This week we are excited to bring you our podcast cross-over event as we are joined by Eddie Qian and Todd Rice, the co-founders of the ICU Ed and Todd-Cast. Listen today as we discuss the recent ACORN trial evaluating the use of Cefepime versus Pipercillin-Tazobactam in adults hospitalized with acute infection.
This week on Pulm PEEPs, we are excited to be cross-posting an episode that Dave Furfaro did on the ATS Breathe Easy Podcast. Listen to hear a discussion about the best way to create a positive learning environment in the ICU, and how to effectively prepare bedside teaching for learners of all levels.
Meet The Host
Matthew Stutz hosted this episode of the ATS Breathe Easy Podcast. He is an Attending Pulmonary and Critical Care physician at Cook County Health and an Assistant Professor at Rush University. He is a dedicated educator and an active member of the American Thoracic Society.
Key Learning Points
Empowerment: It’s crucial to empower both learners and teachers in an educational setting.
Open Communication: Learners should be encouraged to express their discomfort or challenges in learning. This will allow teachers to adapt and create a more effective learning environment.
Self-awareness and Continuous Improvement: Teachers should be self-aware and continuously strive for improvement. If a teacher knows their weak points or areas they want to enhance, such as bedside teaching or teaching on rounds, they should communicate this to their team. This will make the team more observant and supportive in giving feedback.
Honesty: A genuine and honest dialogue helps in building a strong and trusting educational relationship. It’s beneficial for both the teacher and learner to be candid about their needs and challenges.
Feedback Mechanism: Constructive feedback is an essential part of growth. By informing team members of areas you’re working on, you can receive specific and helpful feedback at the end of a rotation or session.
Appreciation: It’s important to appreciate and acknowledge contributions in an educational or collaborative setting.
We are thrilled to spend time with Dr. Jessica Zitter who is an expert in critical care and palliative care medicine, author, speaker, and documentary filmmaker. We are honored to have her join the show today to discuss her work on improving end-of-life and humanistic care as well as promoting conversations about death and dying.
Meet our Guest
Dr. Jessica Zitter received her medical degree from Case Western Reserve University Medical School, and her MPH from UC Berkeley. She completed her IM residency at BWH, her pulmonary and critical care training at UCSF, and is additionally board certified in Palliative Care. She is an author of multiple essays and articles that have appeared in publications ranging from the NY Times to the Journal of the American Medical Association, has authored a book, and is a documentarian whose work is Emmy and Oscar nominated.
Dr. Zitter’s first book, Extreme Measures: Finding A Better Path to the End of Life, offers an insider’s view of intensive care in America today and its impact on how we die. Her work is featured in the Oscar and Emmy-nominated short documentary Extremis, available to view on Netflix. She has also produced and directed the award-winning, 2020 short documentary Caregiver: A Love Story. Dr. Zitter is currently working on her third film, The Chaplain of Oakland, which explores the devastating problem of racial healthcare inequities at the end of life. She has also founded the production and education non-profit, Reel Medicine Media.
We are extremely excited to be hosting this episode in collaboration with CardioNerds! We have known Amit and Dan for many years, and they have been huge supporters of Pulm PEEPs, so it is an honor to address a topic we’re all interested in together.
We are joined by experts in the field today to discuss acute, decompensated right ventricle failure in patients with Pulmonary Arterial Hypertension (PAH). This topic can be quite intimidating, so we hope this will serve as a valuable guide for anyone who encounters a patient like this in the ICU.
Meet Our Guests
Leonid “Leon” Mirson is an internal medicine resident at the Johns Hopkins Hospital Osler Medical Residency and an Associate Editor here at Pulm PEEPs. He was born in Ukraine and moved to Philadelphia in early childhood with his family. He received his undergraduate degree from the University of Pittsburgh where he studied biomedical engineering and received his medical degree from the University of Pittsburgh School of Medicine. His current interests include pulmonary and critical care medicine with a focus on pulmonary hypertension as well as medical education. He is a rising PCCM fellow at the University of Pennsylvania.
Bhavya Varma completed her medical school at the University of Pittsburgh, her internal medicine residency at Johns Hopkins, and is a rising Cardiology fellow at NYU. She is interested in medical education and has done work with CardioNerds during her residency.
Mardi Gomberg-Maitland is a Professor of Medicine at George Washington University. She serves as the Medical Director of the Pulmonary Hypertension Program at George Washington Hospital. She completed her medical degree at Albert Einstein College of Medicine, completed her residency at the Weill-Cornell Medical Center, and completed her fellowship in cardiovascular diseases at Mount Sinai Medical Center. Her research focus is on understanding the epidemiology of pulmonary hypertension and the development of novel therapeutics and biomarkers. Dr. Gomberg-Maitland is internationally known for her work, she has had extensive grant funding and has published over 150 articles, abstracts, reviews, and chapters.
Rachel Damico is a pulmonologist and an Associate Professor of Medicine at Johns Hopkins Hospital, where she is also the Associate Director of the physician-scientist training program. Dr. Damico received her medical degree and doctoral degree in Molecular and Cellular biology from the University of Pennsylvania. She completed her residency in the Osler Internal Medicine training program and continued on as a PCCM fellow at Johns Hopkins. She has quickly achieved an international reputation in the field of pulmonary vascular biology and both basic and translational research, as well as clinical excellence, in Pulmonary Arterial Hypertension.
Patient Presentation
A 21-year-old woman with a past medical history notable for congenital heart disease (primum ASD and sinus venosus with multiple surgeries) complicated by severe PAH on home oxygen, sildenafil, ambrisentan, and subcutaneous treprostinil is presenting with palpitations, chest pain, and syncope. She presented as a transfer from an outside ED where she arrived in an unknown tachyarrhythmia and had undergone DCCV due to tachycardia into the 200s and hypotension. On arrival at our hospital, she denied SOB but did endorse nausea, leg swelling, and poor medication adherence. Her initial vitals were notable for a BP of 80/50, HR 110, RR 25, and saturating 91% on 5L O2. On exam, she was uncomfortable appearing but mentating well. She had cool extremities with 1-2+ LE edema. Her JVP was 15cm H2O. She has an RV Heave and 2/6 systolic murmur. Her lungs were clear bilaterally. Her labs were notable for Cr 2.0, an anion gap metabolic acidosis (HCO3 = 11), elevated lactate (4.1), elevated troponin to 14, and a pro-BNP of ~5000. Her CBC was unremarkable. Her EKG demonstrated 2:1 atrial flutter at a rate of 130.
Key Learning Points
Diagnosing RV failure in patients with PH:
RV dysfunction and RV failure are two separate entities. RV dysfunction can be measured on echocardiography, but RV failure can be thought of as a clinical syndrome where there is evidence of RV dysfunction and elevated right sided filling pressures.
RV failure is a spectrum and can present with a range of manifestations from evidence of R sided volume overload and markers of organ dysfunction, all the way to frank cardiogenic shock. Most patients with RV failure are not in overt shock.
