Today we’re back with another stop on our Fellows’ Case Files journey and making our way to the University of Rochester. Tune in to hear about this fascinating case and learn some key teaching points along the way.
Meet Our Guests
Dr. Shiv Patel completed his IM residency and a Chief year at the California Pacific Medical Center- Van Ness Campus and is currently a second-year PCCM fellow at the University of Rochester.
Dr. Mary Anne Morgan is an Associate Professor of Medicine and the Fellowship Program Director for the PCCM Fellowship at the University of Rochester. Her clinical interests range from the care of critically ill patients in the ICU to the diagnosis and management of rare lung disease in her role as Director of the University of Rochester LAM Clinic. She loves unwrapping clinical reasoning with trainees, exploring issues around communication and teamwork in the ICU, and is excited about curriculum revitalization in the growing URMC PCCM fellowship program.
Case Presentation
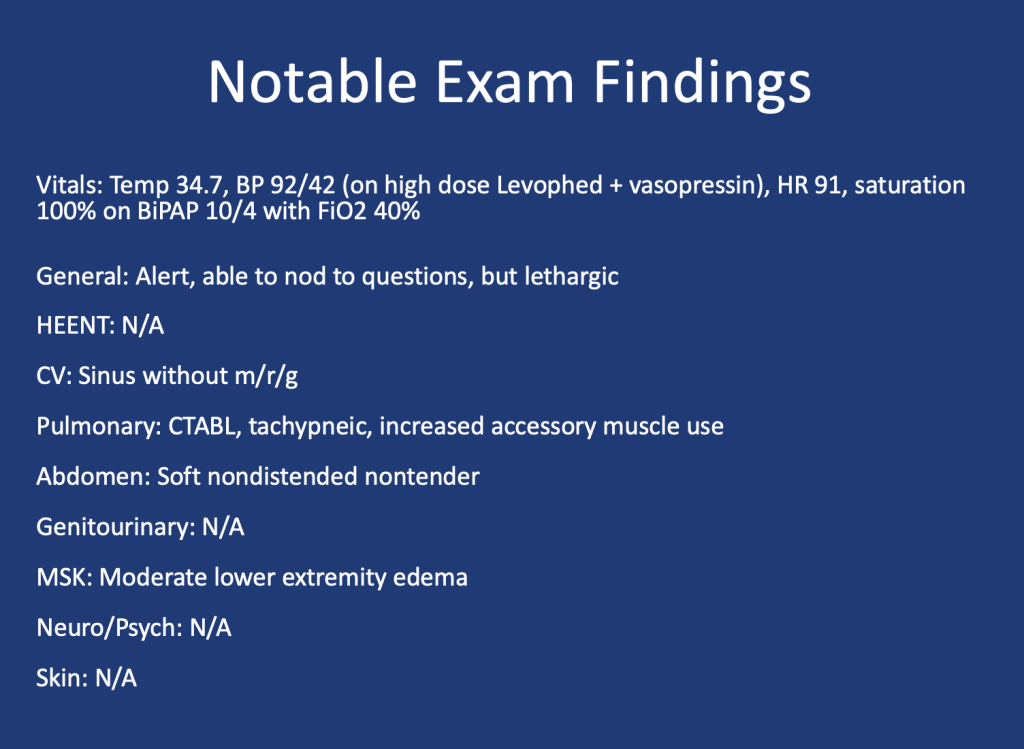
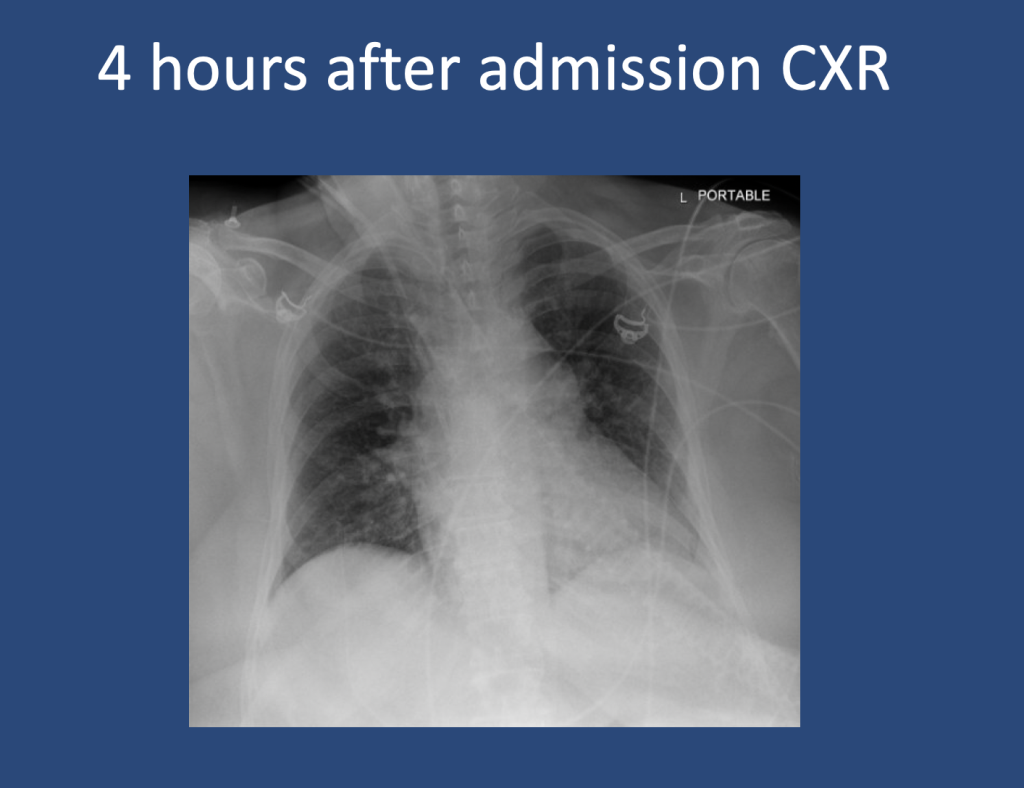
A 75 y.o. female with a history of Hypertension, Hyperlipidemia, and Type 2 Diabetes presented for evaluation of hypoglycemia and generalized fatigue. She had felt poorly for about a week with symptoms of back pain, generalized weakness, and dyspnea, all of which acutely worsened on the day of presentation.
