We have had a number of episodes on Acute Respiratory Distress Syndrome or ARDS. These episodes have ranged from how to titrate PEEP, subphenotypes in ARDS, and the future of ARDS research. Today, we are talking about how we all think about and define ARDS, and work that has highlighted a newer global definition of ARDS.
Meet our Guests
Dr. Elisabeth Riviello is an Assistant Professor of Medicine at Harvard Medical School, and a PCCM physician at Beth Israeal Deconess Medical Center. She is also an Affiliate of the HMS Department of Global Health and Social Medicine and an honorary Associate Professor of Emergency Medicine and Critical Care at the University of Rwanda. She is passionate about improving critical care delivery in resource limited settings and has served on Committees for the World Health Organization. She is the Principal Investigator of BREATHE or the (Building Respiratory Support in East Africa Through High flow versus standard flow oxygen Evaluation); a RCT looking at HFNC in five sites in Kenya, Malawi, and Rwanda.
Dr. Theogen Twagirumugabe is an Anesthesiologist and Intensivist at the College of Medicine and Health Sciences, and a Professor at the University of Rwanda. In addition to clinical work, he has his PhD in Medical Sciences. He is a widely succesful researcher with over 70 publications in critical care and anesthesia delivery and is also a lead investigator in the BREATHE initiative.
Welcome to our second episode of ATS 2024 highlighting content featured through the ATS Critical Care Assembly. Today we are going to be talking about one of the Critical Care Assembly Symposiums entitled: “Care of Dying in the ICU: End of Life Care in 2024 and Beyond”
Meet our Guests
Dr. Theodore “Jack: Iwashyna is a Bloomberg Distinguished Professor at Johns Hopkins School of Medicine and the Johns Hopkins Bloomberg School of Public Health. Jack is a critical care physician and has a broad focus on research that understands the broader context of critical illness, and the long term impact on patients’ lives. He is an enormously productive and successful researcher with numerous publications in the field of critical care, and is a pioneer in the field of ICU survivorship. He is a devoted mentor and has received accolades from numerous societies
Dr. Molly Hayes is an Associate Professor of Medicine at Beth Israel Deaconess Medical Center and Harvard Medical School, the Director of the MICU at BIDMC, and the Director of External Education at the Carl J Shapiro Institute for Education and Research. She additionally is a co-founder of the BIDMC Center for Humanizing the ICU. Molly has been extensively involved with ATS with leadership roles in the Critical Care Assembly, and the newly minted Steering Committee on the Advancement of Learning.
Meet our Collaborators
The American Thoracic Society Critical Care Assembly is the largest Assembly in the American Thoracic Society. Their members include a diverse group of intensivists and care providers for both adult and pediatric critically ill patients. The primary goal of the Critical Care Assembly is to “improve the care of the critically ill through education, research, and professional development.”
Welcome to our first episode of ATS 2024 highlighting content featured through the ATS Critical Care Assembly. Today we are going to be talking about one of the Critical Care Assembly Symposiums entitled: “A New Reality for Critical Care after Dobbs.”
Meet our Guests
Dr. Katie Hauschildt is a Faculty Research Associate at The Johns Hopkins University School of Medicine where she conducts research on equity in healthcare and critical illness recovery. She has her PhD in Sociology from the University of Michigan and an Advanced Fellowship in Health Services Research from the VA Ann Arbor Healthcare System, and is a board certified patient advocate.
Dr. Kathleen Akgün is an Associate Profess or Medicine at the Yale School of Medicine. She is the Association Section Chief for the VA section of Pulmonary, the Co-Director of the Network of Dedicated Enrollment Sites Program, the director of the MICU at the VA Connecticut health care system, and a member of the DEI Working Group at Yale.
Meet our Collaborators
The American Thoracic Society Critical Care Assembly is the largest Assembly in the American Thoracic Society. Their members include a diverse group of intensivists and care providers for both adult and pediatric critically ill patients. The primary goal of the Critical Care Assembly is to “improve the care of the critically ill through education, research, and professional development.”
MacDonald A, Gershengorn HB, Ashana DC. The Challenge of Emergency Abortion Care Following the Dobbs Ruling. JAMA. 2022;328(17):1691-1692. doi:10.1001/jama.2022.17197
Ashana DC, Chen C, Hauschildt K, et al. The Epidemiology of Maternal Critical Illness Between 2008-2021. Ann Am Thorac Soc. Published online June 14, 2023. doi:10.1513/AnnalsATS.202301-071RL
Sonntag E, Akgun KM, Bag R, et al. Access to Medically Necessary Reproductive Care for Individuals with Pulmonary Hypertension. Am J Respir Crit Care Med. Published online June 13, 2023. doi:10.1164/rccm.202302-0230VP
Griffin KM, Oxford-Horrey C, Bourjeily G. Obstetric Disorders and Critical Illness. Clin Chest Med. 2022;43(3):471-488. doi:10.1016/j.ccm.2022.04.008
Today we’re visiting the University of New Mexico for another interesting entry in our Fellows’ Case Files.
Meet Our Guests
Neel Vahil is a second-year internal medicine resident at the University of New Mexico. He completed medical school at New York Medical College and is planning on applying to pulmonary critical care fellowship programs.
Ishan Patel is a third year PCCM fellow at the University of New Mexico and will be pursuing a second fellowship in clinical informatics this year. He completed medical school and residency in Internal Medicine at Oregon Health & Science University. His fellowship research has focused on clinical outcomes of intensivist-led ECMO programs.
Dr. Lucie Griffin completed her internal medicine residency and PCCM fellowship at the University of New Mexico and is currently the Director of the Albuquerque VA medical intensive care unit.