One of the first signs of impending shock in patients with RV failure is the development of new or worsening hypoxemia. Patients with decompensated RV failure approaching shock often do not present with symptoms classic for LV low flow state. Instead, hypoxia 2/2 VQ mismatching may be the first sign and they can be otherwise well appearing. Particularly because patients with PH tend to be younger, they can often appear compensated until they rapidly decompensate.
Causes of decompensation for patients with RV dysfunction and PH:
Iatrogenesis (inadvertent cessation of pulmonary vasodilators by providers, surgery if providers are not familiar with risks of anesthesia), non-adherence to pulmonary vasodilators (either due to affordability issues or other reasons), infections, arrhythmias (particularly atrial arrhythmias), and progression of underlying disease.
Patients with atrial arrhythmias (atrial flutter or atrial fibrillation) and pulmonary hypertension do not tolerate the loss of the atrial kick well as it contributes a significant amount to their RV filling and impacts their cardiac output. It is often difficult to determine if the atrial arrhythmia is a cause or effect of decompensated RV failure, but its presence is associated with a worse prognosis. Efforts should be made to re-establish normal sinus rhythm in patients with decompensated RV failure and atrial arrhythmias.
A patient’s home PH medications should never be stopped for any reason upon admission unless on the basis of recommendations by a pulmonary hypertension provider as this is often a cause of decompensation inpatient
Interpreting findings on echocardiogram:
Echo is a useful screening tool. When interpreting evidence of RV dysfunction, it is important to look at the global picture and not just one measurement.
RVSP, though commonly reported, may be of limited value when evaluating for decompensation. It’s a function of blood pressure, heart rate, and cardiac output. RVSP may even decline as shock worsens.
TAPSE is useful as a marker of RV dysfunction if it is reduced, but it is difficult to follow over time and only gives information about cardiac function around the annulus; it may be normal even when apical RV function is depressed. RV fractional area of change may be more useful for global RV function. It is important to pay attention to the RV size overall, the degree of TR, and the presence of effusion all of which are associated with RV dysfunction.
Tips regarding the interpretation of invasive hemodynamics:
Cardiac output by thermodilution is the standard way to calculate PVR. Despite the degree of TR that is typically present, it is thought to be a better representation of cardiac output than the estimated Fick calculation.
Our experts agree that routine monitoring of invasive hemodynamics for acute decompensated RV failure is likely not helpful and has significant risks. A good external volume exam or CVP off a central venous catheter + central venous saturation will likely be all you need to navigate a patient with shock secondary to RV failure. A right heart catheterization (should be only done under fluoroscopy for patients with large RVs) may be helpful if the etiology of shock is unclear.
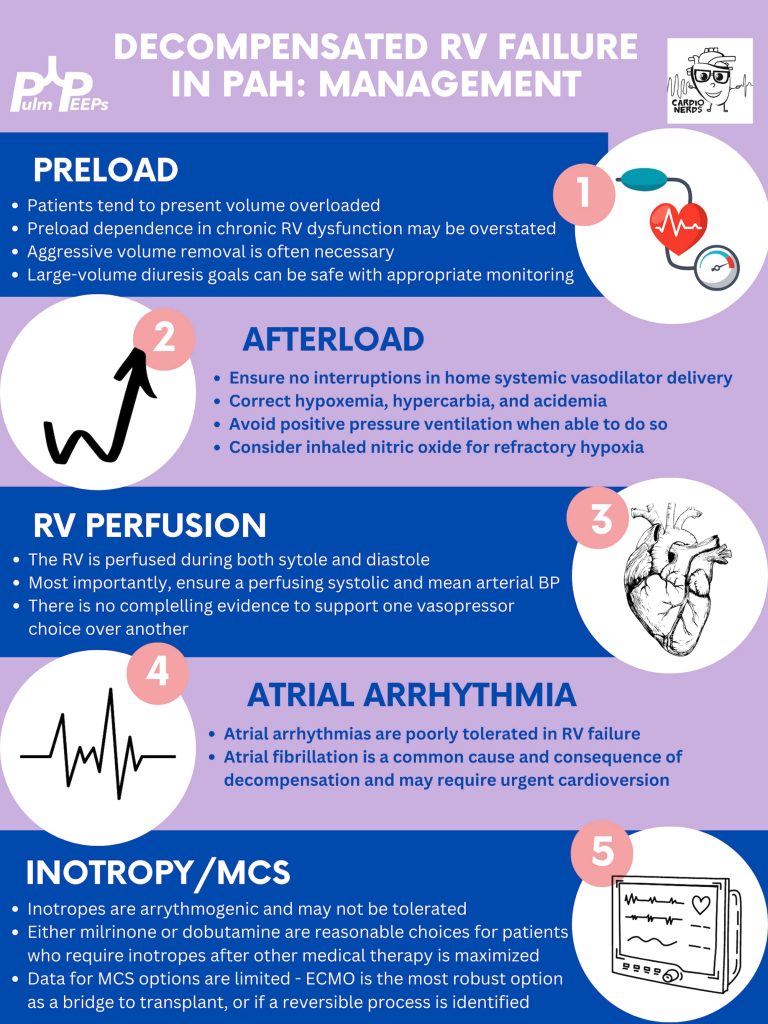
Management of decompensated RV failure in patients with pulmonary hypertension
Managing preload is of utmost importance, perhaps the most important tenant of management of decompensated RV failure. The overwhelming majority of patients with PH and decompensation are volume overloaded, it is exceptionally rare that someone would be dry. Furthermore, the myth that the RV is “preload responsive” is only true in the setting of acute RV injury (eg. RV infarction) and not so in patients with acute on chronic RV dysfunction. It is important to optimize preload in someone in decompensated RV failure and it is safe to do this more rapidly than traditionally taught. Exact goals varied between our experts, but anywhere from 2-4L net negative per day is reasonable especially if the patient is hemodynamically tolerating the fluid removal. If the patient is not responding to diuretics, hemodialysis with ultrafiltration may be necessary to optimize the patient.
Afterload is the next tenant of management. Optimizing the following parameters will reduce the patient’s pulmonary vascular resistance and reduce afterload to the right ventricle.
— Avoiding hypoxic pulmonary vasoconstriction, liberalize the patient’s O2 goal
— Avoid permissive hypercapnia and academia in this patient population
— Do not withhold a patient’s pulmonary vasodilator until discussion with the PH team. If stopped inadvertently, restart this medication immediately. For patients with malfunctioning pumps, there is a phone number on the back that you can call for rapid troubleshooting. Sildanefil can be given IV if a patient is NPO.
— Inhaled nitric oxide can improve oxygenation and reduce afterload
— Intubation and mechanical ventilation greatly increase PVR and are poorly tolerated. Exacting care must be taken to titrate PEEP and tidal volume, and avoid intubation when possible.
— Starting a new systemic pulmonary vasodilator in decompensated RV failure may be considered under close guidance from the pulmonary hypertension team
Management of atrial arrhythmias:
As above, patients with severe pulmonary hypertension do not tolerate loss of sinus rhythm well. If they are decompensated, every effort should be made to re-establish normal sinus rhythm.