She was found to be hypoglycemic with a blood glucose level in the to 40’s. Initial vital signs included a heart rate of 56, blood pressure of 70/40, respiratory rate of 30, and temperature of 28.5 degrees Celsius.
Key Learning Points
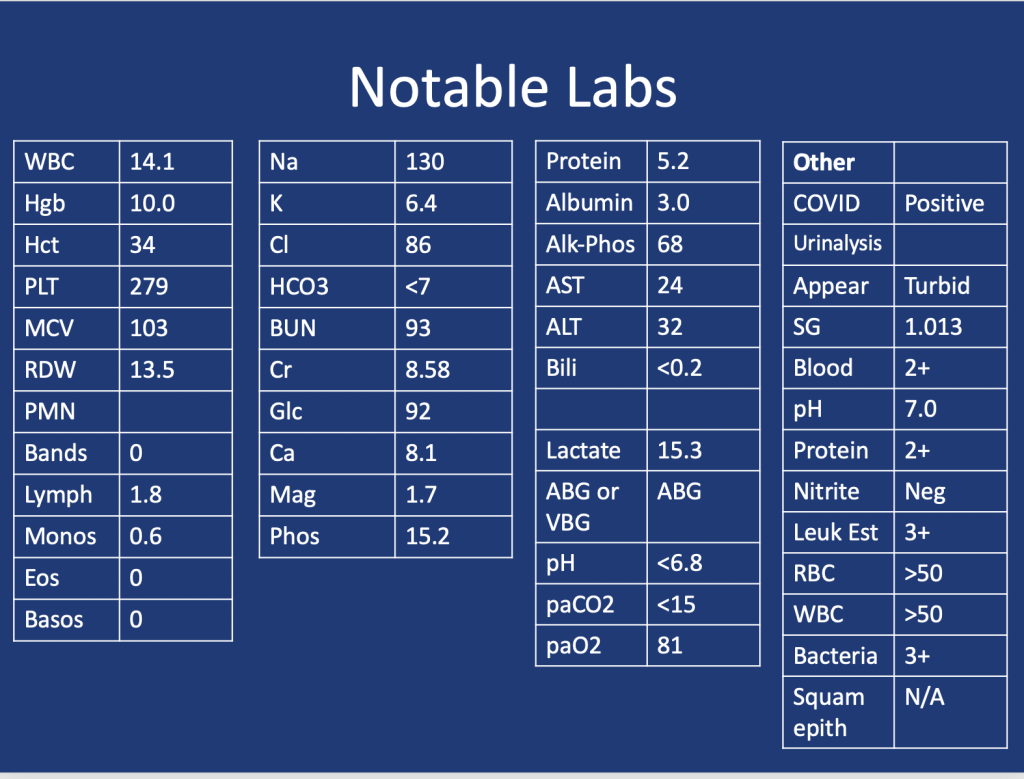
Lactic Acidosis: Type A, Type B and Type D
Type A: Typically secondary to conditions that impair oxygen delivery (respiratory failure, PE) to tissues or decrease tissue perfusion (severe anemia, shock). Patients typically present with hypotension, tachycardia, tachypnea, altered mental status, and signs of organ dysfunction.
Type B: Typically secondary to conditions that directly affect cellular metabolism or lactate clearance and characterized by the presence of hyperlactatemia without evidence of tissue hypoperfusion or hypoxia. Conditions associated include liver dysfunction (e.g., liver failure, cirrhosis), malignancies (especially hematological malignancies), medications/toxins (e.g., metformin, cyanide poisoning), inborn errors of metabolism, and mitochondrial disorders.
Type D: Less common presentation and can be seen in patients with short gut syndrome.
References
1.Blough B, Moreland A, Mora A Jr. Metformin-induced lactic acidosis with emphasis on the anion gap. Proc (Bayl Univ Med Cent). 2015 Jan;28(1):31-3. doi: 10.1080/08998280.2015.11929178. PMID: 25552792; PMCID: PMC4264704.