Case Presentation
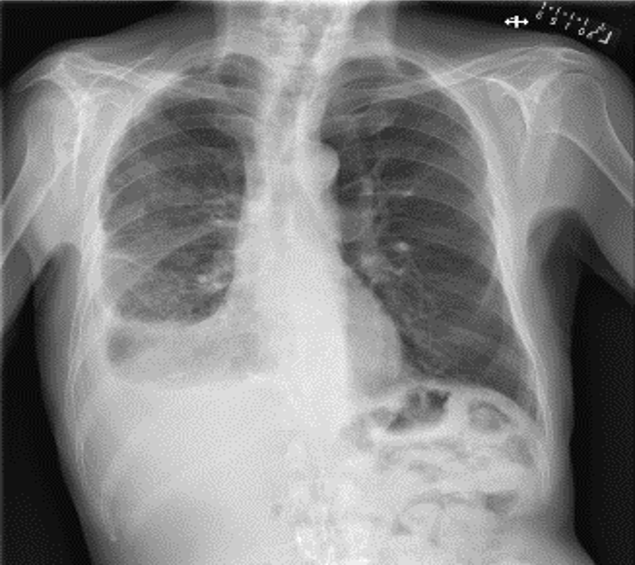
A 69 year old male veteran who presents with 6 weeks of weight loss, cough, and malaise. He has ongoing tobacco use, and history of rheumatoid arthritis on HCQ and weekly MTX with etanercept, which he had stopped taking in the three prior months. Vitals: Afebrile, mildly tachycardic to 101, BP of 93/59, saturating appropriately on room air without any signs of respiratory distress
Key Learning Points
References and Further Reading
Komarla A, Yu GH, Shahane A. Pleural effusion, pneumothorax, and lung entrapment in rheumatoid arthritis. J Clin Rheumatol. 2015;21(4):211-215.
Boddington MM, Spriggs AI, Morton JA, Mowat AG. Cytodiagnosis of rheumatoid pleural effusions. J Clin Pathol. 1971;24(2):95-106.
Balbir-Gurman A, Yigla M, Nahir AM, Braun-Moscovici Y. Rheumatoid pleural effusion. Semin Arthritis Rheum. 2006;35(6):368-378
