It is Tuesday #RadiologyRounds time! We are in a pleural state of mind here at Pulm PEEPs. This is another great case authored by rockstar-associate editor @TessLitchman
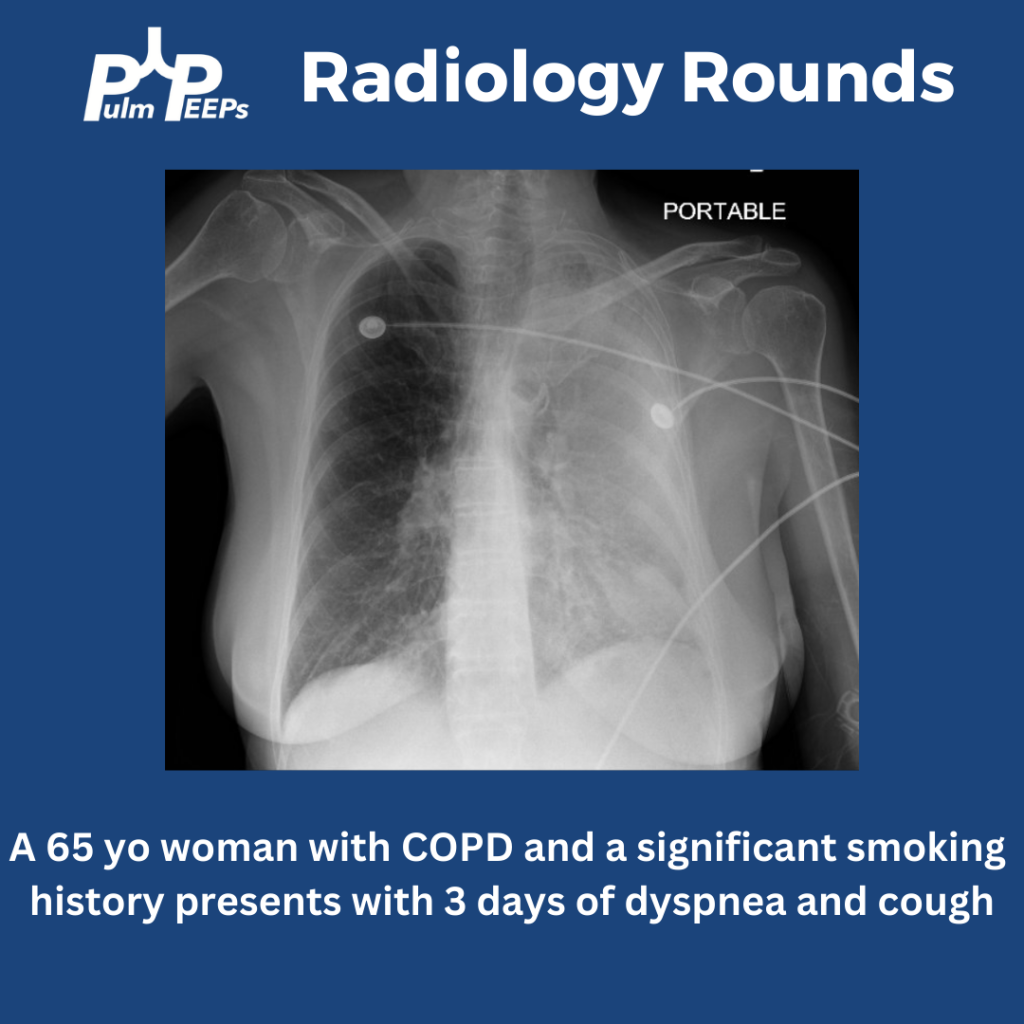
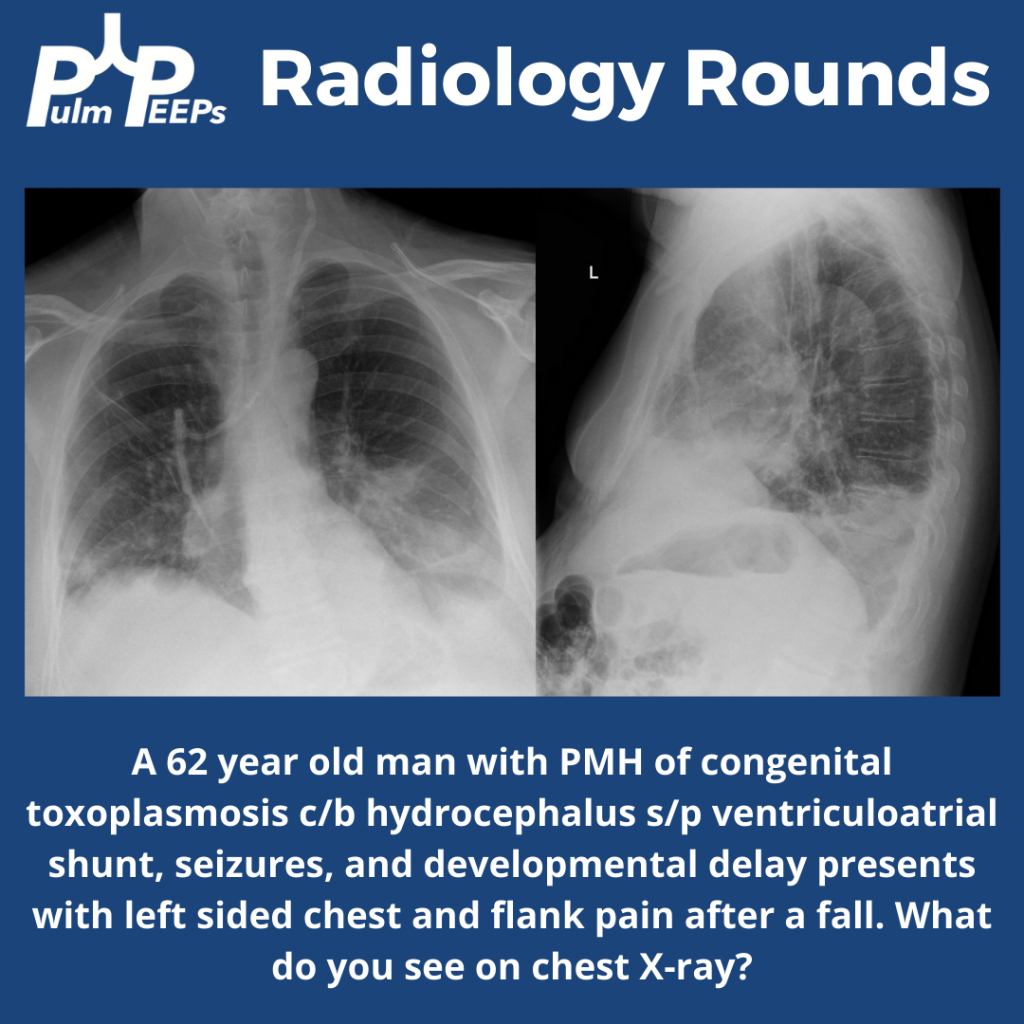
