We’re excited today to launch our first episode in collaboration with the Irish Thoracic Society and their podcast series. The Irish Thoracic Society represents respiratory professionals throughout Ireland and is dedicated to championing excellence in the prevention, diagnosis, and clinical care of respiratory disease through its work in advocacy, education and research.
In today’s episode, we explore the complex and often overlooked world of refractory chronic cough — a condition that can significantly impact patients’ quality of life but is frequently misunderstood or underdiagnosed. With insights from leading respiratory specialists in Ireland and the United States, we discuss the latest thinking on diagnosis, management, and emerging treatments aimed at improving outcomes for patients and helping clinicians navigate this challenging area of respiratory medicine.
Joining us are renowned experts Professor Lorcan McGarvey and Professor Brendan Canning, both internationally recognised leaders in respiratory medicine and cough research. Together, they share their perspectives on the neurobiology of chronic cough, the considerable morbidity experienced by patients, and how clinicians can approach diagnostic investigations more effectively.
We also explore current treatment strategies and promising new therapies on the horizon as chronic cough increasingly gains recognition as a disease in its own right — rather than simply a symptom. Whether you’re a clinician, researcher, or simply interested in advances in respiratory medicine, this episode offers valuable insights into a condition that is finally receiving the attention it deserves.
Meet Our Co-Hosts
Marissa O’Callaghan is an Irish trained Respiratory fellow currently undertaking a post-doc fellow working in Erasmus MC Rotterdam in the Netherlands. She finished her Irish respiratory and Internal medicine training and Phd in 2025. Her areas of interest are interstitial and rare lung diseases. She enjoys clinical research, Med Ed, and dreaming up new medical innovations. Together with cohost Sandra Green, she founded the ITS podcast series in June 2024. Marissa O’Callaghan –LinkedIn
Sandra Green is an Irish-trained respiratory fellow with a strong track record in climate advocacy and multidisciplinary sustainable initiatives, as co-founder of Irish Doctors for the Environment. She has an MSc in Leadership and Innovation in Healthcare at the Royal College of Surgeons Ireland (2023–2025). With Marisssa, she co-founded the Irish Thoracic Society Podcast Productions, launching the platform in 2024 to share knowledge, insights, and innovations in respiratory care. Sandra Green – LinkedIn
Meet Our Guests
Lorcan McGarvey is a professor of respiratory medicine at the University of Belfast, with a focus on the neurobiology of cough. His research has significantly contributed to the understanding of cough hypersensitivity syndrome and the development of new therapeutic strategies. Lorcan is a respected voice in the field, known for his collaborative work and dedication to advancing respiratory health.
Brendan Canning is a distinguished researcher at Johns Hopkins University, specializing in the mechanisms of cough and airway diseases. His pioneering studies on neural pathways and receptor targets have paved the way for novel treatments in refractory chronic cough. Brendan’s expertise and innovative approach make him a key figure in the ongoing efforts to redefine chronic cough management.