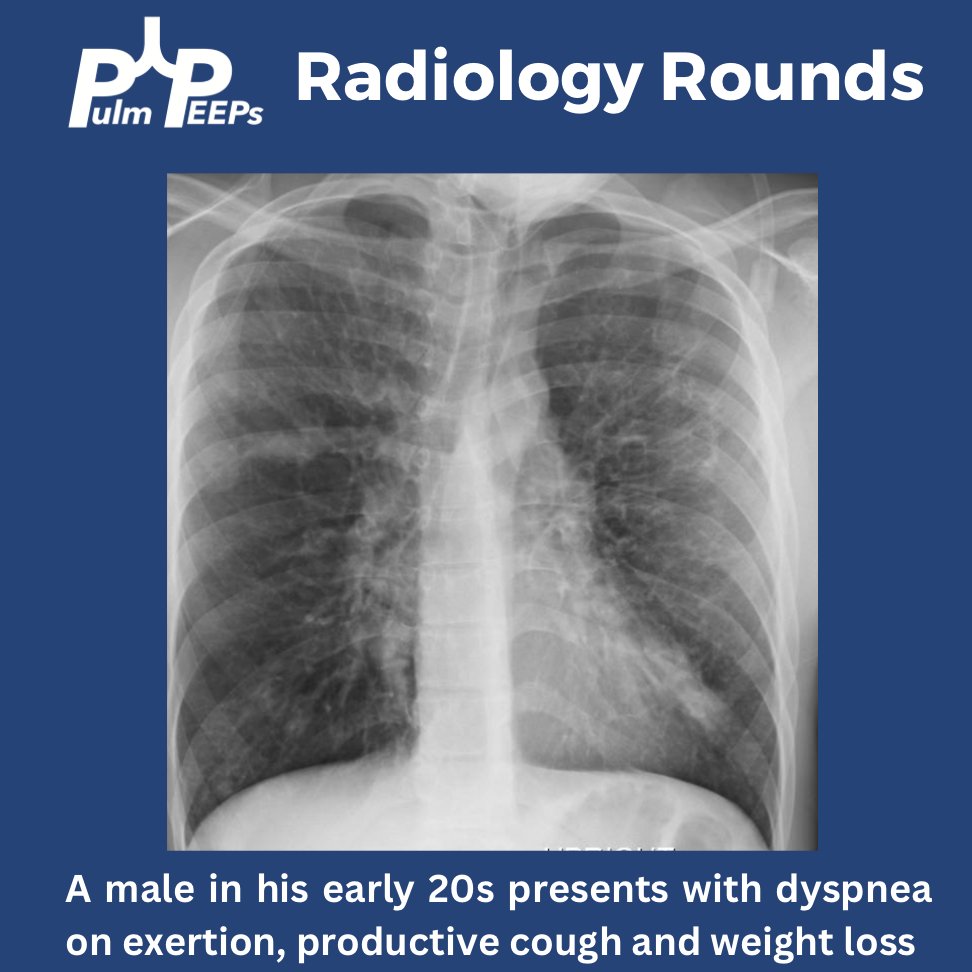
We are excited to start the month off with a new #RadiologyRounds
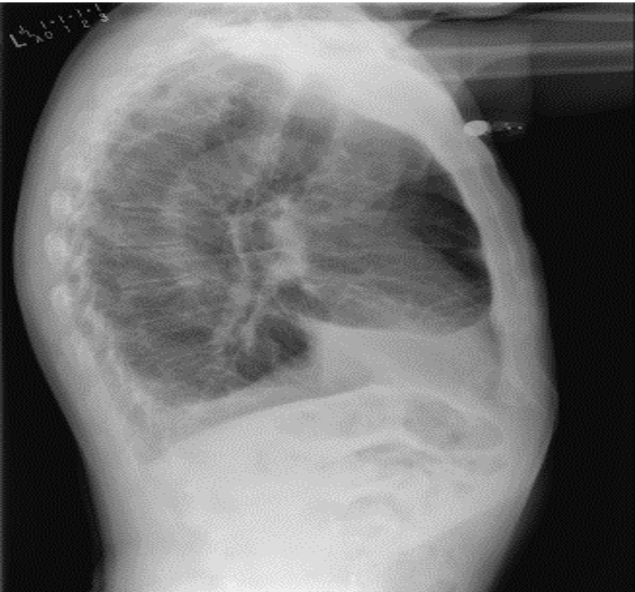
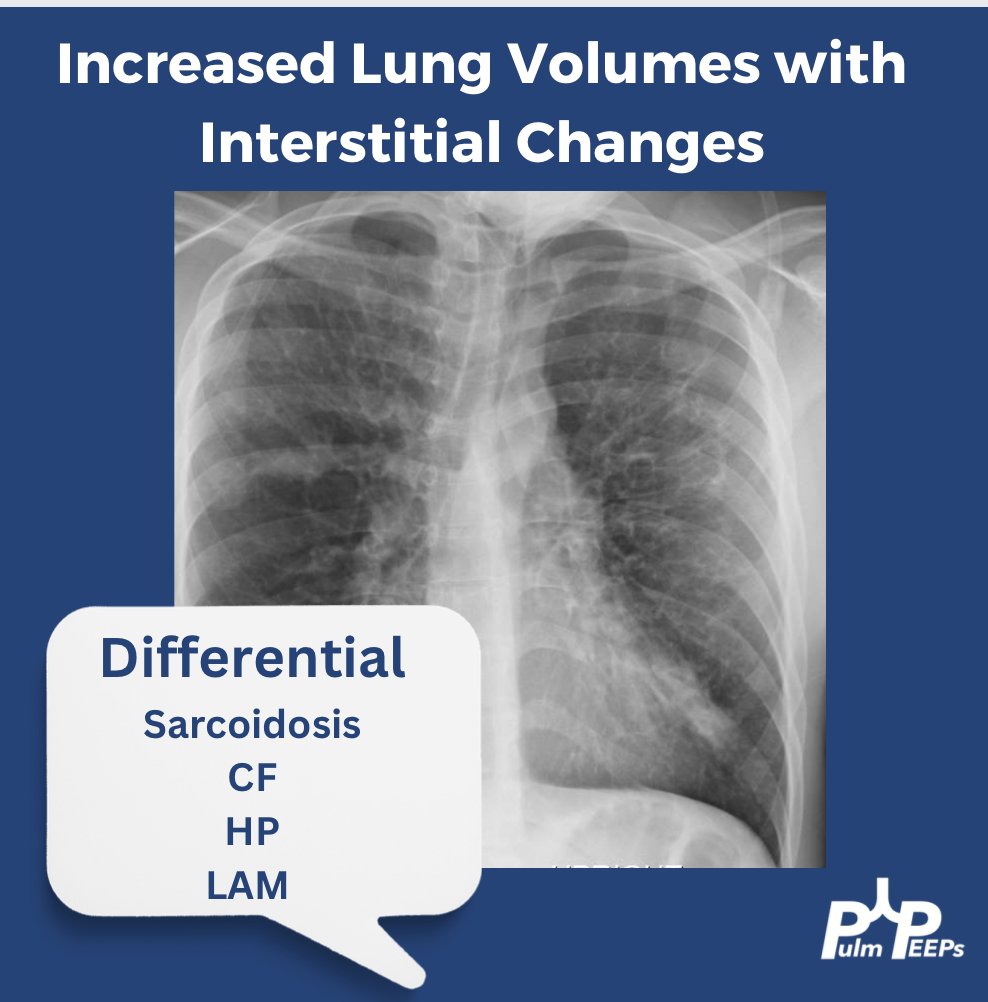
A young adult man in his 20s presents with dyspnea on exertion, productive cough, intermittent wheezing and general fatigue. A chest x-ray was obtained as part of his work-up.
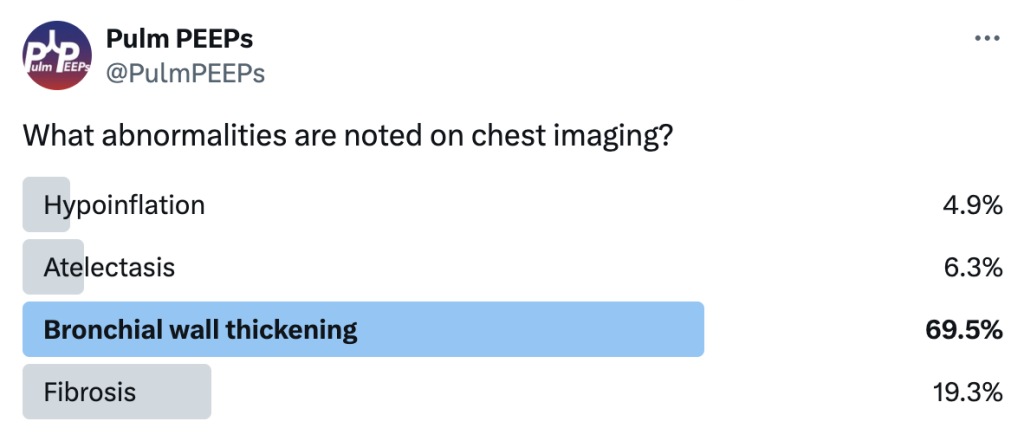
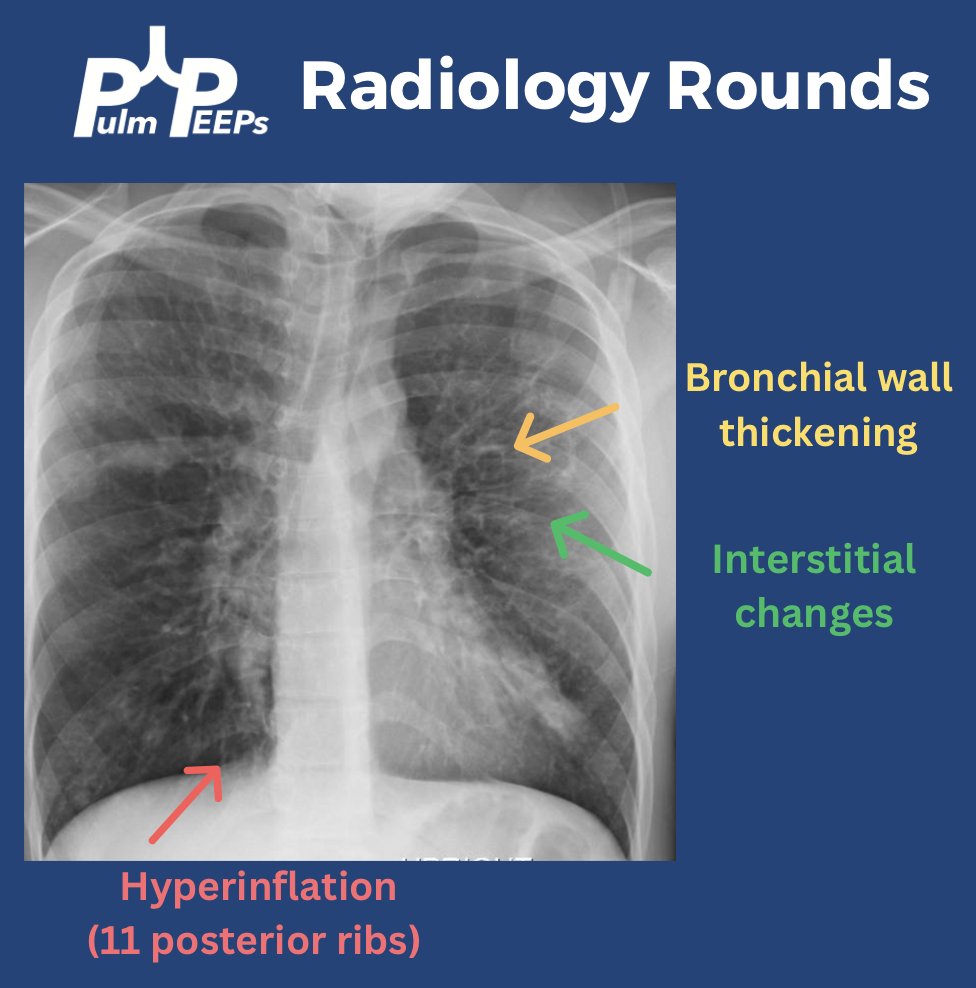
You can identify hyperinflation, interstitial changes and bronchial wall thickening on this image with concern for associated bronchiectasis
You should have Sarcoidosis, Cystic Fibrosis (CF), Hypersensitivity Pneumonitis (HP) and Lymphangioleiomyomatosis (LAM) on the differential
A CT chest is obtained given his abnormal chest x-ray and representative images are shown below