Management of RV perfusion:
Unlike the LV, the RV is perfused during BOTH systole and diastole. Maintaining effective coronary perfusion to the RV is essential in RV failure. For this reason, the systemic systolic pressure (as well as the mean arterial pressure) should be kept high enough to ensure that the RV is able to perfuse. There is no great body of evidence as to which pressor works best. Norepinephrine, vasopressin, and even phenylephrine are all reasonable choices to maintain appropriate perfusing blood pressure.
Inotropy:
Patients in shock and RV failure do not always require inotropes, but if they do it’s often a sign of a grim prognosis. Either dobutamine or milrinone is reasonable, but the negative effects of these drugs (arrhythmias, tachycardia, and systemic hypotension) may limit their uses.
Mechanical circulatory support:
Limited options are available. Balloon pumps and Impella devices have limited roles except in expert centers, and ECMO remains the standard of care. ECMO (either V-V or V-A) may have utility as a bridge to recovery if a reversible cause is identified, or a bridge to transplant if the patient is on the transplant list.
Goals of care:
The prognosis of a patient admitted to the ICU with acute on chronic decompensated RV failure is guarded, with very high mortality rates even if not in shock
It is important for the patient’s longitudinal pulmonary hypertension provider to discuss the prognosis and goals of care ahead of time but this is not always possible. If they are admitted, early discussions regarding code status and prognosis are essential. It may be helpful to bring in the patient’s longitudinal pulmonary hypertension doctor into these discussions if possible.