2.Callelo et al. Extracorporeal Treatment for Metformin Poisoning: Systematic Review and Recommendations From the Extracorporeal Treatments in Poisoning Workgroup. DOI: 10.1097/CCM.0000000000001002
3.Friesecke, S., Abel, P., Roser, M. et al. Outcome of severe lactic acidosis associated with metformin accumulation. Crit Care14, R226 (2010). https://doi.org/10.1186/cc9376
Welcome to our second episode of ATS 2024 highlighting content featured through the ATS Critical Care Assembly. Today we are going to be talking about one of the Critical Care Assembly Symposiums entitled: “Care of Dying in the ICU: End of Life Care in 2024 and Beyond”
Meet our Guests
Dr. Theodore “Jack: Iwashyna is a Bloomberg Distinguished Professor at Johns Hopkins School of Medicine and the Johns Hopkins Bloomberg School of Public Health. Jack is a critical care physician and has a broad focus on research that understands the broader context of critical illness, and the long term impact on patients’ lives. He is an enormously productive and successful researcher with numerous publications in the field of critical care, and is a pioneer in the field of ICU survivorship. He is a devoted mentor and has received accolades from numerous societies
Dr. Molly Hayes is an Associate Professor of Medicine at Beth Israel Deaconess Medical Center and Harvard Medical School, the Director of the MICU at BIDMC, and the Director of External Education at the Carl J Shapiro Institute for Education and Research. She additionally is a co-founder of the BIDMC Center for Humanizing the ICU. Molly has been extensively involved with ATS with leadership roles in the Critical Care Assembly, and the newly minted Steering Committee on the Advancement of Learning.
Meet our Collaborators
The American Thoracic Society Critical Care Assembly is the largest Assembly in the American Thoracic Society. Their members include a diverse group of intensivists and care providers for both adult and pediatric critically ill patients. The primary goal of the Critical Care Assembly is to “improve the care of the critically ill through education, research, and professional development.”
We’re super excited to have a joint episode this week with Dr. Cyrus Askin and Dr. Nick Mark from Critical Care Time! We discuss all the ways that bronchoscopy can be your best friend in the ICU and how to be prepared for the unexpected scary situations that arise in the ICU. This ranges from airway bleeds, difficult intubations, lobar collapse, and trach emergencies. Don’t miss this great discussion!
Key Learning Points
Utility of bronchoscopy in people with critical illness
Bronchoscopy can be both diagnostic and therapeutic; both are potentially lifesaving.
General situations where bronchoscopy is useful in the ICU:
Placing (or confirming placement of) an endotracheal tube or tracheostomy tube
Removing a foreign body or mucous plugs from the lungs
Localizing the source of pulmonary hemorrhage or performing interventions to stop/contain the bleed
Diagnosing certain rare conditions, particularly those where the diagnosis can substantially change management (e.g. DAH, AEP, rare infections, etc).
Proficiency with bronchoscopy is important to realize the benefits. Simply “having the equipment” is insufficient, regular practice/simulation is essential
Anesthesiologists, emergency physicians, and other specialists may have limited experience with bronchoscopy in training. Even experienced pulmonologists, who may be good at diagnostic bronchoscopy often have limited experience deploying bronchial blockers, using retrieval baskets, etc.
Remember: “People don’t rise to the occasion, they sink to the level of their training.”
If you haven’t regularly practiced with a bronchoscope, you are not going to be able to use it effectively under stress when performing high acuity low occurrence (HALO) procedures such as in emergent airways, deploying bronchial blockers, retrieving foreign bodies, etc.
Two broad situations where a bronchoscope is generally used:
Awake intubation in the anticipated difficult airway (e.g. someone with abnormal anatomy, airway tumor, etc)
Rescue method in the unanticipated difficult airway (e.g. very anterior cords, difficulty with Bougie, etc)
Nasal vs Oral approach:
Oral approach is usually used in an unanticipated difficult airway
Nasal approach: More common if performing an awake intubation. Nasal is often better tolerated however epistaxis can make a difficult airway almost impossible.
Sedation strategy:
Full topicalization: lidocaine vs cocaine (equally effective and lidocaine is normally preferred, however the vasoconstriction action of cocaine may be helpful in preventing epistaxis).
Gurgling (Nick: from personal experience lidocaine is super gross)
Remember total dose of lidocaine: < 8 mg/kg
Ketamine
Ideal because it’s dissociative and analgesic, maintains respiratory drive and (maybe) airway reflexes
Consider scopolamine patch to reduce oral secretions
Dexmedetomidine
Great adjunct
One vs two operator
Especially in unanticipated difficult airways; the second operator can use VL/DL to facilitate visualization of the vocal cords.
Second operator can also be preparing for a surgical airway.
Equipment considerations:
Preload the endotracheal tube onto the bronchoscope. Use the bronchoscope as a bougie to guide the ETT through the vocal cords.
Suction! You want two – one connected to the bronch and one connected to a yankuer.
Disposable vs “good” scope
Remember to load the tube first!
Also remember to lube the tube!
Tracheostomy troubleshooting
Similarly to intubation, bronchoscopy can be very useful to confirm placement
Mechanics are similar to above
Goal is to avoid inadvertent placement of the tracheostomy tube into the soft tissues of the neck and to avoid putting air into those tissues (false lumen).
Advanced trick for exchanging tubes: You can use a disposable bronchoscope to exchange tubes: you can get it in, confirm placement, then cut it with trauma shears! Now you can slide the old tube out and put a new one in. (Don’t try this on a $40,000 fiberoptic bronchoscope!)
Ideally you should load the ETT onto the bronchoscope in advance (red arrow). If necessary however, you can cut the ETT and turn the disposable bronchoscope into a improvised exchange catheter. This technique is very useful for exchanging tracheostomy tubes.