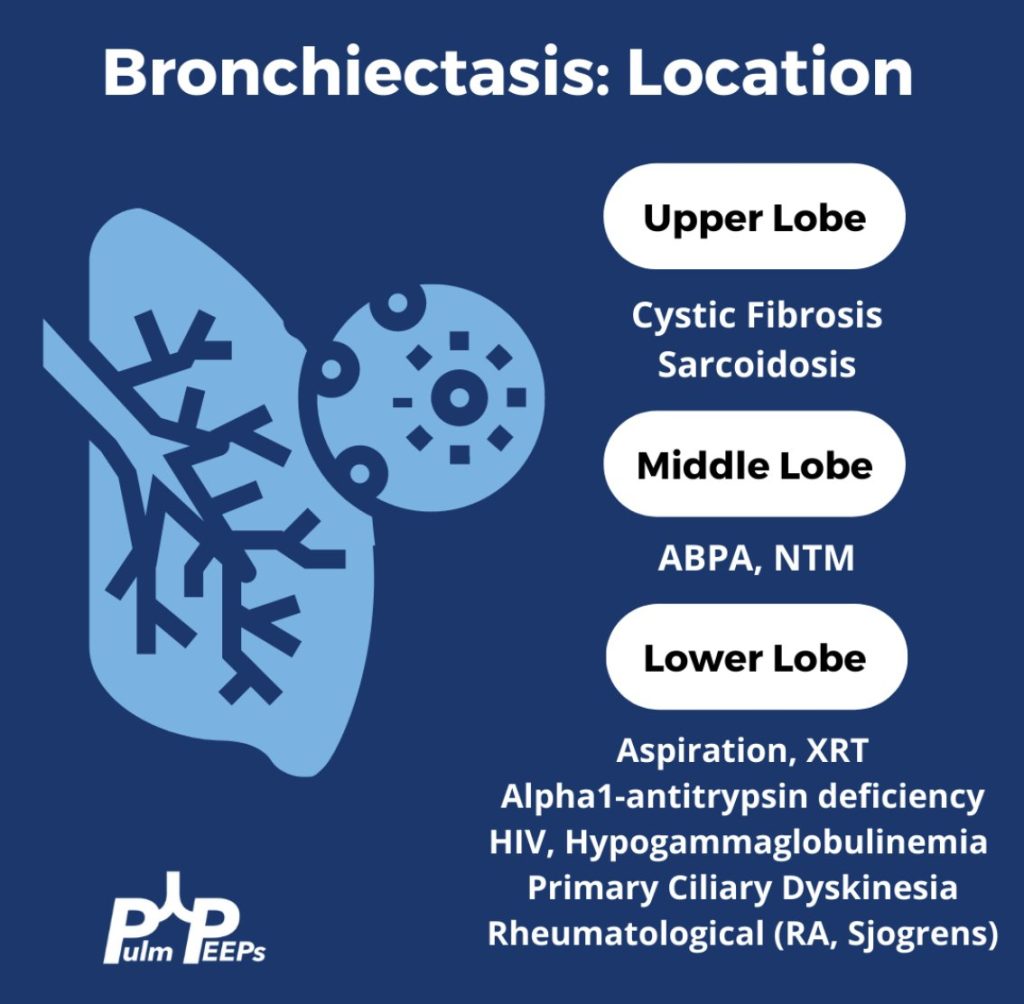
Given upper lobe bronchiectasis you are concerned for cystic fibrosis. A sweat chloride test is obtained and was elevated suggesting CF and further genetic testing was sent to confirm the diagnosis.
We’re super excited to have a joint episode this week with Dr. Cyrus Askin and Dr. Nick Mark from Critical Care Time! We discuss all the ways that bronchoscopy can be your best friend in the ICU and how to be prepared for the unexpected scary situations that arise in the ICU. This ranges from airway bleeds, difficult intubations, lobar collapse, and trach emergencies. Don’t miss this great discussion!
Key Learning Points
Utility of bronchoscopy in people with critical illness
Bronchoscopy can be both diagnostic and therapeutic; both are potentially lifesaving.
