
For “#RadiologyRounds” today, we won’t be looking at any imaging, but we’ll be looking at some vent wave forms and examining dysynchrony! This is a re-booted @david_furfaro Tweetorial. I hope you enjoy and this is an open invitation for all dysynchrony waveforms!
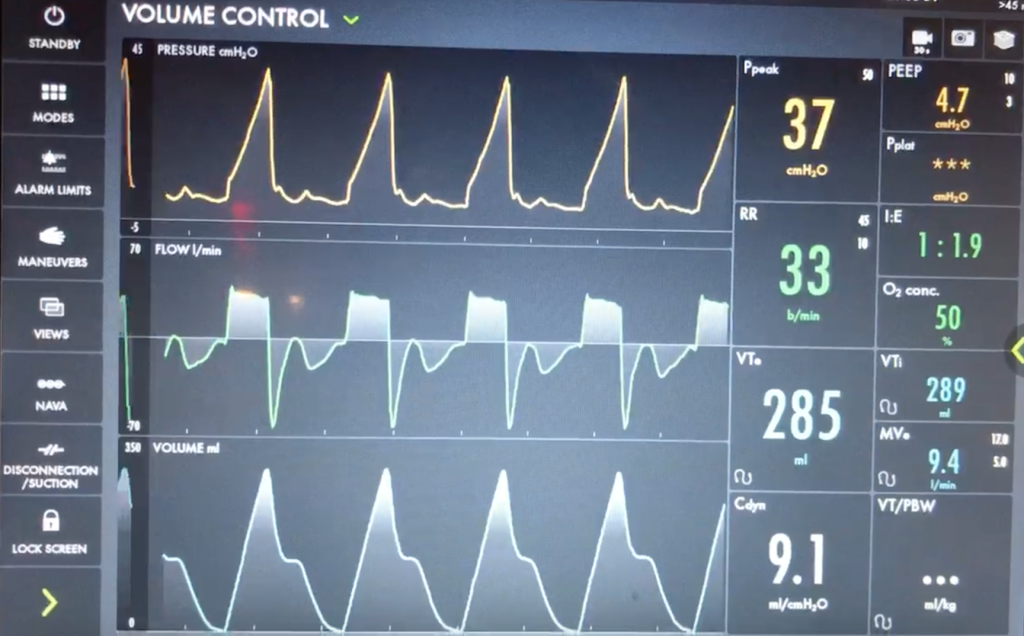
A 40s M is intubated for ARDS. In order to maintain lung protective ventilation, he was on high does of propofol, fentanyl and midazolam. His sedation is being weaned slightly now, and the RN calls for vent dysynchrony. His ventilator looks like this
Before delving into the type of dysynynchrony and management, based on these waveforms what is actually happening? Note: when we say “exhales” or “inhales” I am referring to the mechanical, vent-driven breaths
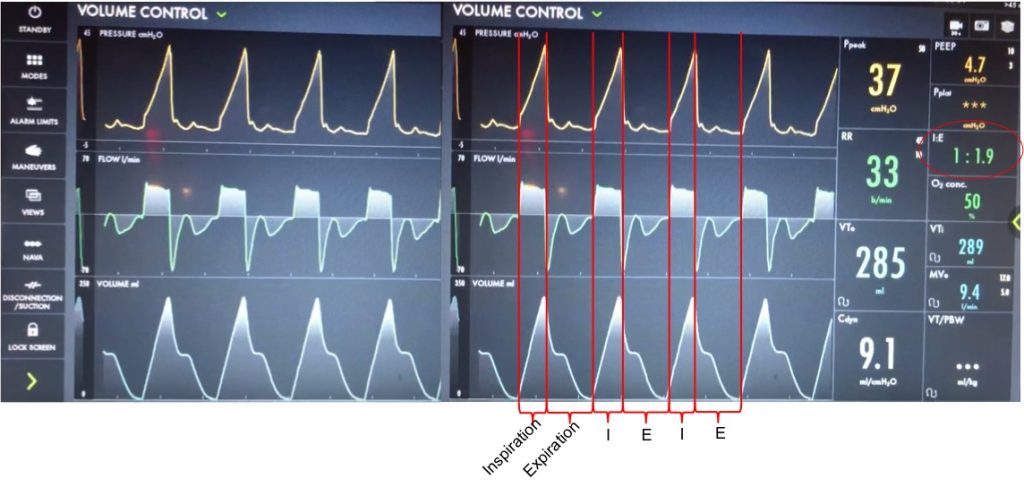
Let’s take a look at the waveforms and identify the phase of breathing. This is VC with a square flow waveform, so as a set volume is delivered, the flow is at a constant rate, and the pressure is measured. Expiration is about 2x as long as inspiration (determined by I time or flow rate)
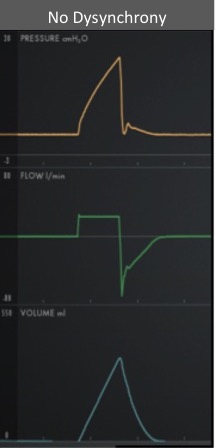
With a passive patient (no dysynchrony) after inspiration, the volume curve should show a smooth decrease with exhalation, the pressure curve should flatten to the set PEEP, and the flow will be negative and gradually return to 0 as the patient exhales
In our case, you can see simultaneous dysynchrony in all three waveforms during exhalation (red arrows) vs normal (orange lines). There is a pressure negative deflection; the flow quickly rises to 0 before returning to negative; and the volume curve plateaus as exhalation pauses

Putting this together, it means that during expiration there is an inspiratory effort. The patient is trying to inhale, which causes a negative pressure deflection, and a pause in air flowing out of the lungs. If this effort triggered a breath, there could be breath stacking. Notice that the same pattern occurs after every breath, and clinically we said the patient was still heavily sedated. This combination of findings is a type of dysynchrony called REVERSE TRIGGERING or ENTRAINMENT.

You could consider whether this dysynchrony was an ineffective effort, but the trigger sensitivity was low, and the pattern and consistent timing after inspiration is more consistent with reverse triggering.
The change in pressure and flow of a ventilator-initiated, mandatory breath stimulates an inspiratory effort from the patient. Theories differ on if this is mediated by the diaphragm or central respiratory center. This can start during the ventilator-delivered breath, or afterwards in exhalation, as with our patient.
Reverse triggering often occurs in heavily sedated patients, and is defined by a stable, repetitive pattern (i.e. it is not voluntary, but reflex mediated). It can also occur in anoxic brain injury. Treating it involves breaking the pattern and avoiding harmful therapies. It can even be induced in healthy patients but this is much less clinically relevant, and is rare.
DO NOT just increase the trigger sensitivity of the vent. This can stop breath stacking but does not prevent dysynchrony and it can cause harmful changes in transpulmonary pressure. For this patient, sedation was lightened slightly, and the respiratory rate decreased and the pattern of reverse triggering ultimately broke without the need for paralysis.