A 65-year-old man with cirrhosis presents to the ED with progressive shortness of breath:
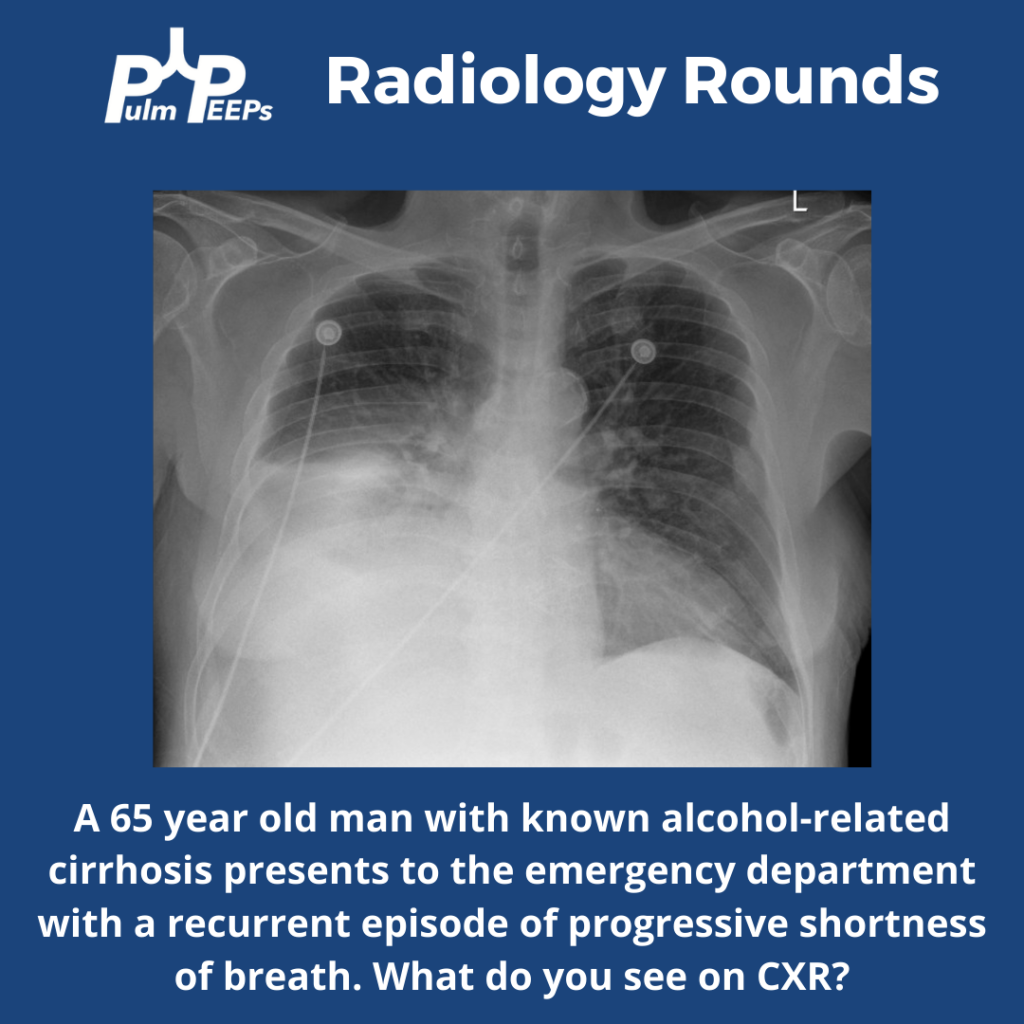
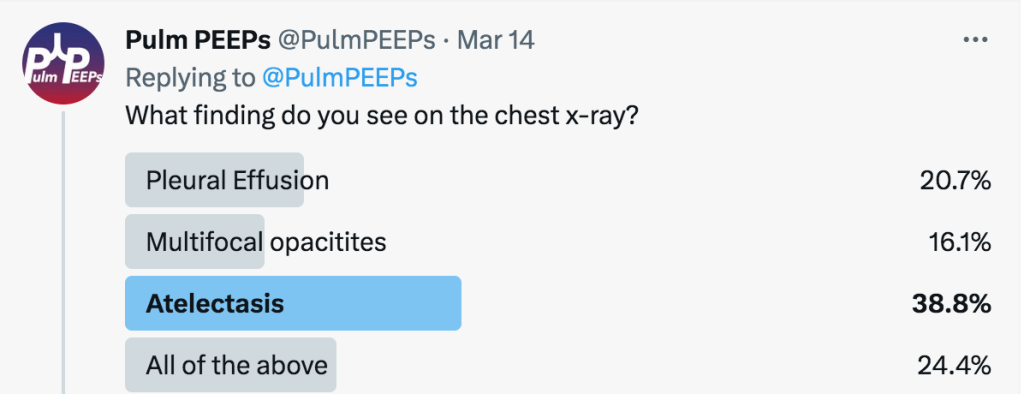
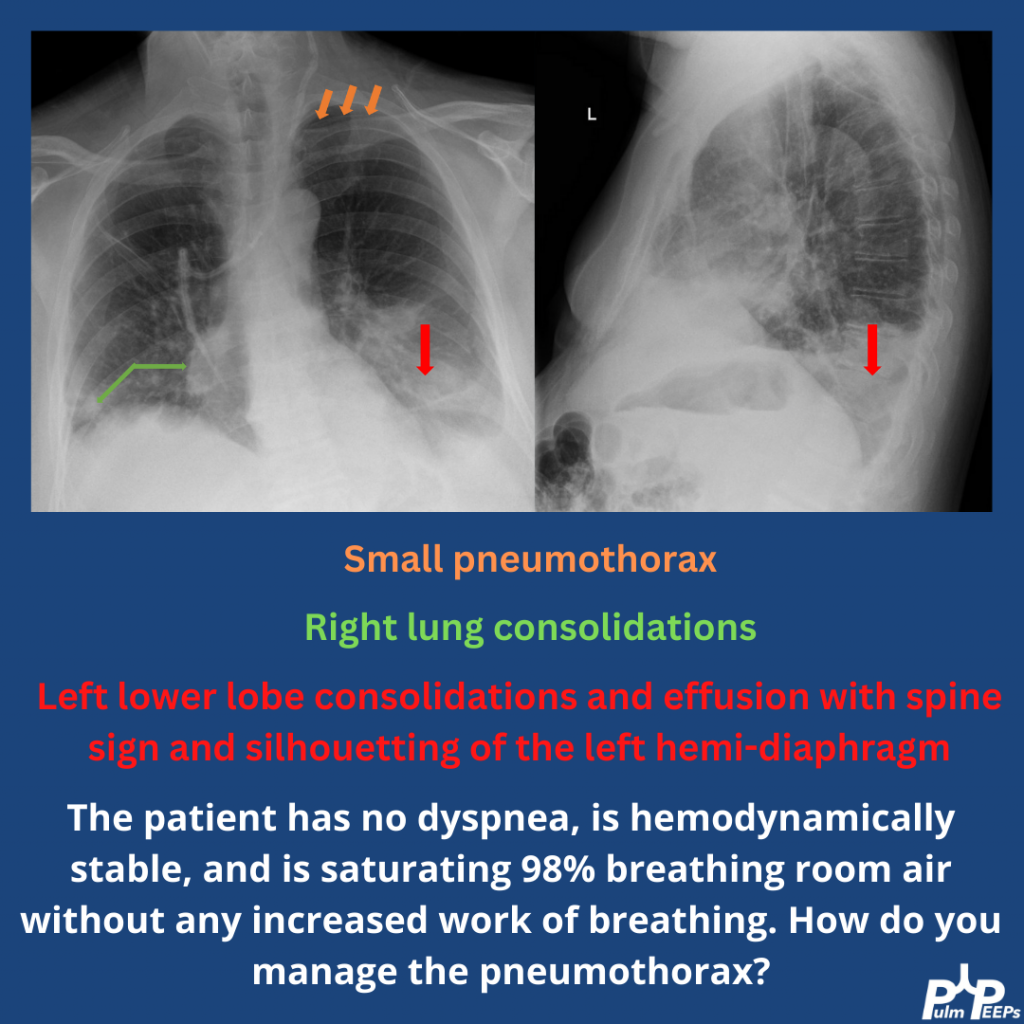
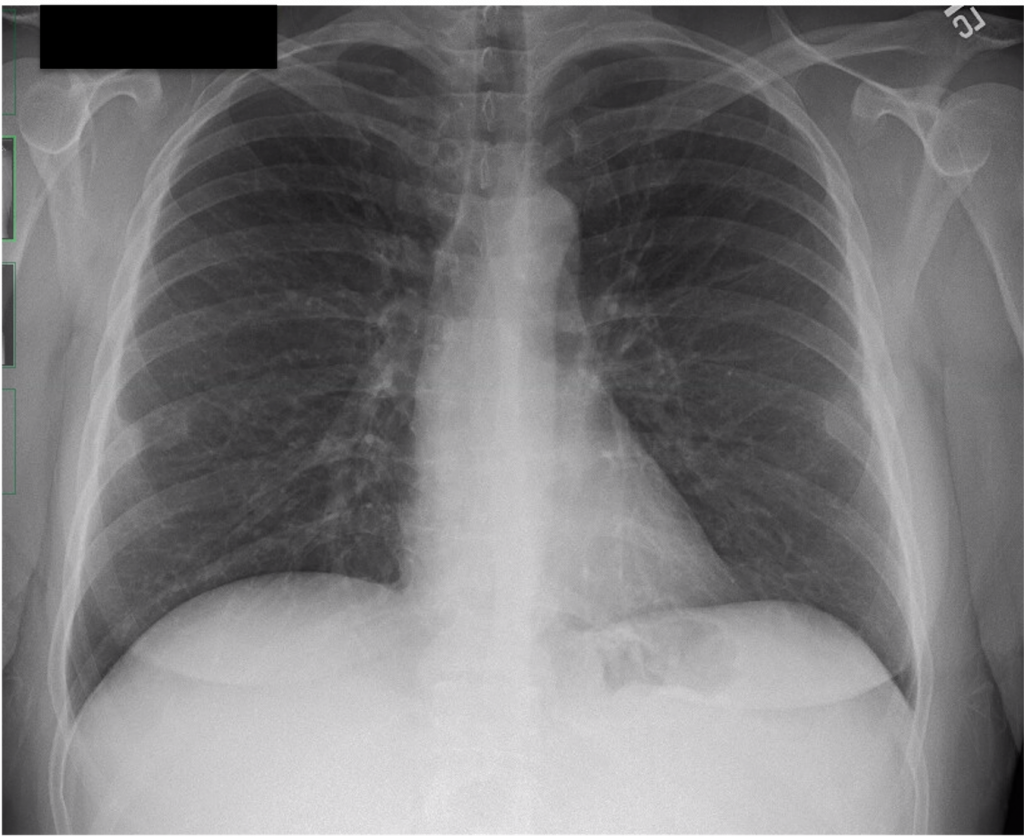