General situations where bronchoscopy is useful in the ICU:
Placing (or confirming placement of) an endotracheal tube or tracheostomy tube
Removing a foreign body or mucous plugs from the lungs
Localizing the source of pulmonary hemorrhage or performing interventions to stop/contain the bleed
Diagnosing certain rare conditions, particularly those where the diagnosis can substantially change management (e.g. DAH, AEP, rare infections, etc).
Proficiency with bronchoscopy is important to realize the benefits. Simply “having the equipment” is insufficient, regular practice/simulation is essential
Anesthesiologists, emergency physicians, and other specialists may have limited experience with bronchoscopy in training. Even experienced pulmonologists, who may be good at diagnostic bronchoscopy often have limited experience deploying bronchial blockers, using retrieval baskets, etc.
Remember: “People don’t rise to the occasion, they sink to the level of their training.”
If you haven’t regularly practiced with a bronchoscope, you are not going to be able to use it effectively under stress when performing high acuity low occurrence (HALO) procedures such as in emergent airways, deploying bronchial blockers, retrieving foreign bodies, etc.
Two broad situations where a bronchoscope is generally used:
Awake intubation in the anticipated difficult airway (e.g. someone with abnormal anatomy, airway tumor, etc)
Rescue method in the unanticipated difficult airway (e.g. very anterior cords, difficulty with Bougie, etc)
Nasal vs Oral approach:
Oral approach is usually used in an unanticipated difficult airway
Nasal approach: More common if performing an awake intubation. Nasal is often better tolerated however epistaxis can make a difficult airway almost impossible.
Sedation strategy:
Full topicalization: lidocaine vs cocaine (equally effective and lidocaine is normally preferred, however the vasoconstriction action of cocaine may be helpful in preventing epistaxis).
Gurgling (Nick: from personal experience lidocaine is super gross)
Remember total dose of lidocaine: < 8 mg/kg
Ketamine
Ideal because it’s dissociative and analgesic, maintains respiratory drive and (maybe) airway reflexes
Consider scopolamine patch to reduce oral secretions
Dexmedetomidine
Great adjunct
One vs two operator
Especially in unanticipated difficult airways; the second operator can use VL/DL to facilitate visualization of the vocal cords.
Second operator can also be preparing for a surgical airway.
Equipment considerations:
Preload the endotracheal tube onto the bronchoscope. Use the bronchoscope as a bougie to guide the ETT through the vocal cords.
Suction! You want two – one connected to the bronch and one connected to a yankuer.
Disposable vs “good” scope
Remember to load the tube first!
Also remember to lube the tube!
Tracheostomy troubleshooting
Similarly to intubation, bronchoscopy can be very useful to confirm placement
Mechanics are similar to above
Goal is to avoid inadvertent placement of the tracheostomy tube into the soft tissues of the neck and to avoid putting air into those tissues (false lumen).
Advanced trick for exchanging tubes: You can use a disposable bronchoscope to exchange tubes: you can get it in, confirm placement, then cut it with trauma shears! Now you can slide the old tube out and put a new one in. (Don’t try this on a $40,000 fiberoptic bronchoscope!)
Ideally you should load the ETT onto the bronchoscope in advance (red arrow). If necessary however, you can cut the ETT and turn the disposable bronchoscope into a improvised exchange catheter. This technique is very useful for exchanging tracheostomy tubes.
Foreign Body Removal from airways
Bronchoscopy is invaluable for both diagnosis and treatment of foreign body aspirations.
Most commonly these aspirations are food (nuts, seeds, etc), teeth, pills, etc
Intubated is harder in many cases: no cough to help, hard to get foreign body out of the ETT.
Flexible vs rigid
Most objects can be retrieved using flexible bronchoscope; however 15-20% require rigid bronchoscopy
Flexible can reach smaller foreign bodies that are lodged more distally.
Rigid bronchoscopy is usually done if flexible bronchoscopy fails; an interventional pulmonologist wielding a rigid is superior but more invasive (requires GA)
Cryoprobe can be especially useful for frangible materials (e.g. food)
Mucous Plugs & Lobar collapse
Presentation can be subtle or dramatic.
Bronchoscopy can remove mucous plugs and help re-expand collapsed lung areas, which is potentially life saving.
Additionally, bronchoscopy can permit diagnosis of tracheal bronchus (bronchus sui)
Pig bronchus – 1-3% of people – have a RUL bronchus that comes off the trachea.
Often presents with RUL collapse in an intubated person.
Suction considerations and bronchoscope size
Remember that suctioning force is highly dependent (i.e. radius raised to the fourth power!) upon the working channel size. Use the largest size bronchoscopy possible when suctioning.
Remember that other interventions: regular inline suctioning, chest PT, adequate hydration, mucolytics are also important to prevent recurrent mucous plugging.
Localization & Isolation of Pulmonary Hemorrhage
Pre-bronch interventions
Stabilization
Nebulized TXA
Bad side down → counter-intuitive because shifting blood flow, but also the goal is to protect the non-bleeding lung.
etc
Bronch can localize the bleeding site. Bronch can also perform interventions such as:
Cold saline
Epinephrine 1:100,000
Bronchial blockers – comparison of types
CRE balloon
Fogarty
Cryo probe – great for removing clots
Delivering ETT to contralateral side → single lung ventilation
Making “bronchoscopy only” diagnoses
Diffuse Alveolar Hemorrhage (DAH)
Finding: Increasingly bloody returns on serial lavages
1) an unexpected diagnosis was made and followed by a management change (as the most rigorous estimate of utility)
13% of the time a diagnosis was only made because of bronchoscopy which changed management
2) the post-bronchoscopy diagnosis was discordant from the leading diagnosis considered before this procedure and was followed by a management change
48% of the time pre and post procedure leading diagnoses were different
26% of the time the change in leading diagnosis led to a change in therapy
3) a change in management was made following bronchoscopy regardless of whether the diagnosis was expected or considered.
32% escalation of antibiotics
30% de-escalation of antibiotics
9% addition of steroids
2% mold → surgery
Remember that in critically ill patients whose symptoms are unexplained or failing to resolve with therapy, diagnostic flexible bronchscopy can provide useful insights.
