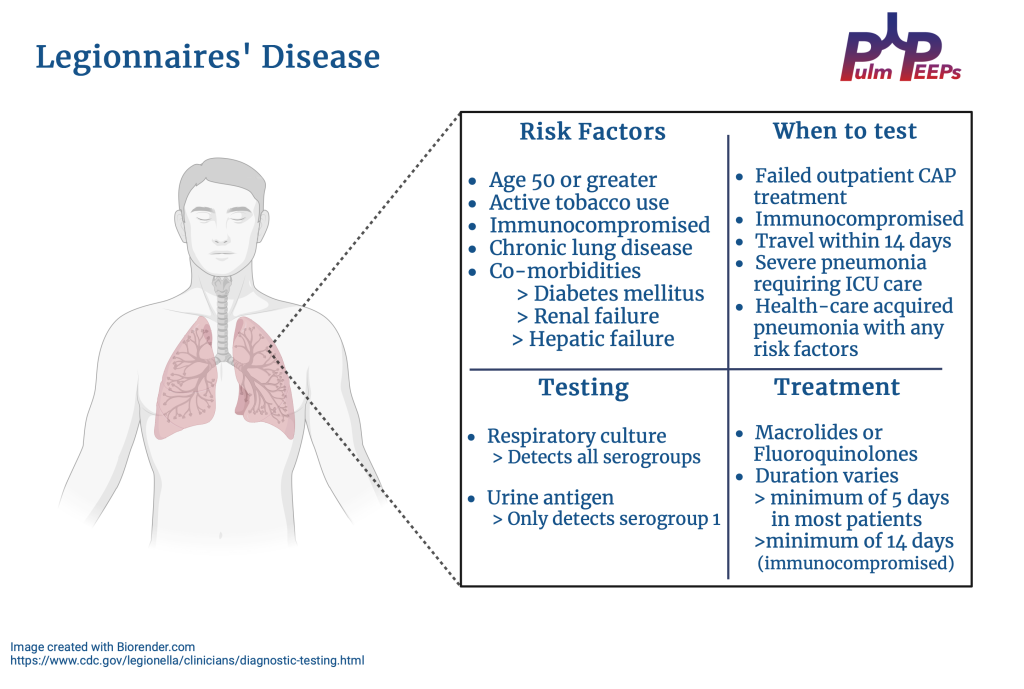
The urinary antigen and sputum culture were positive for Legionella and the patient was continued on Macrolide therapy. See our infographic for high-yield teaching points for Legionnaires’ Disease