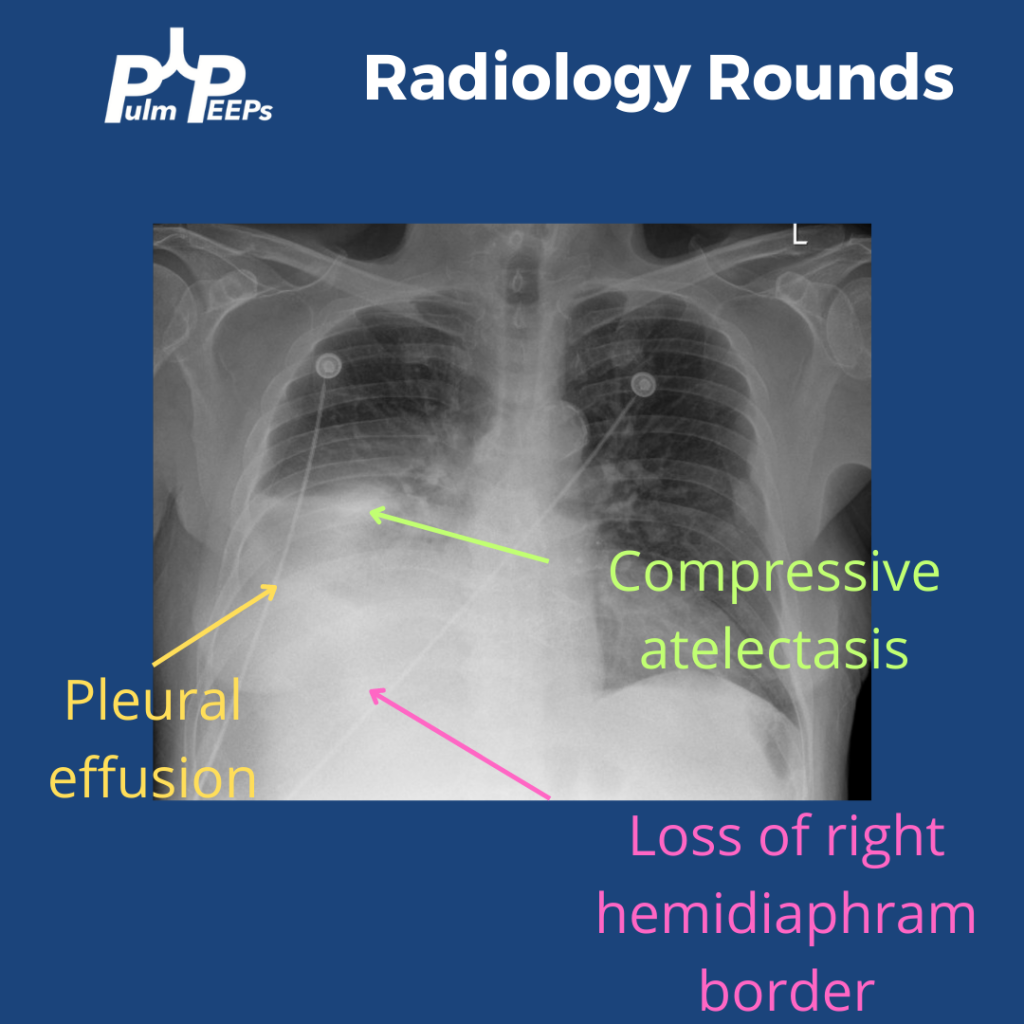
The CXR has a right lower opacity decreasing in density that is silhouetting the right hemi-diaphragm without signs of volume loss on the right concerning for pleural effusion. There is also associated atelectasis adjacent to the effusion