Foreign Body Removal from airways
Bronchoscopy is invaluable for both diagnosis and treatment of foreign body aspirations.
Most commonly these aspirations are food (nuts, seeds, etc), teeth, pills, etc
Intubated is harder in many cases: no cough to help, hard to get foreign body out of the ETT.
Flexible vs rigid
Most objects can be retrieved using flexible bronchoscope; however 15-20% require rigid bronchoscopy
Flexible can reach smaller foreign bodies that are lodged more distally.
Rigid bronchoscopy is usually done if flexible bronchoscopy fails; an interventional pulmonologist wielding a rigid is superior but more invasive (requires GA)
Cryoprobe can be especially useful for frangible materials (e.g. food)
Mucous Plugs & Lobar collapse
Presentation can be subtle or dramatic.
Bronchoscopy can remove mucous plugs and help re-expand collapsed lung areas, which is potentially life saving.
Additionally, bronchoscopy can permit diagnosis of tracheal bronchus (bronchus sui)
Pig bronchus – 1-3% of people – have a RUL bronchus that comes off the trachea.
Often presents with RUL collapse in an intubated person.
Suction considerations and bronchoscope size
Remember that suctioning force is highly dependent (i.e. radius raised to the fourth power!) upon the working channel size. Use the largest size bronchoscopy possible when suctioning.
Remember that other interventions: regular inline suctioning, chest PT, adequate hydration, mucolytics are also important to prevent recurrent mucous plugging.
Localization & Isolation of Pulmonary Hemorrhage
Pre-bronch interventions
Stabilization
Nebulized TXA
Bad side down → counter-intuitive because shifting blood flow, but also the goal is to protect the non-bleeding lung.
etc
Bronch can localize the bleeding site. Bronch can also perform interventions such as:
Cold saline
Epinephrine 1:100,000
Bronchial blockers – comparison of types
CRE balloon
Fogarty
Cryo probe – great for removing clots
Delivering ETT to contralateral side → single lung ventilation
Making “bronchoscopy only” diagnoses
Diffuse Alveolar Hemorrhage (DAH)
Finding: Increasingly bloody returns on serial lavages
1) an unexpected diagnosis was made and followed by a management change (as the most rigorous estimate of utility)
13% of the time a diagnosis was only made because of bronchoscopy which changed management
2) the post-bronchoscopy diagnosis was discordant from the leading diagnosis considered before this procedure and was followed by a management change
48% of the time pre and post procedure leading diagnoses were different
26% of the time the change in leading diagnosis led to a change in therapy
3) a change in management was made following bronchoscopy regardless of whether the diagnosis was expected or considered.
32% escalation of antibiotics
30% de-escalation of antibiotics
9% addition of steroids
2% mold → surgery
Remember that in critically ill patients whose symptoms are unexplained or failing to resolve with therapy, diagnostic flexible bronchscopy can provide useful insights.
Hi everyone, we’re here with another Fellows’ Case Files. Today, we’re going virtually to Emory University School of Medicine. We’re joined by Associated Editor Luke Hedrick to dive into a critical care case. Listen in and let us know if you have any additional thoughts or questions!
Meet Our Guests
Luke Hedrick is a first-year pulmonary and critical care fellow at Emory University. He did his internal medicine residency at BIDMC in Boston. He is also one of our amazing Associate Editors here at Pulm PEEPs
Shirine Allam is an Associate Professor of Medicine at the Emory University School of Medicine where she is the Program Director of both the Pulmonary and Critical Care Medicine fellowship as well as the Critical Care Medicine fellowship. She completed her PCCM training at the Mayo Clinic in Rochester, followed by a Sleep Medicine fellowship at Stanford. She has received multiple teaching awards throughout her career
Case Presentation
A 32-year-old male is brought in by his coworkers unresponsive. He is a construction worker and was his usual self in the morning at the start of the day, but when they broke for lunch they noticed he was acting different—his arms were drooping, and while he initially was able to answer yes/no, he soon started babbling, then grunting, then vomited and became unresponsive. They laid him flat, threw cold water on him because it was 110 degrees and humid outside that day, and brought him to the ED.
When they arrive in the ED, he is unresponsive and warm to the touch. His vitals are notable for an oral temperature of 105, HR in the 160s, BP 76/34, a RR in the high 30s, and an SpO2 100% RA. His exam is relatively unremarkable other than for significant diaphoresis and both bowel and bladder incontinence.