We’re podcasting again today from #ATS2023! Yesterday, we heard all about the conference in general, with some great recaps and previews of the remaining sessions. Today, we are coming to you in collaboration with the Critical Care Assembly to preview one of the symposiums they are hosting. This session is about Cardiac Arrest: New Science and Changing Guidelines and is happening today (the day of podcast release, 5/23/23)! If you’re interested in hearing more after the episode then please plan to attend at 2:15 PM in Room 150 A-B.
For those of you who aren’t at the conference, or couldn’t make this session, we’ll talk about some of the key points and discussion topics. We will additionally be talking to the chairs of other symposiums over the next coming months so stay tuned for some more highlights from ATS 2023.
Meet Our Guest
Ari Moskowitz is an Assistant Professor of Medicine at Montefiore Medical Center / Albert Einstein College of Medicine. He is additionally the MICU Director at Montefiore Einstein and Director of Critical Care Quality Improvement. He is an NIH-funded researcher and has conducted research in cardiac arrest care, sepsis, and ARDS.
Meet our Collaborators
The American Thoracic Society Critical Care Assembly is the largest Assembly in the American Thoracic Society. Their members include a diverse group of intensivists and care providers for both adult and pediatric critically ill patients. The primary goal of the Critical Care Assembly is to “improve the care of the critically ill through education, research, and professional development.”
Join us as we head to Indiana University! Listen in as we discuss another great case and hear teaching points from our amazing guests.
Meet our Guests
Parth Savsani is currently an internal medicine resident at Indiana University School of Medicine. He received his undergraduate degree from the University of Wisconsin-Madison and his medical degree from the University of Illinois College of Medicine. He enjoys medical education and was selected to be the VA chief resident next year.