We’re back with another Case Files episode from Mt. Sinai Morningside. Listen in to hear another great case and some key learning points along the way.
Meet Our Guests
Dr. Sara Luby is a third-year Internal Medicine resident and rising chief resident at Mt. Sinai Morningside/West and planning on applying to Pulmonary and Critical Care fellowship this upcoming year.
Dr. Javier Zulueta is the Chief of the Division of Pulmonary, Critical Care, and Sleep Medicine at Mount Sinai Morningside. He completed residency training at St. Luke’s Medical Center/Case Western in Cleveland and fellowship in Pulmonary/Critical Care at Tufts Medical Center in Boston. His research focuses on lung cancer screening and incidental lung findings.
Dr. Mirna Mohanraj is the Associate Program Director for the Pulmonary and Critical Care Fellowship at Mt. Sinai Morningside / Beth Israel and an associate professor of medicine and medical education at the Icahn School of Medicine at Mount Sinai. She completed residency training at University of Chicago and fellowship training at Mt. Sinai Hospital.
Case Presentation
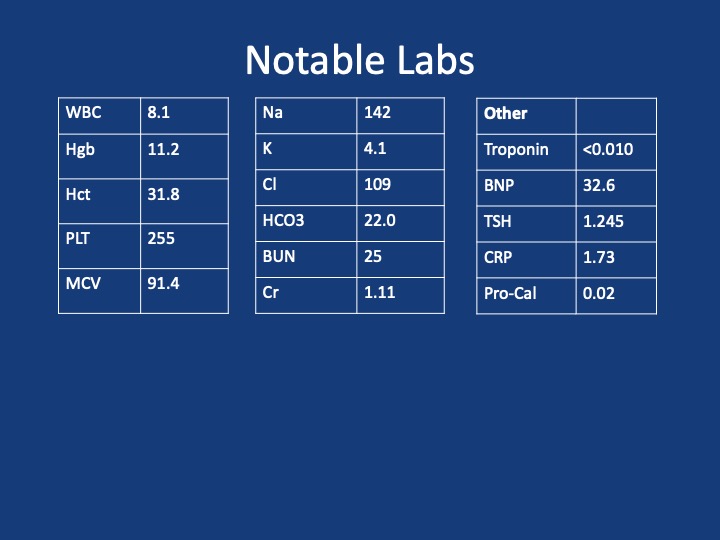
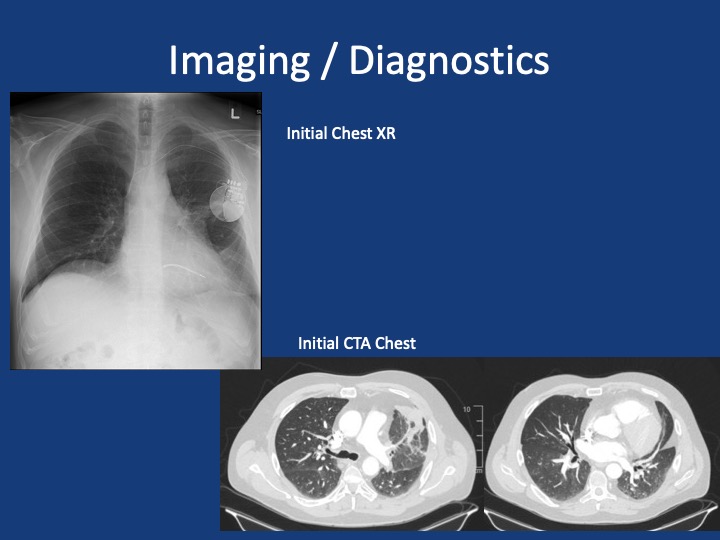
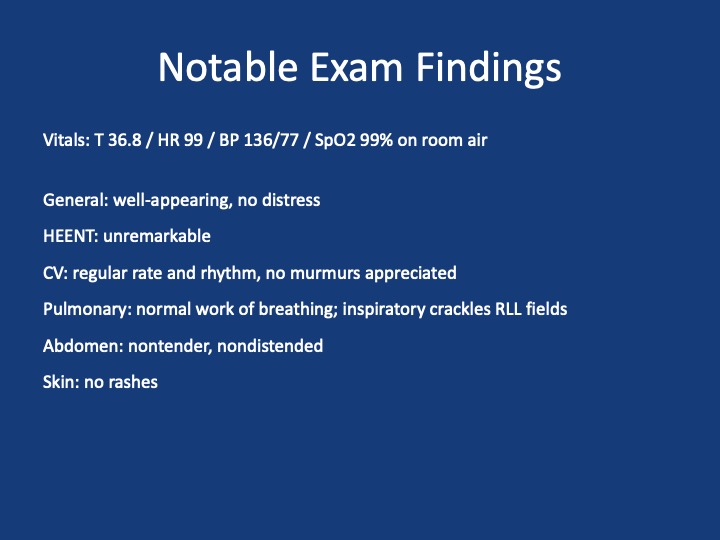
A 51 year old male presents with two days of acute on chronic chest pain and shortness of breath, worsening over the last month. His initial vitals: 143/ 100, pulse 85, temperature 36.5 °C (97.87°F), RR 16, SpO2 97 % on room air, BMI 29.8
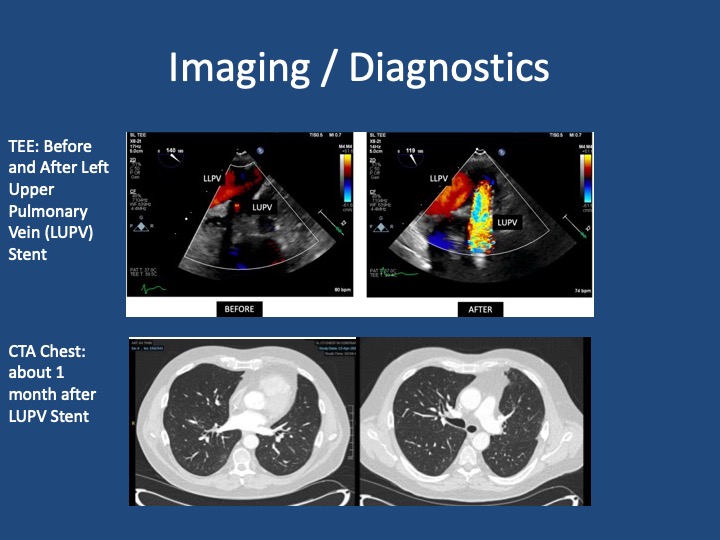
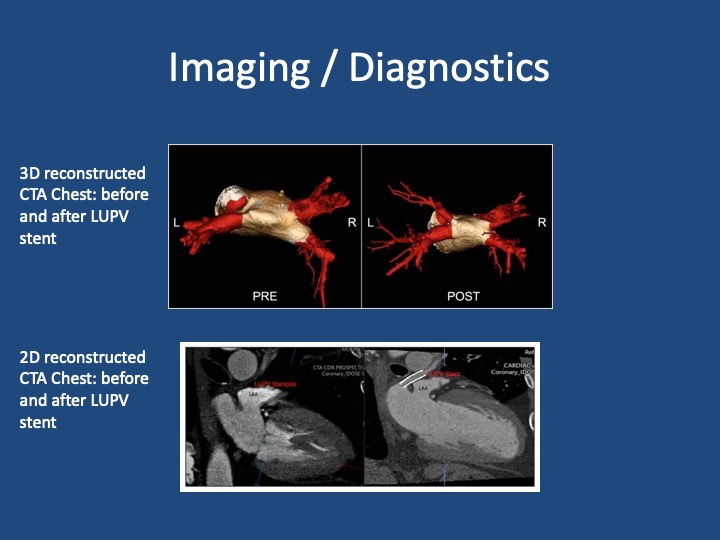
Pre and Post Treatment Imaging
References and Further Reading
Shroff N, Choi W, Villanueva-Meyer J, Palacio DM, Bhargava P. Pulmonary vein occlusion: A delayed complication following radiofrequency ablation for atrial fibrillation. Radiol Case Rep. 2021;16(12):3666-3671. doi:10.1016/j.radcr.2021.09.015