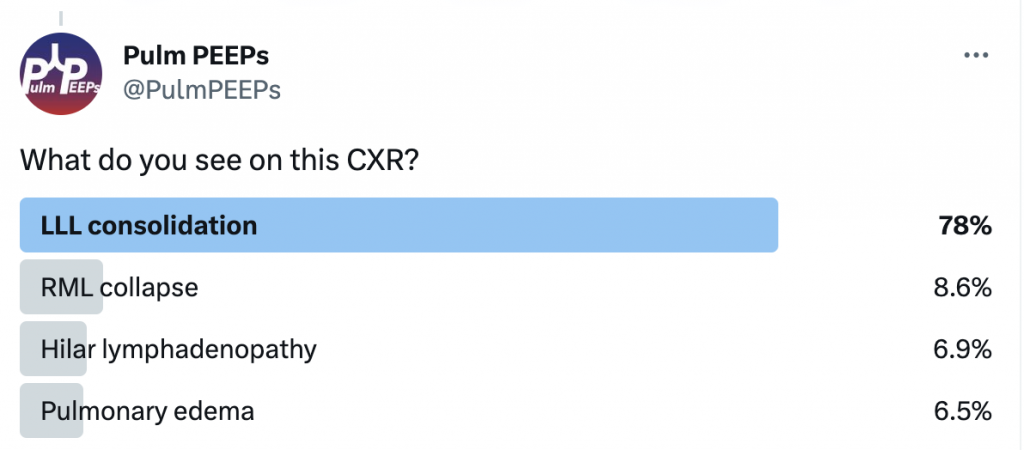
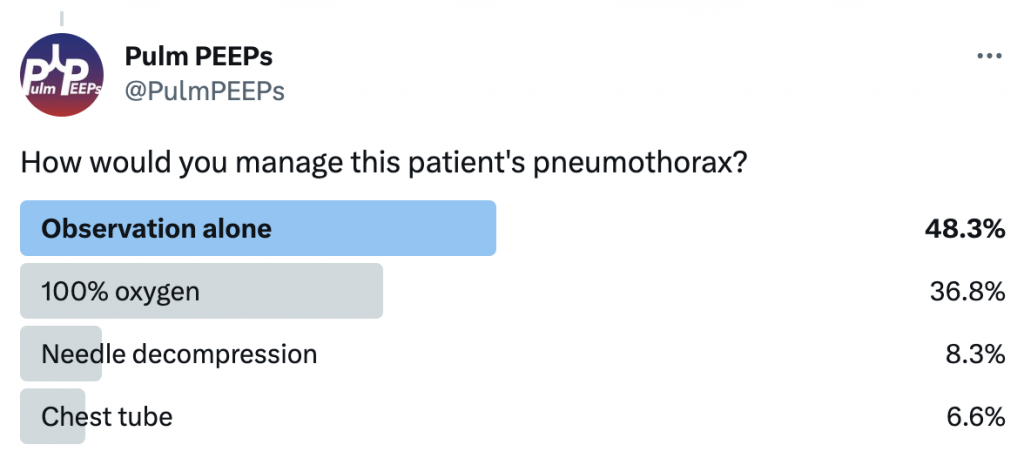
What is your next step for this patient?
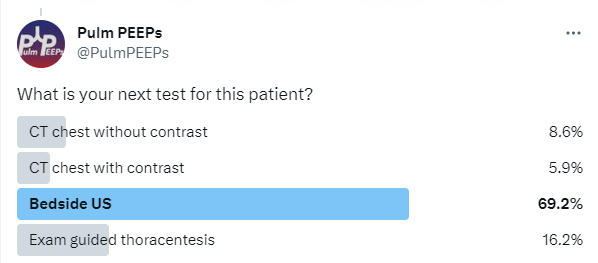
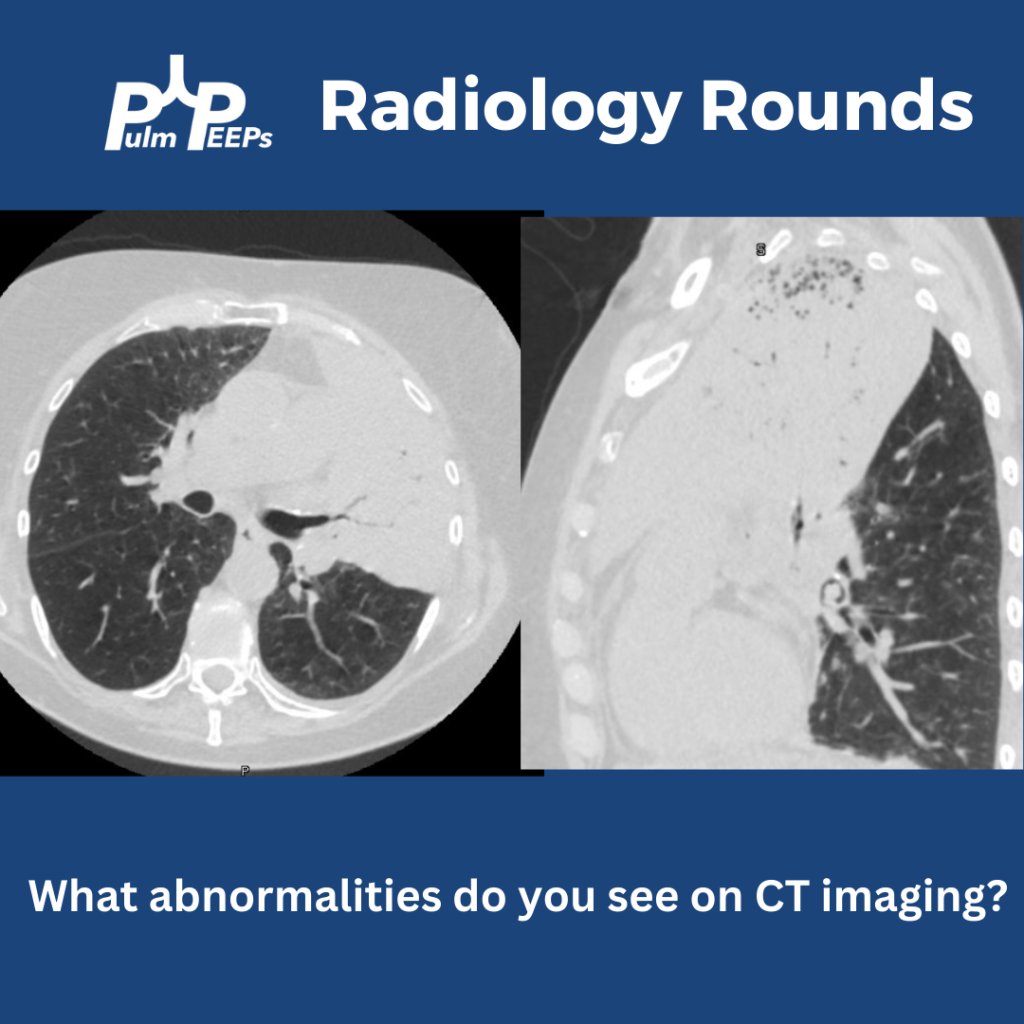