Key Learning Points
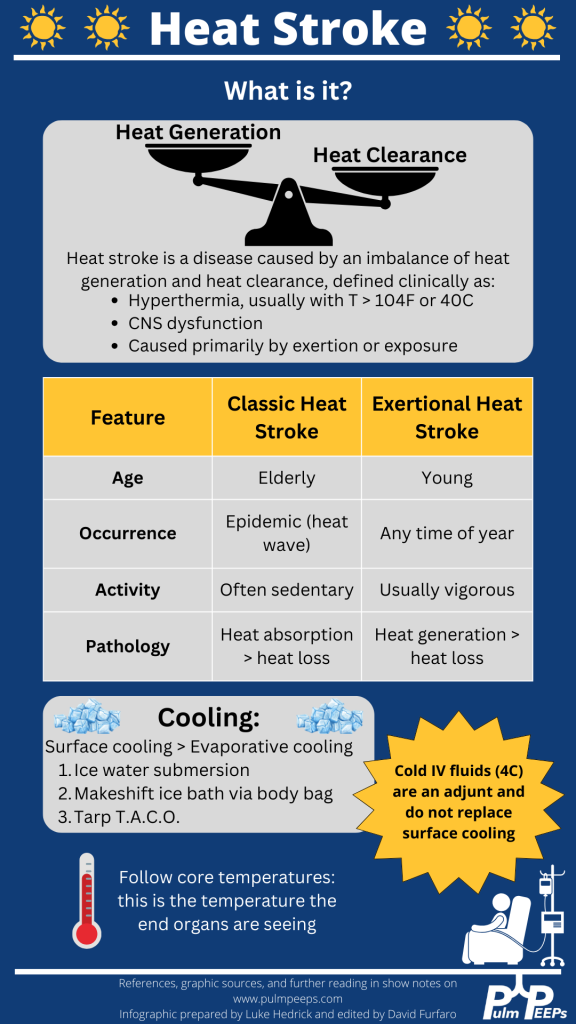
Definition and recognition of heat stroke: Heat stroke is characterized by hyperthermia (>104°F or 40°C) accompanied by CNS dysfunction, primarily caused by exertion or exposure. Encephalitis without significant heat load does not constitute heat stroke.
Management priorities: Rapid cooling is paramount to minimize long-term complications and organ failure. Cooling should be initiated as soon as possible, even before transportation to a hospital, particularly in cases of exertional heat stroke.
Cooling methods: Surface cooling, such as immersion in ice water, is the most effective way to cool heat-stroke patients. Alternative methods include the TACO method and evaporative cooling, although they are less efficient. Refrigerated IV fluids can be used as an adjunct, but they do not replace the need for surface cooling.
Monitoring and goals: Shivering during cooling should be monitored to prevent excessive heat generation. The goal is to reach a normal core body temperature (~38°C or 100.4°F). Traditional antipyretics like aspirin and acetaminophen should be avoided due to ineffectiveness and potential toxicity.
Approach to endotracheal tube (ETT) exchange: ETT exchange requires preparation for potential complications. This includes ensuring the availability of airway equipment, sedation of the patient, and having additional personnel for assistance. Direct visualization using a video laryngoscope is recommended, along with measuring and marking the exchange catheter for proper insertion depth.
The following infographic can be downloaded from our website:
We’re starting off 2024 with a bang!! Today we’re hosting another expert Roundtable discussion and we’re joined by internationally recognized experts in the field. We’ll tackle everything from teaching about sepsis, to how to incorporate guidelines into education and practice, to future research directions in the field. This is a can’t-miss discussion. Let us know what you think and other sepsis questions you have!
Meet Our Guests
Dr. Derek Angus is a Professor at the University of Pittsburgh where he holds the Mitchell P. Fink Endowed Chair in Critical Care Medicine and is the Chair of the Department of Critical Care Medicine. He is a world-renowned researcher in a range of critical care topics including sepsis, has hundreds of publications, and has led numerous NIH-funded studies.
Dr. Hallie Prescott is an Associate Professor in Pulmonary and Critical Care Medicine at the University of Michigan. She is the Co-Chair of the Surviving Sepsis Campaign Guidelines and is also an internationally recognized expert due to her research in improving sepsis outcomes. She has been recognized by both medical journals and professional societies for her outstanding contributions to the field.
Summary of Episode Discussion Topics
1. Sepsis Guidelines and Education
Surviving Sepsis Guidelines: Stressed as essential reading for professionals in pulmonary and critical care. They provide a structured approach to sepsis management.
Teaching Approaches: Transition from during-rounds teaching to focused, separate teaching sessions for trainees. Emphasizes the need to go beyond guidelines to include discussions on seminal articles, management strategies, and areas lacking robust data.
2. Clinical Skills and Decision Making in Sepsis Care
Early Recognition and Polypharmacy: Highlighted the need for timely sepsis identification and caution against excessive polypharmacy.
Mental Models in Care: Encourages building comprehensive mental models for understanding sepsis, stressing the importance of not just treating symptoms but understanding underlying causes.
3. Implementation of Sepsis Guidelines
Guideline Application in Bedside Care: Discusses the challenge of applying guidelines while considering patient-specific factors.
Fluid Resuscitation Practices: Identifies fluid resuscitation as a key area for improvement, with a shift towards more conservative approaches.
Overcoming Institutional Barriers: Addresses the fear of causing harm as a significant barrier to guideline implementation and emphasizes the need for balanced decision-making.
4. Advances in Sepsis Care and Prevention
Pre-Hospital Sepsis Management: Explores the role of early intervention in community settings and the potential of wearables for early detection.
Paramedic Role in Early Antibiotic Administration: Underlines the importance of starting antibiotics in the ambulance for suspected sepsis cases.
5. Recovery and Post-Discharge Care
Post-Discharge Initiatives: Focuses on improving handoffs from ICU to ward and from hospital to home. Highlights the importance of medication reconciliation and clear communication with primary care.
Challenges in Continuity of Care: Discusses the need for clear documentation and communication during patient transitions to ensure continuity of care.
6. Future Directions in Sepsis Treatment and Research
Phenotyping for Targeted Treatment: The potential of identifying patient subgroups through phenotyping for more effective, tailored treatments.