Maria Srour is a Pulmonary and Critical Care Fellow at Indiana University School of Medicine. She completed her internal medicine residency at Saint Louis University where she was also a chief resident, and received her medical degree from IU. She works in global health to improve care for sepsis patients in low resources settings, and is currently pursuing her MPH.
Laura Hinkle is a Indiana University die hard and has been there from her since medical school through residency and fellowship, and is now an Assistant Professor of Clinical Medicine and the Associate Program Director for the Pulmonary and Critical Care Medicine Fellowship. She will be taking over as the Program Director July 1, 2023. She is a dedicated educator and is the Key Clinical Educator for Pulmonary and Critical Care, and the Director of the Clinical Transitions Curriculum. Additionally, she is working on a Master’s Degree in Education through the University of Cincinnati.
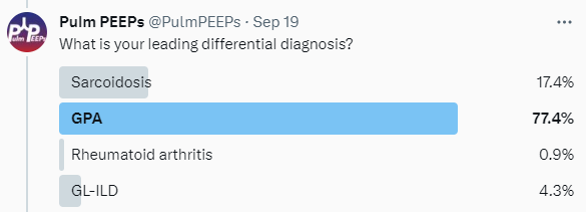
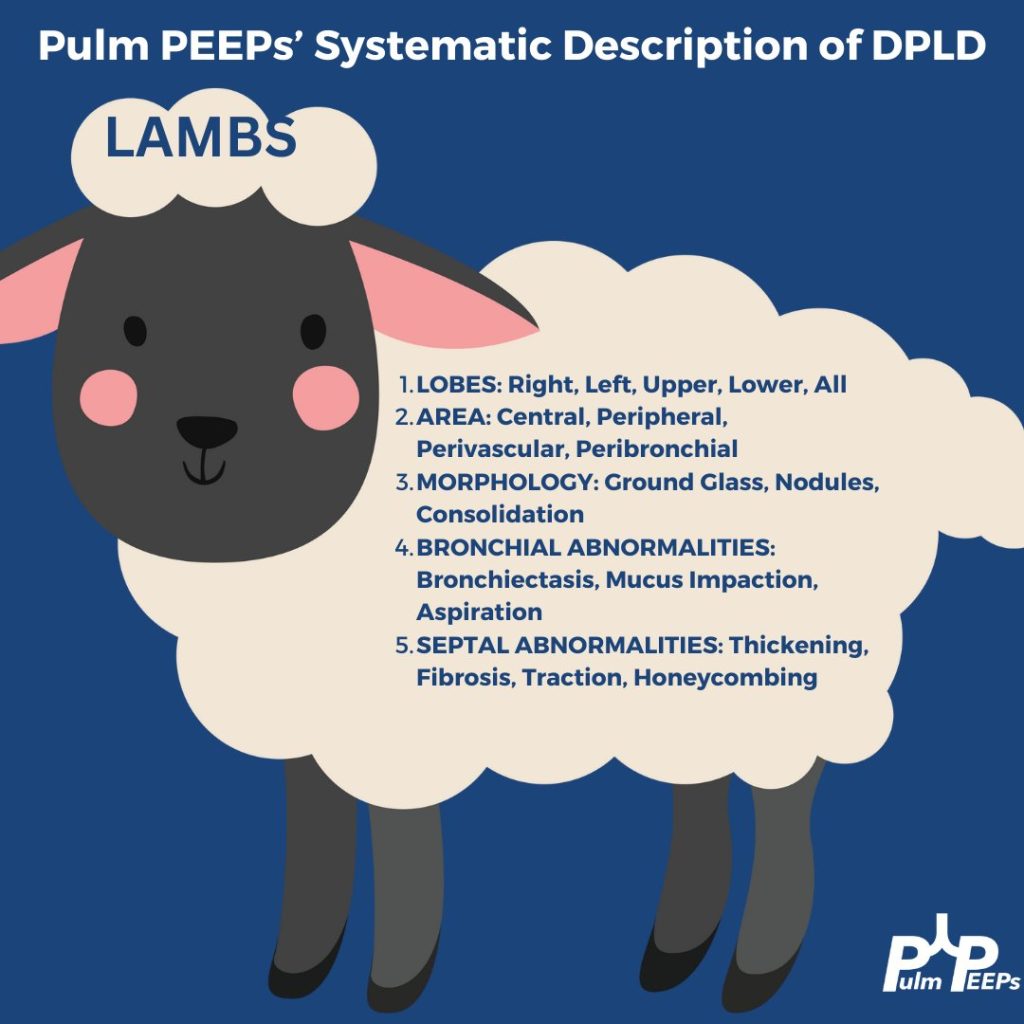
Case Presentation
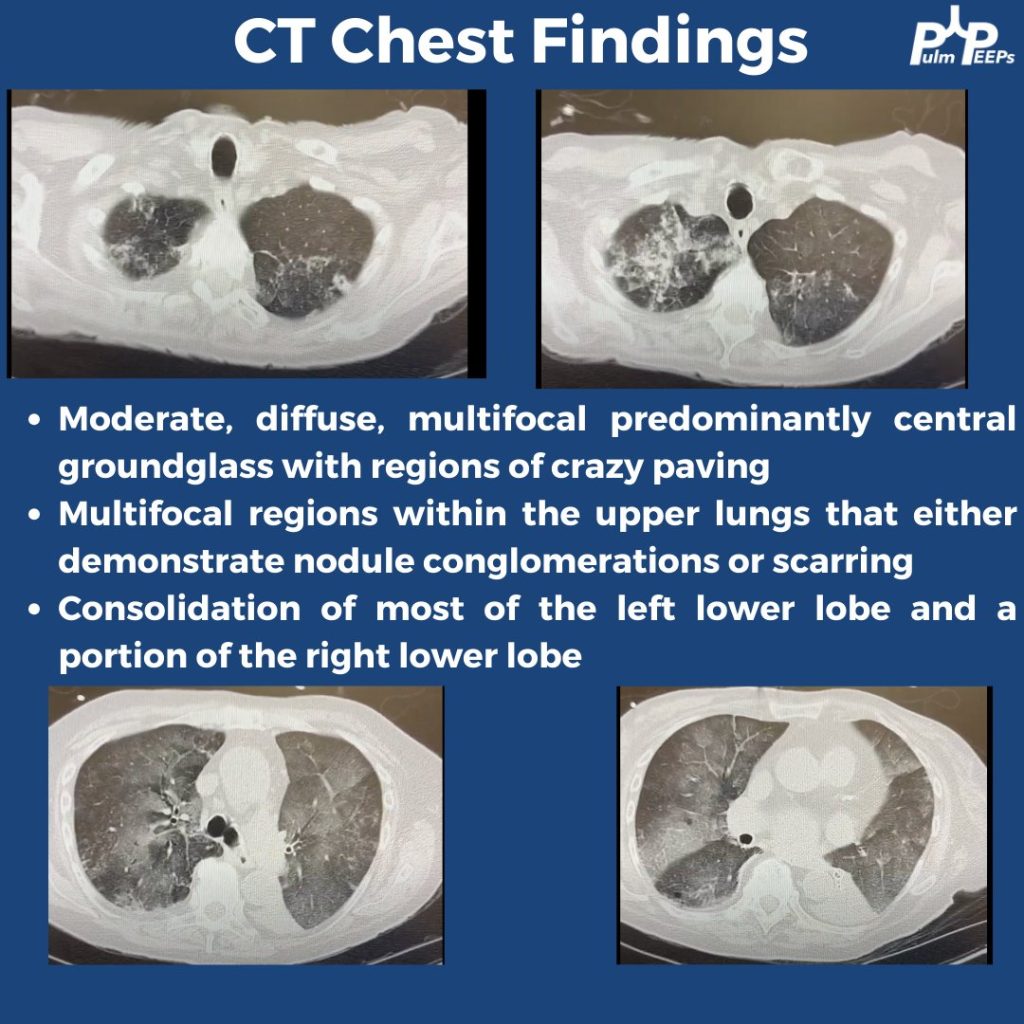
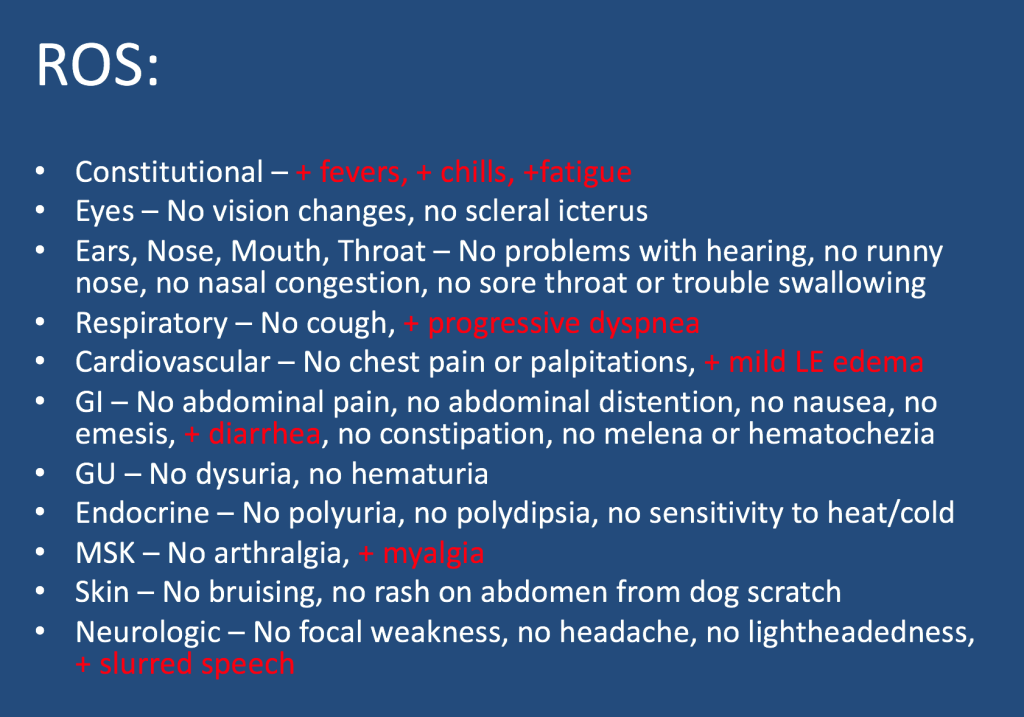
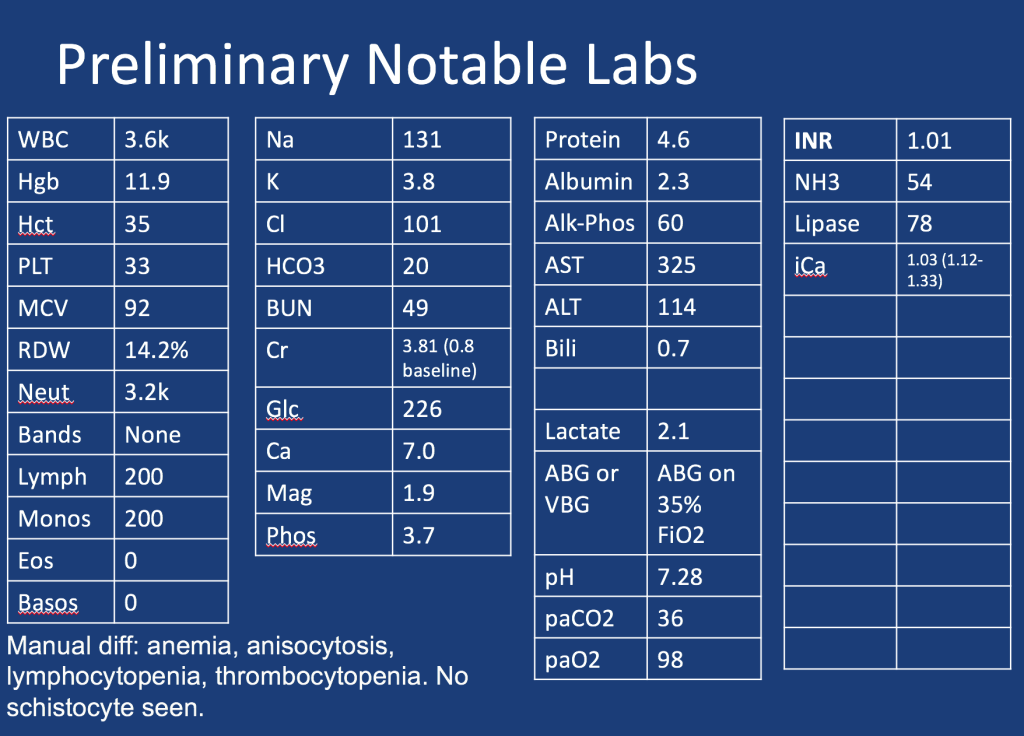
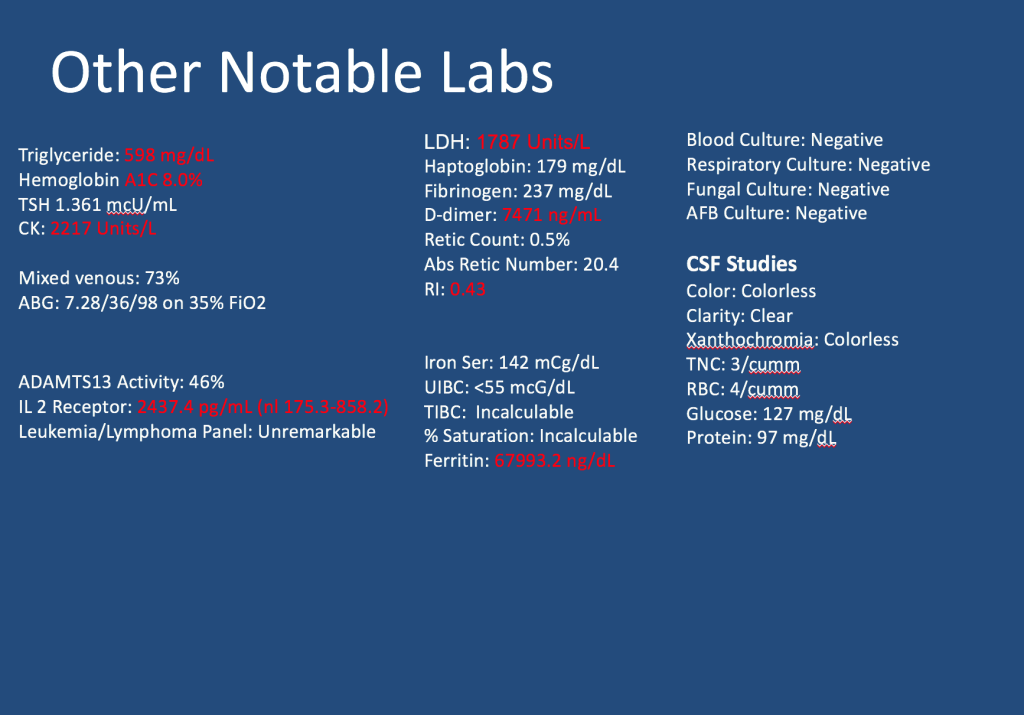
A male in her early 60s is transferred from a neighboring facility with a 1 week history of fatigue and lethargy. Three days prior to presentation he developed dyspnea and increased weakness with a near fall at home. HIs family also reported recent fevers, chills, dyspnea, and diarrhea. On his way to seek evaluation, he developed slurred speech without any other focal abnormalities.
Additional information is summarized as below:
Follow along our episode to hear the final diagnosis and key teaching points from the case!
For “#RadiologyRounds” today, we won’t be looking at any imaging, but we’ll be looking at some vent wave forms and examining dysynchrony! This is a re-booted @david_furfaro Tweetorial. I hope you enjoy and this is an open invitation for all dysynchrony waveforms!