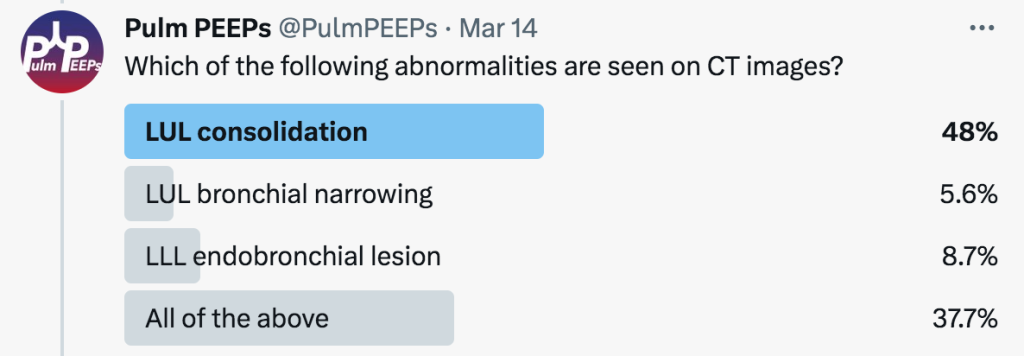
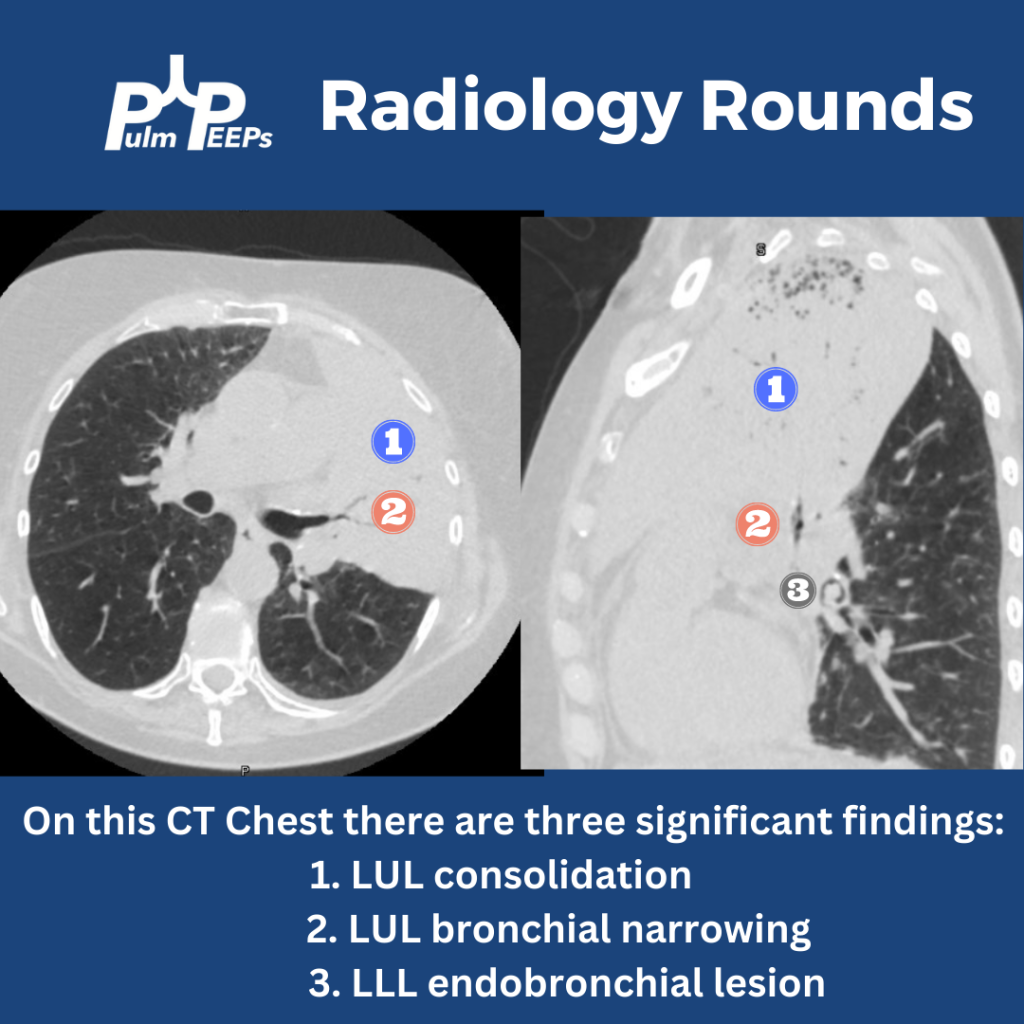
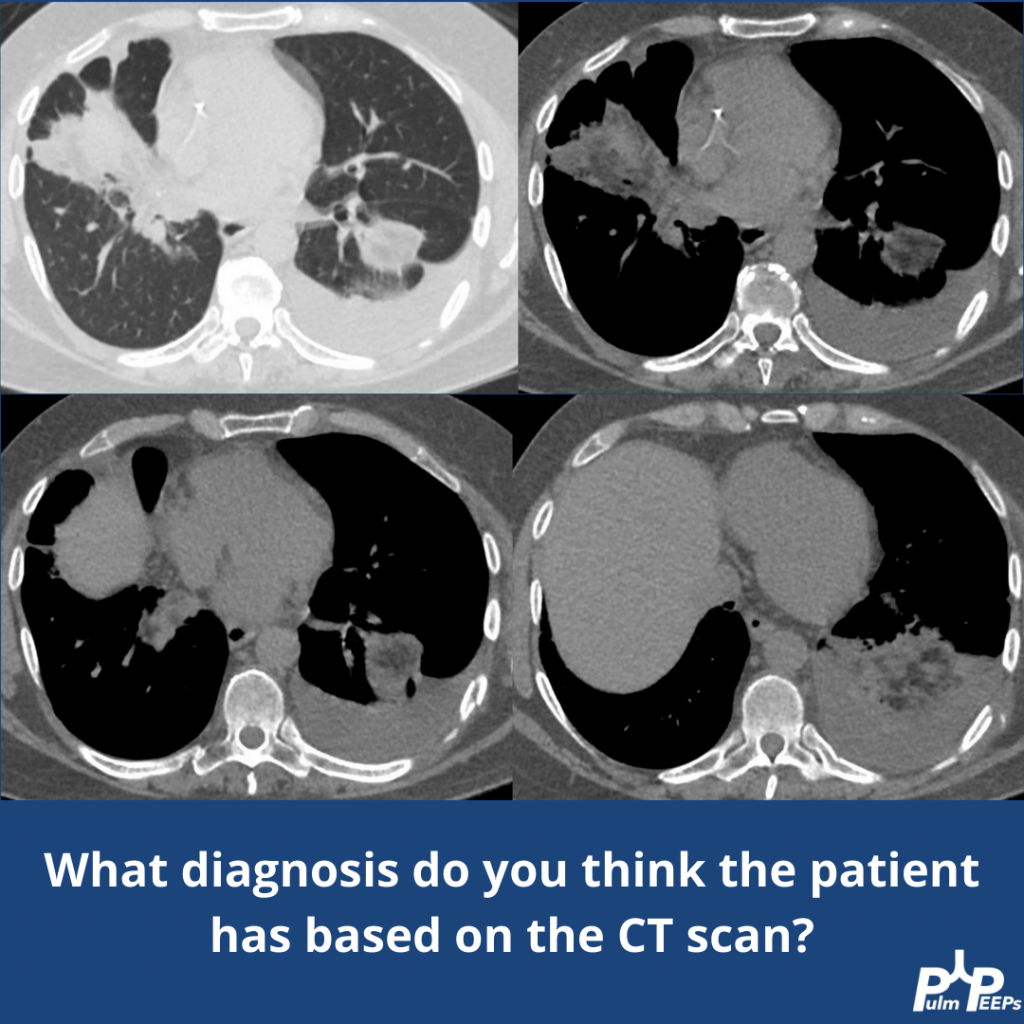
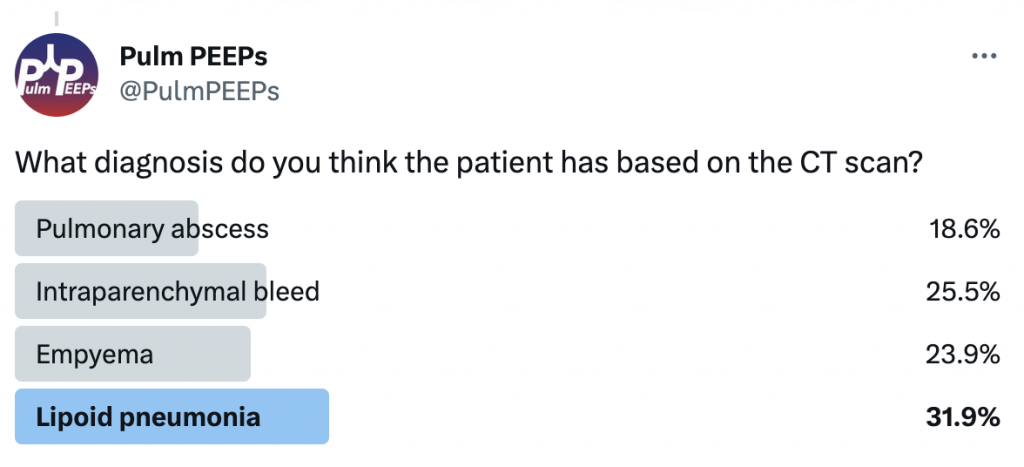
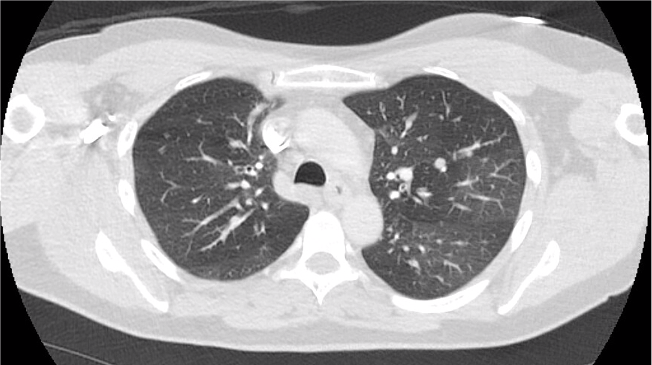
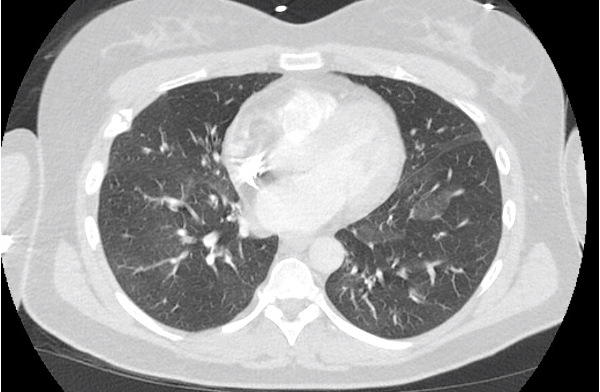