Adaptive Trial Designs: Advocates for large-scale adaptive platform trials that can test multiple interventions across diverse patient populations.
7. Personal Involvements and Perspectives
Experts’ Current Work: The panelists share their ongoing projects and research in sepsis care, reflecting a commitment to advancing the field through comprehensive and adaptive approaches.
This week we are excited to bring you our podcast cross-over event as we are joined by Eddie Qian and Todd Rice, the co-founders of the ICU Ed and Todd-Cast. Listen today as we discuss the recent ACORN trial evaluating the use of Cefepime versus Pipercillin-Tazobactam in adults hospitalized with acute infection.
This week on Pulm PEEPs, we are excited to be cross-posting an episode that Dave Furfaro did on the ATS Breathe Easy Podcast. Listen to hear a discussion about the best way to create a positive learning environment in the ICU, and how to effectively prepare bedside teaching for learners of all levels.
Meet The Host
Matthew Stutz hosted this episode of the ATS Breathe Easy Podcast. He is an Attending Pulmonary and Critical Care physician at Cook County Health and an Assistant Professor at Rush University. He is a dedicated educator and an active member of the American Thoracic Society.
Key Learning Points
Empowerment: It’s crucial to empower both learners and teachers in an educational setting.
Open Communication: Learners should be encouraged to express their discomfort or challenges in learning. This will allow teachers to adapt and create a more effective learning environment.
Self-awareness and Continuous Improvement: Teachers should be self-aware and continuously strive for improvement. If a teacher knows their weak points or areas they want to enhance, such as bedside teaching or teaching on rounds, they should communicate this to their team. This will make the team more observant and supportive in giving feedback.
Honesty: A genuine and honest dialogue helps in building a strong and trusting educational relationship. It’s beneficial for both the teacher and learner to be candid about their needs and challenges.
Feedback Mechanism: Constructive feedback is an essential part of growth. By informing team members of areas you’re working on, you can receive specific and helpful feedback at the end of a rotation or session.
Appreciation: It’s important to appreciate and acknowledge contributions in an educational or collaborative setting.
We are thrilled to spend time with Dr. Jessica Zitter who is an expert in critical care and palliative care medicine, author, speaker, and documentary filmmaker. We are honored to have her join the show today to discuss her work on improving end-of-life and humanistic care as well as promoting conversations about death and dying.
Meet our Guest
Dr. Jessica Zitter received her medical degree from Case Western Reserve University Medical School, and her MPH from UC Berkeley. She completed her IM residency at BWH, her pulmonary and critical care training at UCSF, and is additionally board certified in Palliative Care. She is an author of multiple essays and articles that have appeared in publications ranging from the NY Times to the Journal of the American Medical Association, has authored a book, and is a documentarian whose work is Emmy and Oscar nominated.
Dr. Zitter’s first book, Extreme Measures: Finding A Better Path to the End of Life, offers an insider’s view of intensive care in America today and its impact on how we die. Her work is featured in the Oscar and Emmy-nominated short documentary Extremis, available to view on Netflix. She has also produced and directed the award-winning, 2020 short documentary Caregiver: A Love Story. Dr. Zitter is currently working on her third film, The Chaplain of Oakland, which explores the devastating problem of racial healthcare inequities at the end of life. She has also founded the production and education non-profit, Reel Medicine Media.
We are extremely excited to be hosting this episode in collaboration with CardioNerds! We have known Amit and Dan for many years, and they have been huge supporters of Pulm PEEPs, so it is an honor to address a topic we’re all interested in together.
We are joined by experts in the field today to discuss acute, decompensated right ventricle failure in patients with Pulmonary Arterial Hypertension (PAH). This topic can be quite intimidating, so we hope this will serve as a valuable guide for anyone who encounters a patient like this in the ICU.
Meet Our Guests
Leonid “Leon” Mirson is an internal medicine resident at the Johns Hopkins Hospital Osler Medical Residency and an Associate Editor here at Pulm PEEPs. He was born in Ukraine and moved to Philadelphia in early childhood with his family. He received his undergraduate degree from the University of Pittsburgh where he studied biomedical engineering and received his medical degree from the University of Pittsburgh School of Medicine. His current interests include pulmonary and critical care medicine with a focus on pulmonary hypertension as well as medical education. He is a rising PCCM fellow at the University of Pennsylvania.
Bhavya Varma completed her medical school at the University of Pittsburgh, her internal medicine residency at Johns Hopkins, and is a rising Cardiology fellow at NYU. She is interested in medical education and has done work with CardioNerds during her residency.
Mardi Gomberg-Maitland is a Professor of Medicine at George Washington University. She serves as the Medical Director of the Pulmonary Hypertension Program at George Washington Hospital. She completed her medical degree at Albert Einstein College of Medicine, completed her residency at the Weill-Cornell Medical Center, and completed her fellowship in cardiovascular diseases at Mount Sinai Medical Center. Her research focus is on understanding the epidemiology of pulmonary hypertension and the development of novel therapeutics and biomarkers. Dr. Gomberg-Maitland is internationally known for her work, she has had extensive grant funding and has published over 150 articles, abstracts, reviews, and chapters.