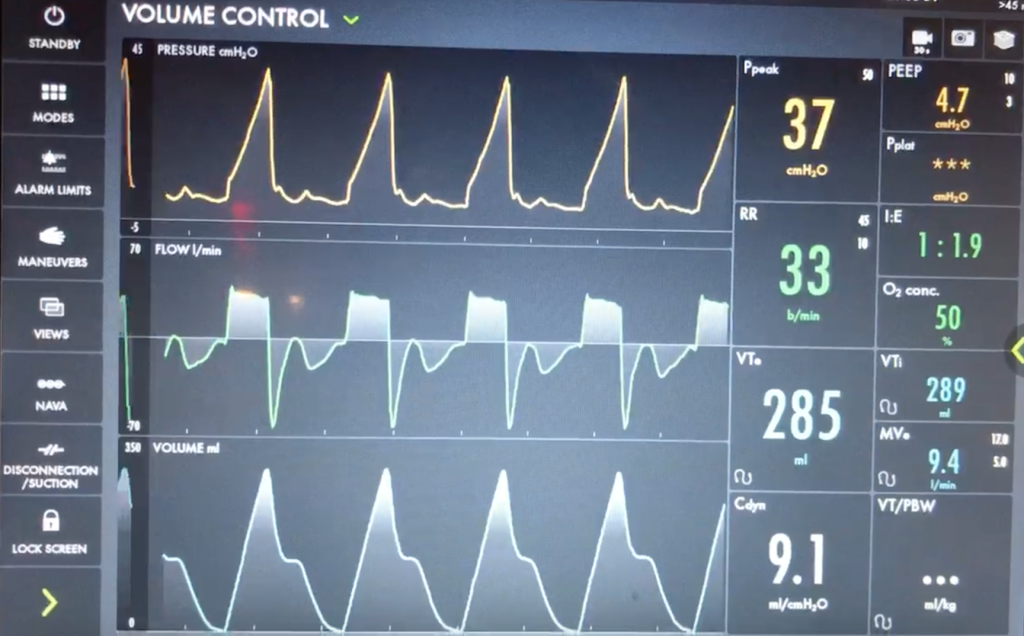
A 40s M is intubated for ARDS. In order to maintain lung protective ventilation, he was on high does of propofol, fentanyl and midazolam. His sedation is being weaned slightly now, and the RN calls for vent dysynchrony. His ventilator looks like this
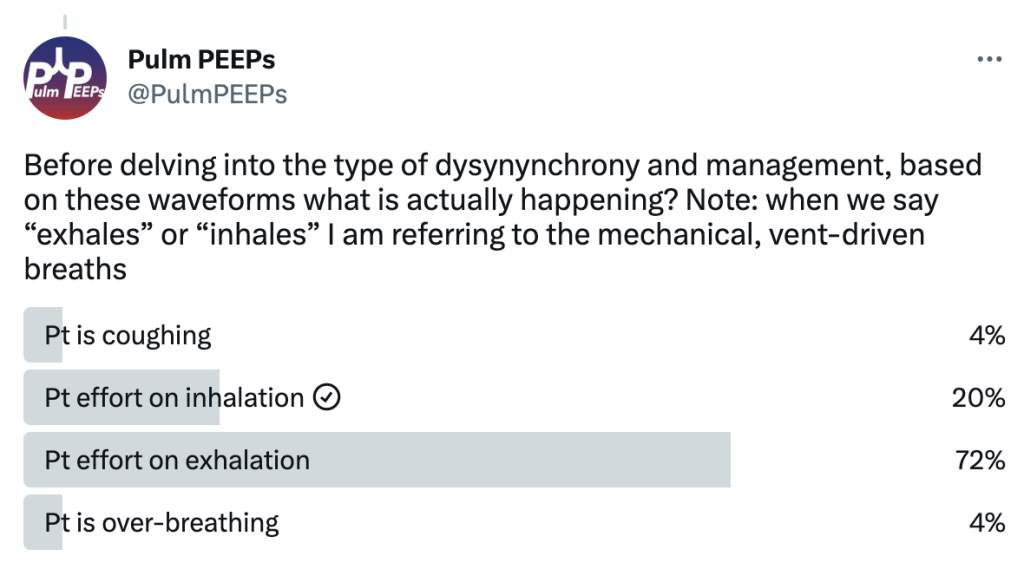
Before delving into the type of dysynynchrony and management, based on these waveforms what is actually happening? Note: when we say “exhales” or “inhales” I am referring to the mechanical, vent-driven breaths
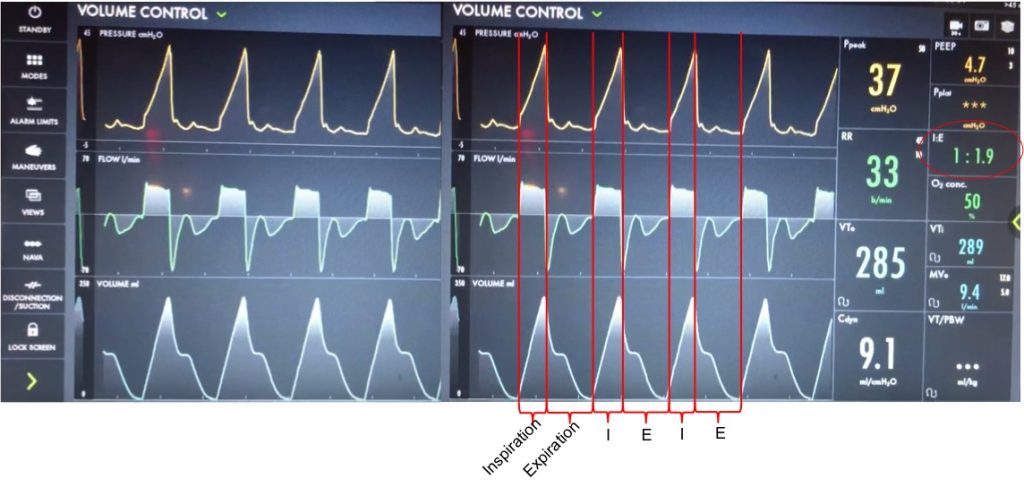
Let’s take a look at the waveforms and identify the phase of breathing. This is VC with a square flow waveform, so as a set volume is delivered, the flow is at a constant rate, and the pressure is measured. Expiration is about 2x as long as inspiration (determined by I time or flow rate)
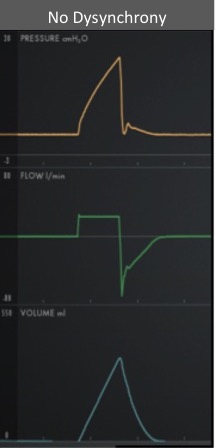
With a passive patient (no dysynchrony) after inspiration, the volume curve should show a smooth decrease with exhalation, the pressure curve should flatten to the set PEEP, and the flow will be negative and gradually return to 0 as the patient exhales
In our case, you can see simultaneous dysynchrony in all three waveforms during exhalation (red arrows) vs normal (orange lines). There is a pressure negative deflection; the flow quickly rises to 0 before returning to negative; and the volume curve plateaus as exhalation pauses
Putting this together, it means that during expiration there is an inspiratory effort. The patient is trying to inhale, which causes a negative pressure deflection, and a pause in air flowing out of the lungs. If this effort triggered a breath, there could be breath stacking. Notice that the same pattern occurs after every breath, and clinically we said the patient was still heavily sedated. This combination of findings is a type of dysynchrony called REVERSE TRIGGERING or ENTRAINMENT.
You could consider whether this dysynchrony was an ineffective effort, but the trigger sensitivity was low, and the pattern and consistent timing after inspiration is more consistent with reverse triggering.
The change in pressure and flow of a ventilator-initiated, mandatory breath stimulates an inspiratory effort from the patient. Theories differ on if this is mediated by the diaphragm or central respiratory center. This can start during the ventilator-delivered breath, or afterwards in exhalation, as with our patient.
Reverse triggering often occurs in heavily sedated patients, and is defined by a stable, repetitive pattern (i.e. it is not voluntary, but reflex mediated). It can also occur in anoxic brain injury. Treating it involves breaking the pattern and avoiding harmful therapies. It can even be induced in healthy patients but this is much less clinically relevant, and is rare.
DO NOT just increase the trigger sensitivity of the vent. This can stop breath stacking but does not prevent dysynchrony and it can cause harmful changes in transpulmonary pressure. For this patient, sedation was lightened slightly, and the respiratory rate decreased and the pattern of reverse triggering ultimately broke without the need for paralysis.
We are extremely excited for another PulmPEEPs Roundtable table discussion today. We have spent multiple episodes talking about different aspects of ARDS and respiratory failure. Today, multiple expert guests return, as well as a new guest to the show, to discuss the future of ARDS research. This is a can’t miss discussion that is so jam-packed with pearls you’ll have to listen twice!
Meet Our Guests
Carolyn Calfee is a Professor of Medicine and Anesthesia at the University of California, San Francisco. She is a world-renowned ARDS researcher and has authored multiple landmark studies in the field. She previously joined us for a discussion on ARDS precision medicine and phenotypes.