This patient had a bedside POCUS revealing a simple pleural effusion and abdominal ascites. He also had a CT scan performed:
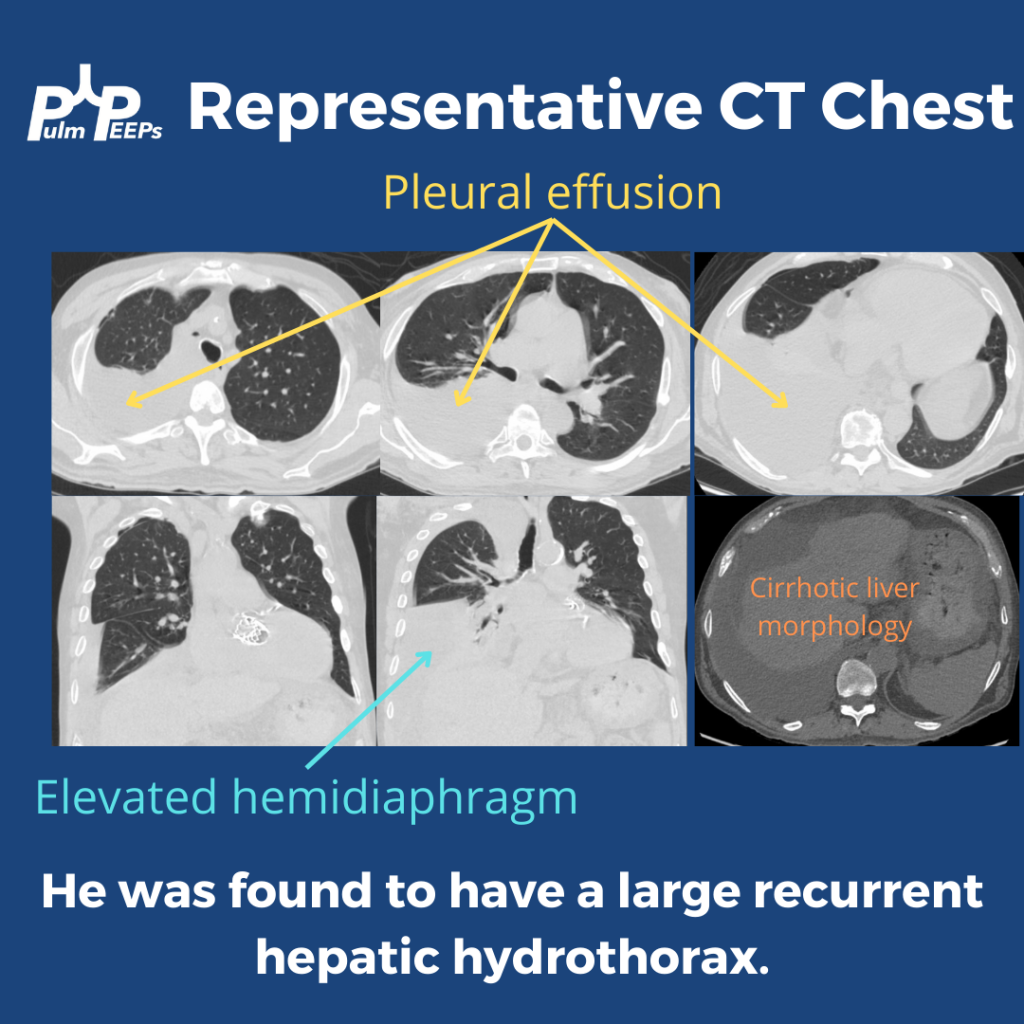
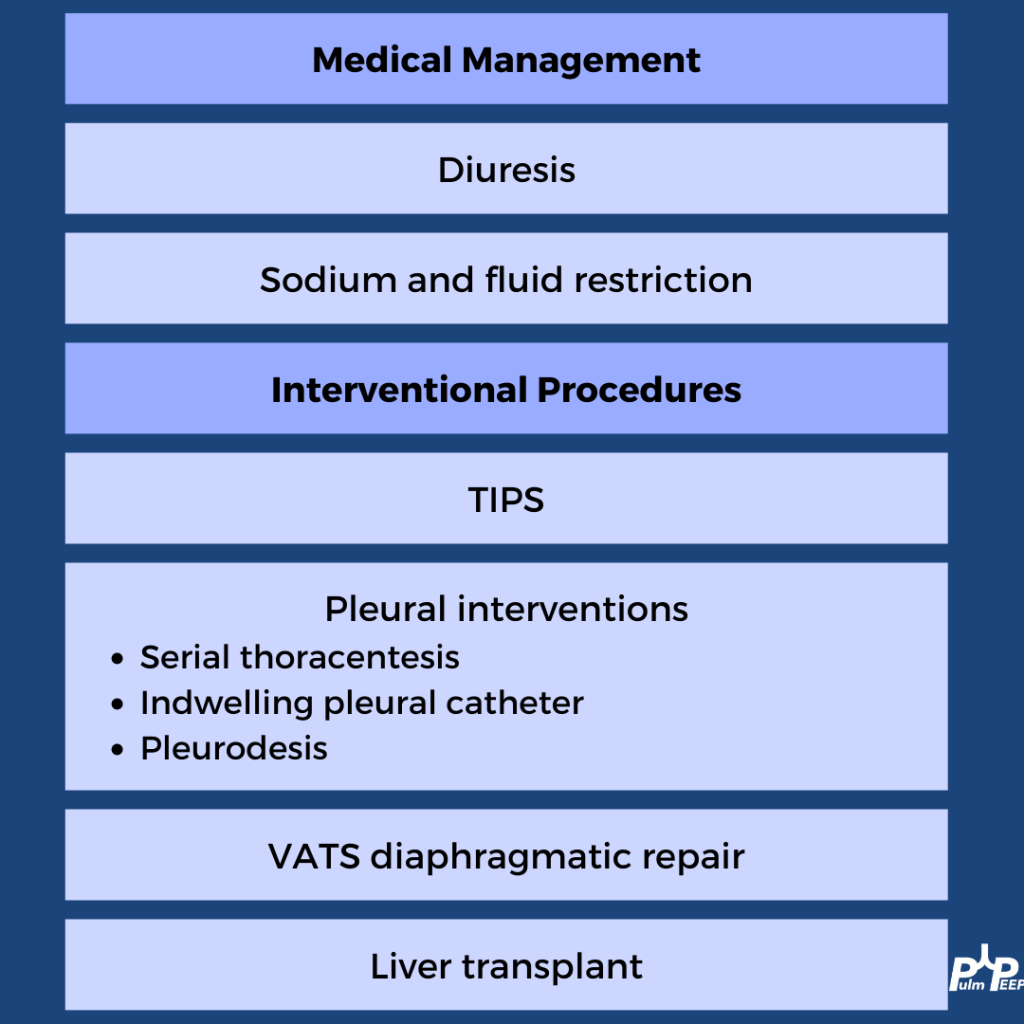
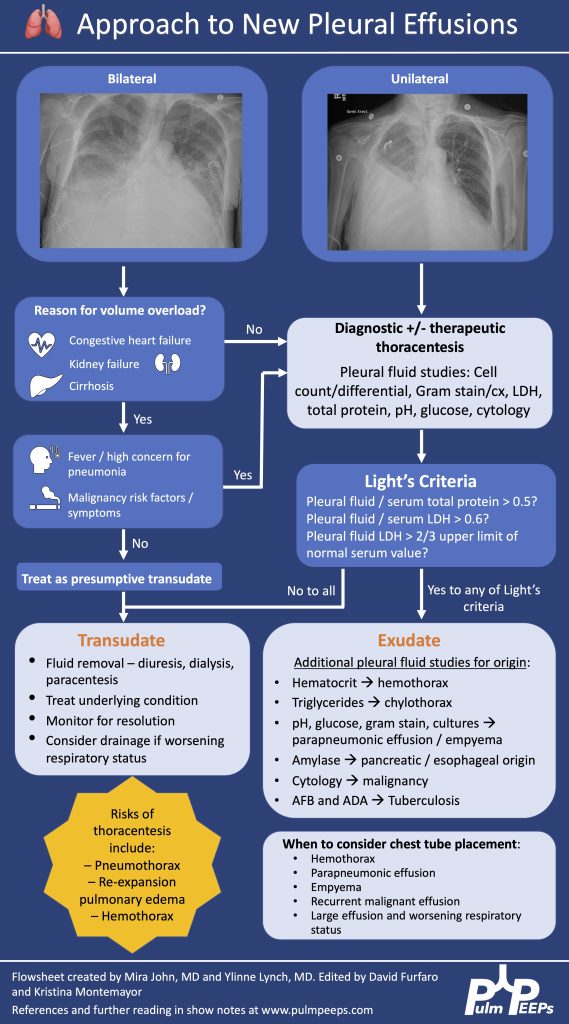