Rachel Damico is a pulmonologist and an Associate Professor of Medicine at Johns Hopkins Hospital, where she is also the Associate Director of the physician-scientist training program. Dr. Damico received her medical degree and doctoral degree in Molecular and Cellular biology from the University of Pennsylvania. She completed her residency in the Osler Internal Medicine training program and continued on as a PCCM fellow at Johns Hopkins. She has quickly achieved an international reputation in the field of pulmonary vascular biology and both basic and translational research, as well as clinical excellence, in Pulmonary Arterial Hypertension.
Patient Presentation
A 21-year-old woman with a past medical history notable for congenital heart disease (primum ASD and sinus venosus with multiple surgeries) complicated by severe PAH on home oxygen, sildenafil, ambrisentan, and subcutaneous treprostinil is presenting with palpitations, chest pain, and syncope. She presented as a transfer from an outside ED where she arrived in an unknown tachyarrhythmia and had undergone DCCV due to tachycardia into the 200s and hypotension. On arrival at our hospital, she denied SOB but did endorse nausea, leg swelling, and poor medication adherence. Her initial vitals were notable for a BP of 80/50, HR 110, RR 25, and saturating 91% on 5L O2. On exam, she was uncomfortable appearing but mentating well. She had cool extremities with 1-2+ LE edema. Her JVP was 15cm H2O. She has an RV Heave and 2/6 systolic murmur. Her lungs were clear bilaterally. Her labs were notable for Cr 2.0, an anion gap metabolic acidosis (HCO3 = 11), elevated lactate (4.1), elevated troponin to 14, and a pro-BNP of ~5000. Her CBC was unremarkable. Her EKG demonstrated 2:1 atrial flutter at a rate of 130.
Key Learning Points
Diagnosing RV failure in patients with PH:
RV dysfunction and RV failure are two separate entities. RV dysfunction can be measured on echocardiography, but RV failure can be thought of as a clinical syndrome where there is evidence of RV dysfunction and elevated right sided filling pressures.
RV failure is a spectrum and can present with a range of manifestations from evidence of R sided volume overload and markers of organ dysfunction, all the way to frank cardiogenic shock. Most patients with RV failure are not in overt shock.
One of the first signs of impending shock in patients with RV failure is the development of new or worsening hypoxemia. Patients with decompensated RV failure approaching shock often do not present with symptoms classic for LV low flow state. Instead, hypoxia 2/2 VQ mismatching may be the first sign and they can be otherwise well appearing. Particularly because patients with PH tend to be younger, they can often appear compensated until they rapidly decompensate.
Causes of decompensation for patients with RV dysfunction and PH:
Iatrogenesis (inadvertent cessation of pulmonary vasodilators by providers, surgery if providers are not familiar with risks of anesthesia), non-adherence to pulmonary vasodilators (either due to affordability issues or other reasons), infections, arrhythmias (particularly atrial arrhythmias), and progression of underlying disease.
Patients with atrial arrhythmias (atrial flutter or atrial fibrillation) and pulmonary hypertension do not tolerate the loss of the atrial kick well as it contributes a significant amount to their RV filling and impacts their cardiac output. It is often difficult to determine if the atrial arrhythmia is a cause or effect of decompensated RV failure, but its presence is associated with a worse prognosis. Efforts should be made to re-establish normal sinus rhythm in patients with decompensated RV failure and atrial arrhythmias.
A patient’s home PH medications should never be stopped for any reason upon admission unless on the basis of recommendations by a pulmonary hypertension provider as this is often a cause of decompensation inpatient
Interpreting findings on echocardiogram:
Echo is a useful screening tool. When interpreting evidence of RV dysfunction, it is important to look at the global picture and not just one measurement.
RVSP, though commonly reported, may be of limited value when evaluating for decompensation. It’s a function of blood pressure, heart rate, and cardiac output. RVSP may even decline as shock worsens.
TAPSE is useful as a marker of RV dysfunction if it is reduced, but it is difficult to follow over time and only gives information about cardiac function around the annulus; it may be normal even when apical RV function is depressed. RV fractional area of change may be more useful for global RV function. It is important to pay attention to the RV size overall, the degree of TR, and the presence of effusion all of which are associated with RV dysfunction.
Tips regarding the interpretation of invasive hemodynamics:
Cardiac output by thermodilution is the standard way to calculate PVR. Despite the degree of TR that is typically present, it is thought to be a better representation of cardiac output than the estimated Fick calculation.
Our experts agree that routine monitoring of invasive hemodynamics for acute decompensated RV failure is likely not helpful and has significant risks. A good external volume exam or CVP off a central venous catheter + central venous saturation will likely be all you need to navigate a patient with shock secondary to RV failure. A right heart catheterization (should be only done under fluoroscopy for patients with large RVs) may be helpful if the etiology of shock is unclear.