In This Episode
The definitions and classifications of chronic cough, including unexplained, refractory, and unexplained refractory cough
The importance of a thorough clinical history and focused diagnostics over exhaustive testing
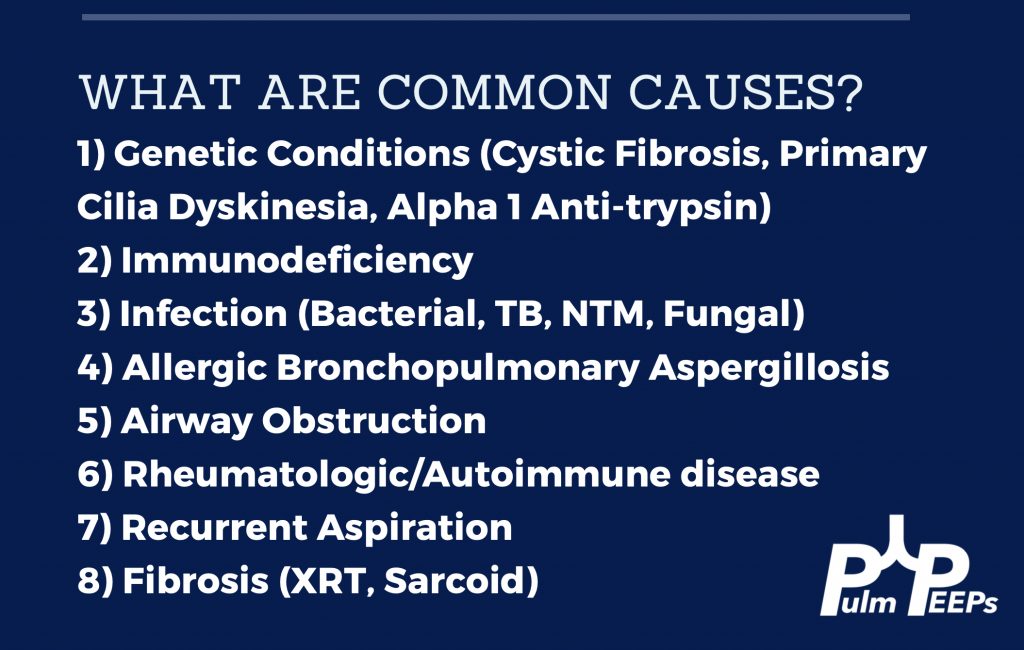
Common causes of chronic cough
The role of personalized, multidisciplinary management—combining pharmacologic, speech therapy, and psychological support—to improve quality of life for even the most challenging patients.
The concept of cough hypersensitivity syndrome and its role in refractory cases
Evidence-based approach to treatment, including pharmacologic and non-pharmacologic options
Emerging therapies on the horizon, including novel receptor modulators and neuromodulatory agents and ongoing clinical trials in this rapidly evolving field
The impact of chronic cough on mental health, social life, and overall quality of life
The importance of reframing chronic cough as a disease entity in its own right
References and Further Reading
Chung KF, Pavord ID. Prevalence, pathogenesis, and causes of chronic cough. Lancet. 2008;371(9621):1364-1374.
Gibson PG, Vertigan AE. Management of chronic refractory cough. BMJ. 2015;351:h5590.
Matsumoto H, Kanemitsu Y, Ohe M, Tanaka H, Terada K, Nishi K, et al. Real-world usage and response to gefapixant in refractory chronic cough. ERJ Open Res. 2025;11(4):01037-2024. doi:10.1183/23120541.01037-2024.
McGarvey LP, Birring SS. Cough hypersensitivity syndrome: a novel paradigm for understanding cough. Lancet Respir Med. 2014;2(8):647-656.
Morice AH, Millqvist E, Bieksiene K, Birring SS, Dicpinigaitis P, Ribas CD, et al. ERS guidelines on the diagnosis and treatment of chronic cough in adults and children. Eur Respir J. 2020;55(1):1901136.
Parker SM, Smith JA, Birring SS, Chamberlain-Mitchell S, Gruffydd-Jones K, Haines J, et al. British Thoracic Society clinical statement on chronic cough in adults. Thorax. 2023;78(Suppl 1):S3-S19.
Smith JA, Woodcock A. Chronic cough. N Engl J Med. 2006;354(2):136-144.
Song WJ, Dupont L, Birring SS, Chung KF, Dąbrowska M, Dicpinigaitis P, et al. Consensus goals and standards for specialist cough clinics: the NEUROCOUGH international Delphi study. ERJ Open Res. 2023;9(6):00618-2023. doi:10.1183/23120541.00618-2023.
Song WJ, McGarvey L, Cho PSP, Mazzone SB, Chung KF, editors. Chronic cough. Sheffield: European Respiratory Society; 2025.
Podcast: Play in new window | Download
Subscribe: Apple Podcasts | Spotify | Amazon Music | Android | iHeartRadio | Podcast Index | RSS