Ewan Goligher is an Assistant Professor at the University of Toronto and University Health Network. He has published many practice-changing papers in ARDS. These have included prospective studies and some fantastic retrospective analyses that have fundamentally shaped our interpretation of trial results. He previously came on the show discussing lung and diaphragm protection.
Sarina Sahetya is an Assistant Professor of Medicine at Johns Hopkins. She is a funded researcher in ARDS and respiratory physiology and has published multiple studies on lung protection and ARDS. She last helped us understand how to titrate PEEP in ARDS.
Matthew Semler is an Assistant Professor of Medicine and Biomedical Informatics at Vanderbilt University Medical Center, where he is also the Associate MICU Director and the co-director of the Inpatient Division of the Learning Healthcare System at Vanderbilt. Through his role as Chair of the Steering Committee for the Pragmatic Critical Care Research Group, he has helped lead more than two dozen randomized trials leading to multiple high-impact publications.
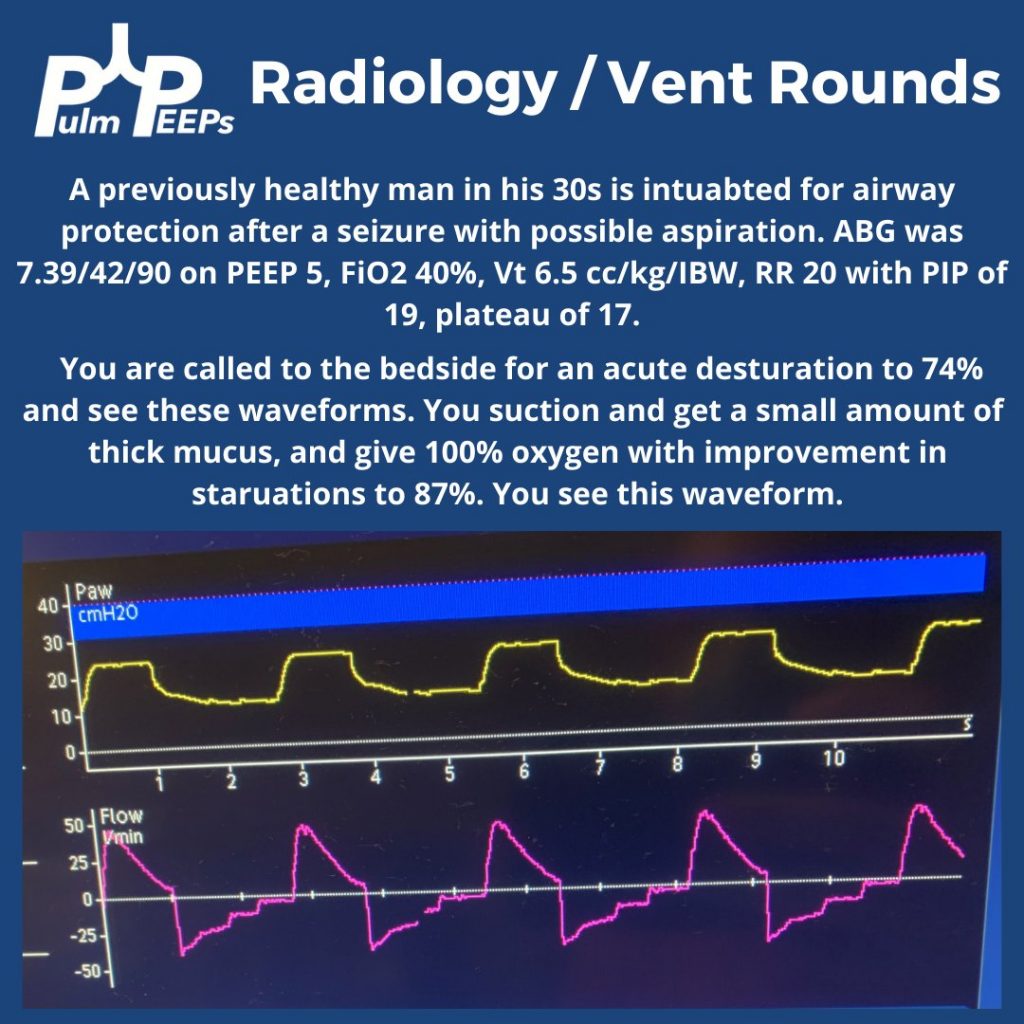