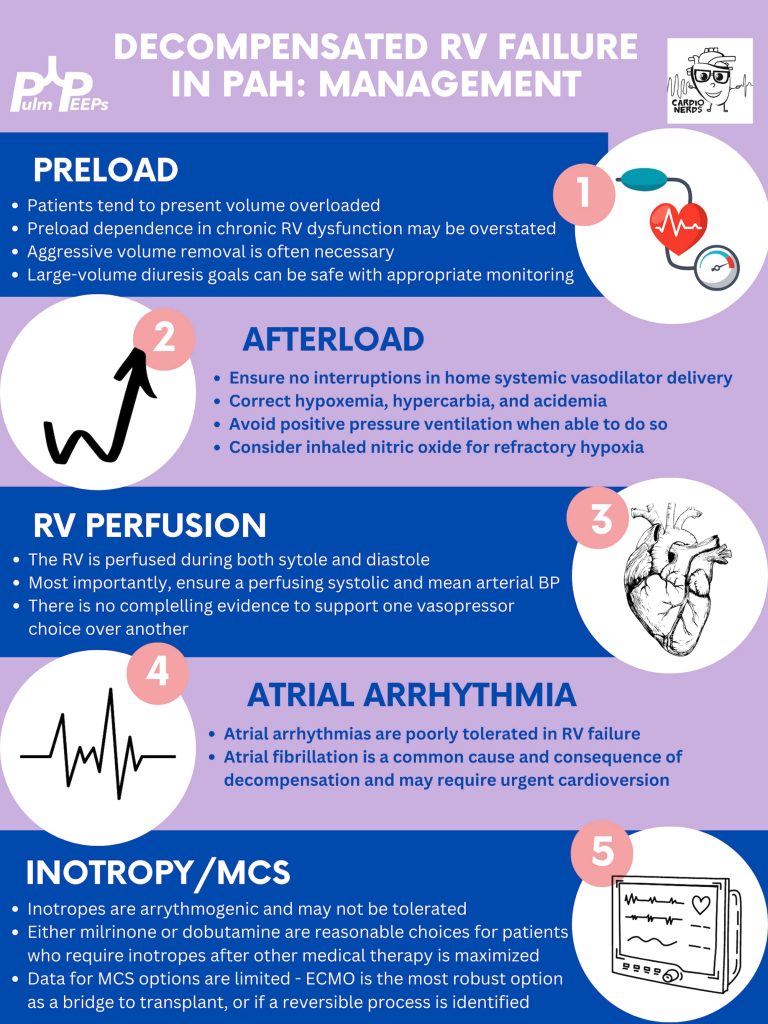
Management of decompensated RV failure in patients with pulmonary hypertension
Managing preload is of utmost importance, perhaps the most important tenant of management of decompensated RV failure. The overwhelming majority of patients with PH and decompensation are volume overloaded, it is exceptionally rare that someone would be dry. Furthermore, the myth that the RV is “preload responsive” is only true in the setting of acute RV injury (eg. RV infarction) and not so in patients with acute on chronic RV dysfunction. It is important to optimize preload in someone in decompensated RV failure and it is safe to do this more rapidly than traditionally taught. Exact goals varied between our experts, but anywhere from 2-4L net negative per day is reasonable especially if the patient is hemodynamically tolerating the fluid removal. If the patient is not responding to diuretics, hemodialysis with ultrafiltration may be necessary to optimize the patient.
Afterload is the next tenant of management. Optimizing the following parameters will reduce the patient’s pulmonary vascular resistance and reduce afterload to the right ventricle.
— Avoiding hypoxic pulmonary vasoconstriction, liberalize the patient’s O2 goal
— Avoid permissive hypercapnia and academia in this patient population
— Do not withhold a patient’s pulmonary vasodilator until discussion with the PH team. If stopped inadvertently, restart this medication immediately. For patients with malfunctioning pumps, there is a phone number on the back that you can call for rapid troubleshooting. Sildanefil can be given IV if a patient is NPO.
— Inhaled nitric oxide can improve oxygenation and reduce afterload
— Intubation and mechanical ventilation greatly increase PVR and are poorly tolerated. Exacting care must be taken to titrate PEEP and tidal volume, and avoid intubation when possible.
— Starting a new systemic pulmonary vasodilator in decompensated RV failure may be considered under close guidance from the pulmonary hypertension team
Management of atrial arrhythmias:
As above, patients with severe pulmonary hypertension do not tolerate loss of sinus rhythm well. If they are decompensated, every effort should be made to re-establish normal sinus rhythm.
Management of RV perfusion:
Unlike the LV, the RV is perfused during BOTH systole and diastole. Maintaining effective coronary perfusion to the RV is essential in RV failure. For this reason, the systemic systolic pressure (as well as the mean arterial pressure) should be kept high enough to ensure that the RV is able to perfuse. There is no great body of evidence as to which pressor works best. Norepinephrine, vasopressin, and even phenylephrine are all reasonable choices to maintain appropriate perfusing blood pressure.
Inotropy:
Patients in shock and RV failure do not always require inotropes, but if they do it’s often a sign of a grim prognosis. Either dobutamine or milrinone is reasonable, but the negative effects of these drugs (arrhythmias, tachycardia, and systemic hypotension) may limit their uses.
Mechanical circulatory support:
Limited options are available. Balloon pumps and Impella devices have limited roles except in expert centers, and ECMO remains the standard of care. ECMO (either V-V or V-A) may have utility as a bridge to recovery if a reversible cause is identified, or a bridge to transplant if the patient is on the transplant list.
Goals of care:
The prognosis of a patient admitted to the ICU with acute on chronic decompensated RV failure is guarded, with very high mortality rates even if not in shock
It is important for the patient’s longitudinal pulmonary hypertension provider to discuss the prognosis and goals of care ahead of time but this is not always possible. If they are admitted, early discussions regarding code status and prognosis are essential. It may be helpful to bring in the patient’s longitudinal pulmonary hypertension doctor into these discussions if possible.