Fender EA, Widmer RJ, Hodge DO, et al. Assessment and Management of Pulmonary Vein Occlusion After Atrial Fibrillation Ablation. JACC: Cardiovascular Interventions. Vol 11(16); 2018. doi:10.1016/j.jcin.2018.05.020
López-Reyes R, García-Ortega A, Torrents A, et al. Pulmonary venous thrombosis secondary to radiofrequency ablation of the pulmonary veins. Respir Med Case Rep. 2018;23:46-48. doi:10.1016/j.rmcr.2017.11.008
Mizuno A, Mauler-Wittwer S, Muller H, Noble S. Recurrent pneumonia post atrial fibrillation ablation: do not forget to look for pulmonary vein stenosis. BMJ Case Rep. 2022;15(12):e250896. doi:10.1136/bcr-2022-250896
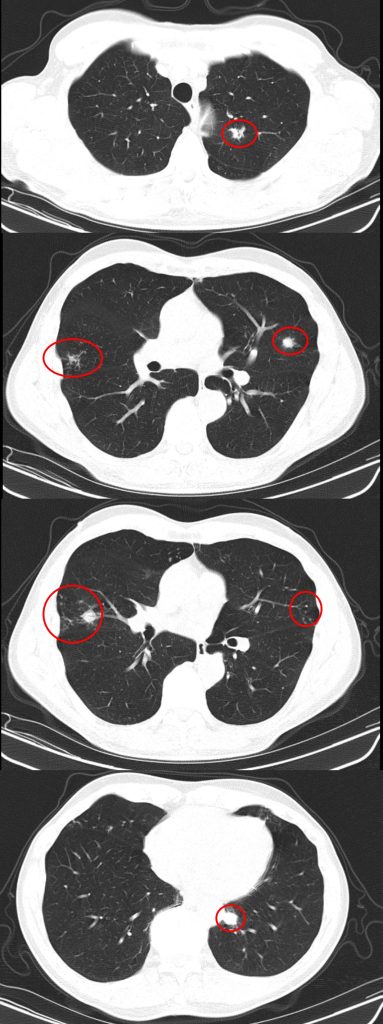
A #RadiologyRounds case with 3 different imaging modalities! A 65+ year old man never smoker, former marathoner has had 2-3 years of progressive non-productive, incessant cough with decreasing exercise tolerance. Some select CT scan slices are below
You are considering multiple etiologies including airway bleeding, pneumothorax, and hemothorax. You grab an ultrasound and perform a lung / pleural POCUS. Here is what you see
The long POCUS shows an area of lung sliding and an area without any lung sliding. This is called lung point and is diagnostic of a pneumothorax. To get a better look at this, you can use M-mode.
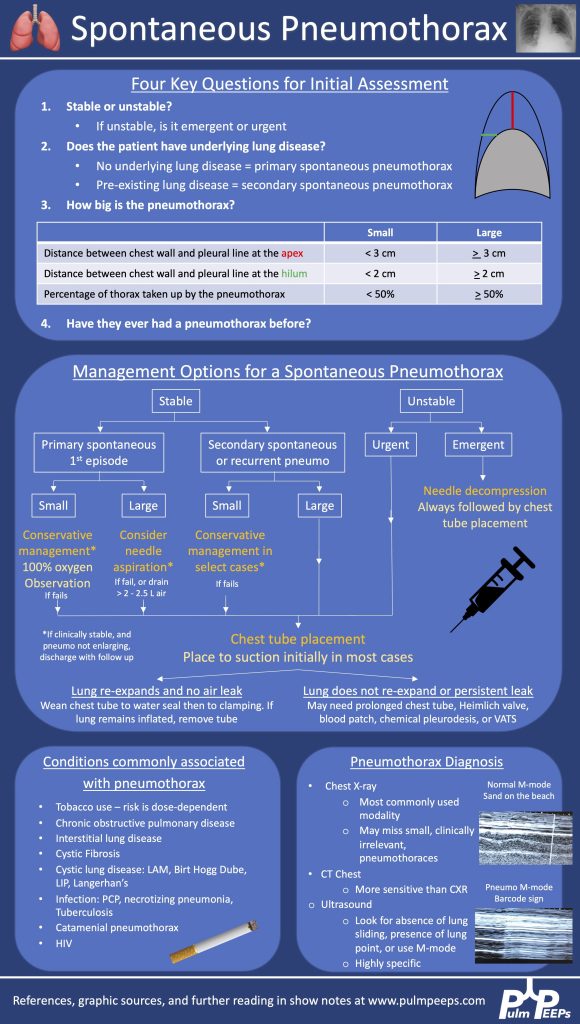
A CXR confirmed the finding of a pneumo. He was trialed on 100% oxygen but repeat CXR showed the pneumothorax was expanding. He had a chest tube placed with re-expansion of his lung and no air leak. It was able to be removed the next morning without incident
Here is our algorithm for pneumothorax!