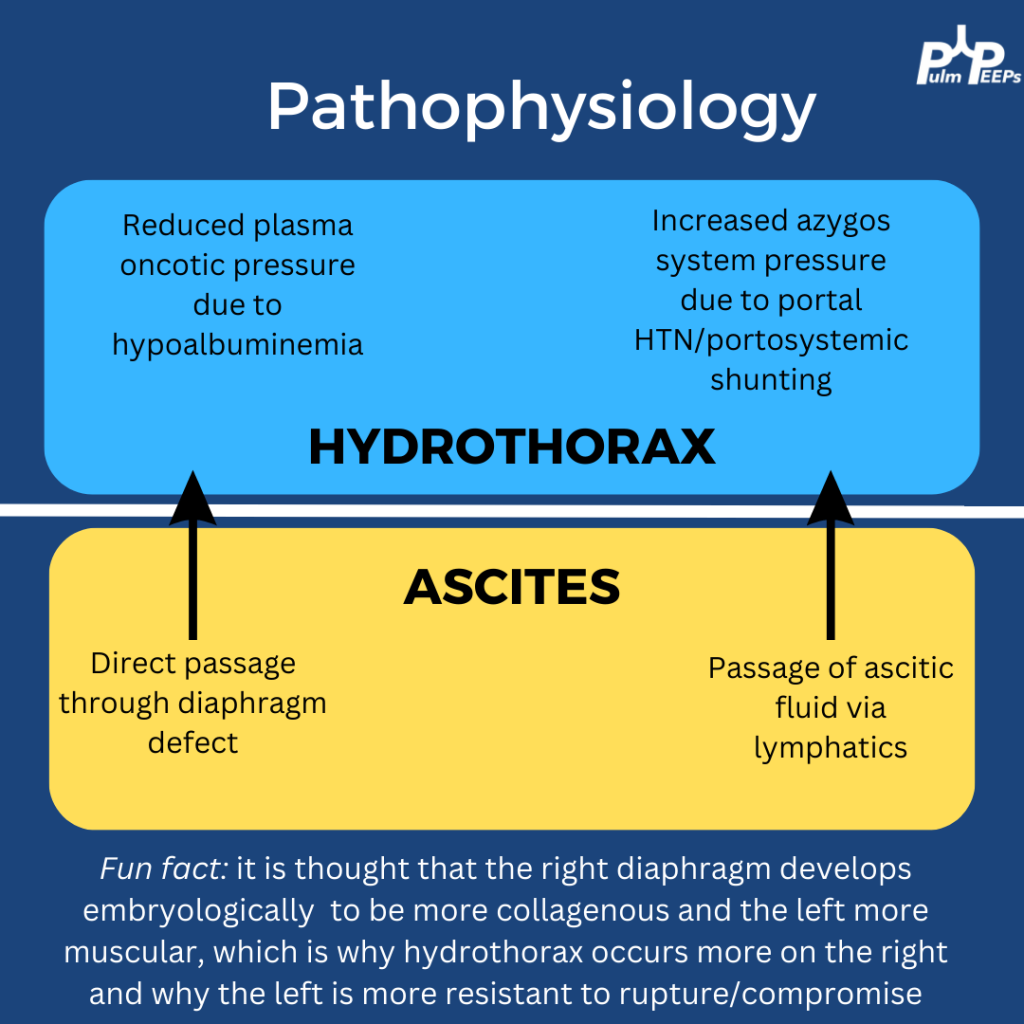
Based on his imaging and history, the most likely diagnosis on the differential was a hepatic hydrothorax. Here is some more information on hepatic hydrothoraces:
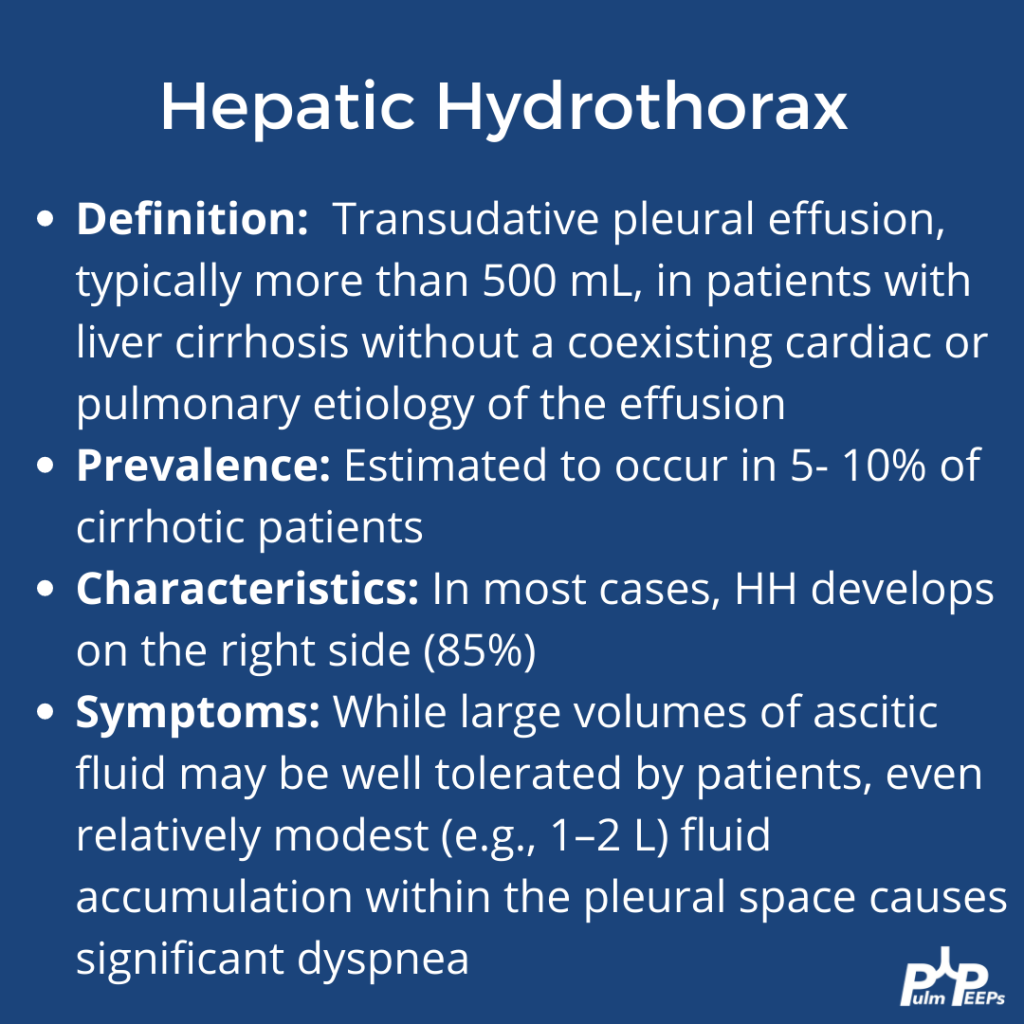
A transudative effusion was confirmed on thoracentesis, and no other clear etiologies were identified The treatment of hepatic hydrothorax should always start with medical management of volume overload in cirrhosis. Pleural procedures can be used for disease that is refractory