For today’s #RadiologyRounds we have a combined Radiology and Ventilator imaging rounds! You’re in the ICU caring for a young patient on a ventilator when you are called to the bedside for a desaturation.
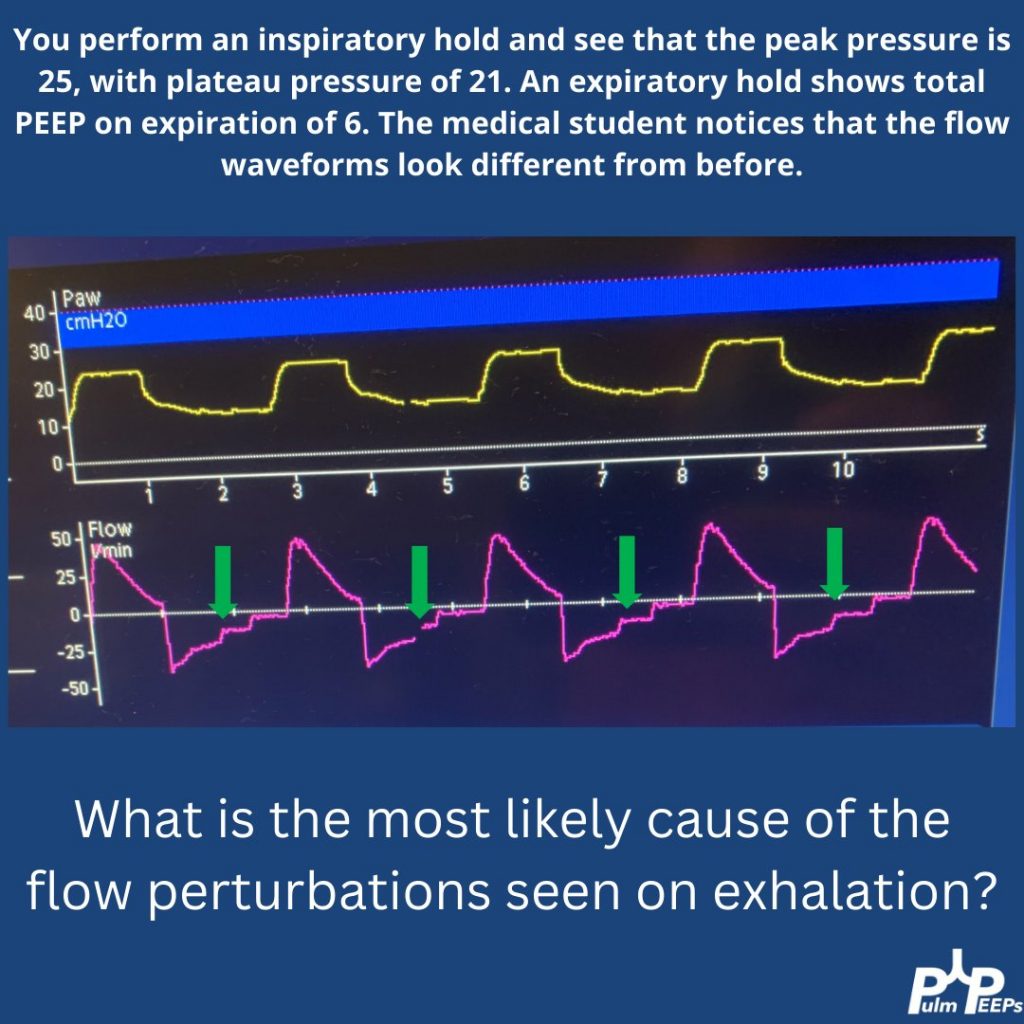
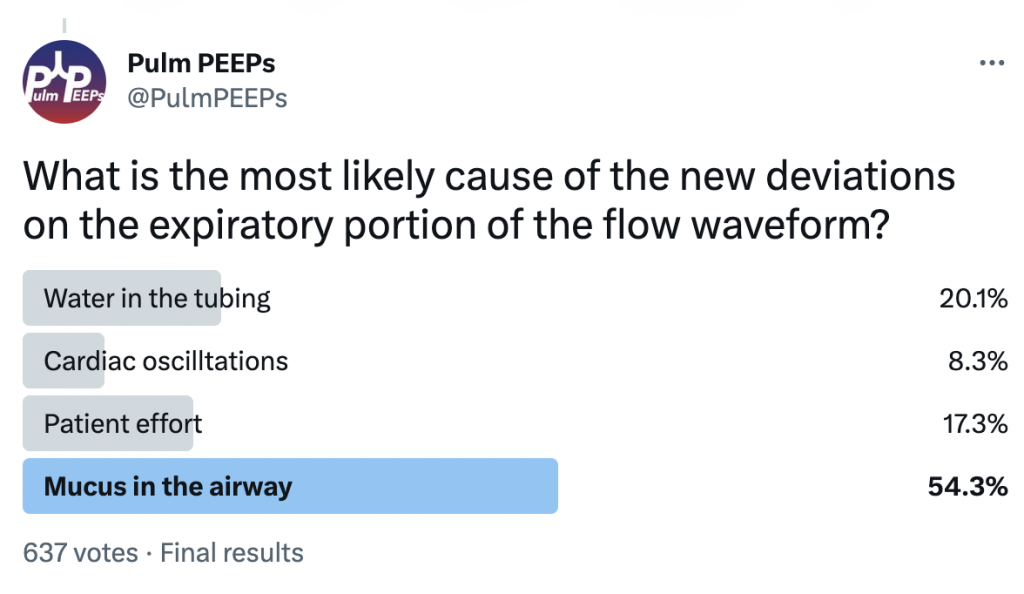
You perform an inspiratory hold and see that the PIP, plateau, and difference between peak and plateau have all increased. On exam you hear bilateral mechanical breath sounds anteriorly. You order a CXR and the student asks a question about the waveforms
There are pressure deviations corresponding to the flow deviations.
There is no clear patient effort The fact that the PIP and plat have changed makes water in the tubing or cardiac oscillations less likely.
You think this is mucus, with a plug ball-valving in a bronchus
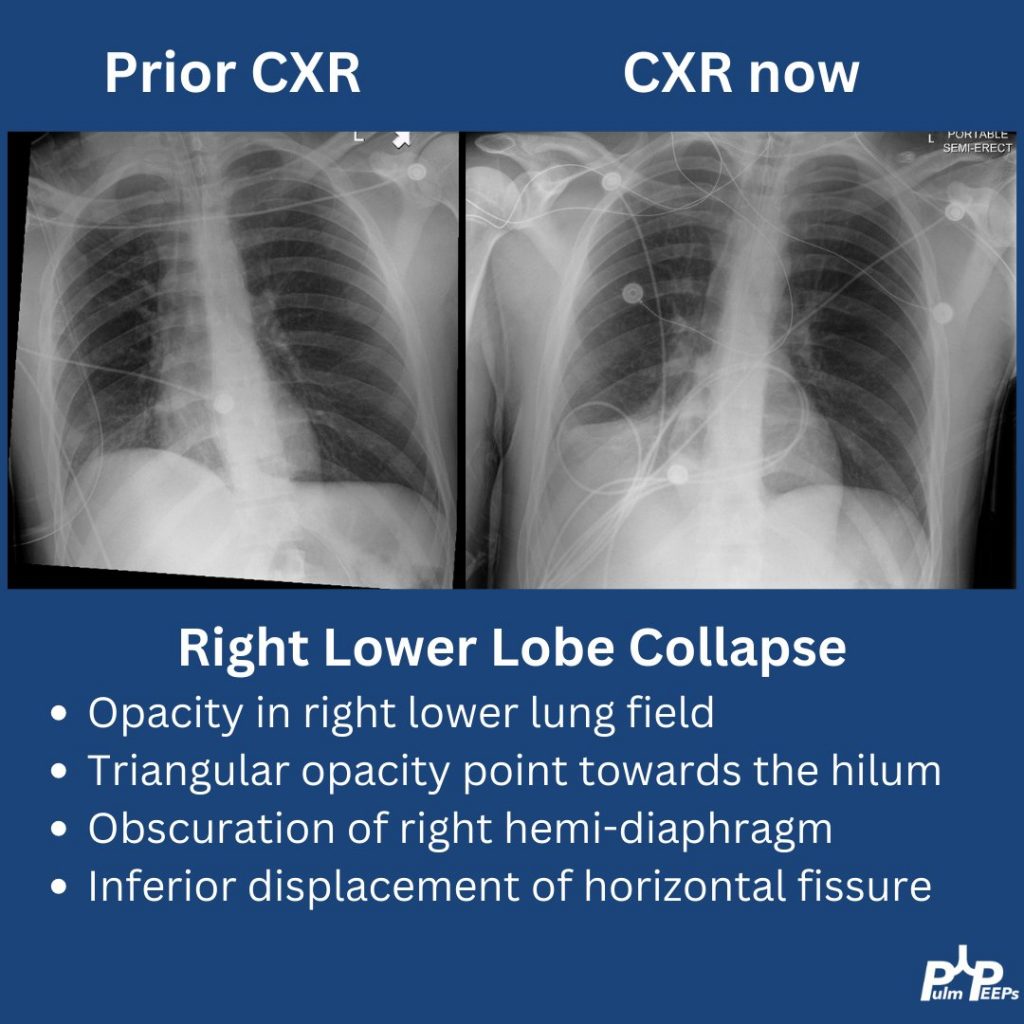
The CXR arrives and shows right lower lobe collapse.
A bedside bronchoscopy is performed with large mucus plugs suctioned out of the RLL and RML. Afterward, the patient’s oxygenation is improved, the flow deviations resolve, and the plateau pressure drops to 19