Both BAL and tbbx returned positive for MAI complex. He was HIV neagative. Given his persistent and bothersome symptoms, he was started on treatment for pulmonary MAC with a macrolide, ethambutol and a rifamycin with plan for 6 months of therapy. He improved with this
Listen in today to another stop on our Fellows’ Case Files journey. We’re at Northwestern University for another great case presentation. Tune in, check out our associated infographic, and let us know what you think!
Meet Our Guests
Jamie Rowell is a first-year clinical fellow in the Northwestern PCCM program. She completed medical school at the Medical University of South Carolina and her internal medicine residency and Chief Residency at the University of Vermont Medical Center.
Cathy Gao is an Instructor of Medicine at Northwestern and completed her PCCM fellowship there last year. Her research focuses on using machine learning applied to ICU EHR data to characterize patient trajectories and identify potential interventions to improve outcomes.
Clara Schroedl is an Associate Professor of Medicine in Pulmonary and Critical Care and Medical Education. She is the program director of the Northwestern PCCM fellowship program, with an interest in medical education and simulation.
Case Presentation
A 25-year-old previously healthy woman presents with recurrent episodes of right chest pain and cough. In October she was treated with antibiotics and felt somewhat better but in December, she presented again with chest pain, and again was treated with antibiotics. The pain improved but she still felt breathless. In February, again she had intense chest pain interfering with life, and was given NSAIDs and took high dose TID without clear benefit.
One month later, she coughed up some bloody mucus, so now she is presenting for evaluation. The chest pain is worse with deep breaths and improves in between these episodes. She only notes it on her right side. At this point, she does sometimes feel short of breath; she used to run 5 miles but is now struggling to run two miles. She denies any unusual exposures. She went to school in central rural Ohio for a while. She has no history of pulmonary infections, no exposure to mold or animals, and no history of vaping.
Key Learning Points
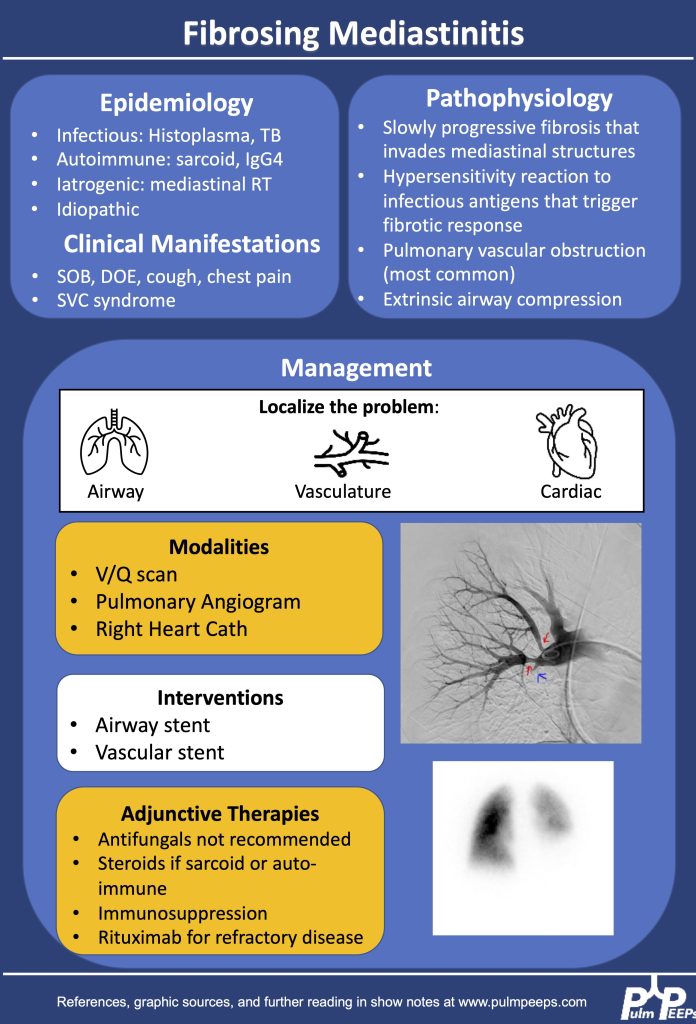
1.Making the diagnosis of Fibrosing Mediastinitis :
–Etiologies: histoplasmosis, sarcoidosis, tuberculosis, IgG4, Behcet, ANCA vasculitis
–Imaging characteristics: infiltrative, heterogeneous, fibrotic process that crosses fat planes and encroaches on nearby structures causing airway or vascular stenoses
2. Management strategies:
–No curative therapies. Goal to relieve symptom burden
–Airway stents
–Vascular stents
–Rituximab
–Antifungals, steroids generally not considered effective
References and Further Reading
Kern et al. Bronchoscopic Management of Airway Compression due to Fibrosing Mediastinitis. Annals of the American Thoracic Society 2017. 14: 1235-1359
Welby JP, Fender EA, Peikert T, Holmes DR Jr, Bjarnason H, Knavel-Koepsel EM. Evaluation of Outcomes Following Pulmonary Artery Stenting in Fibrosing Mediastinitis. Cardiovasc Intervent Radiol. 2021 Mar;44(3):384-391. doi: 10.1007/s00270-020-02714-z. Epub 2020 Nov 17. PMID: 33205295.
Westerly, BD Targeting B Lymphocytes in Progressive Fibrosing Mediastinitis.Am J Respir Crit Care Med. 2014 Nov 1; 190(9): 1069–1071.