This week the Pulm PEEPs, David Furfaro and Kristina Montemayor, are joined by three outstanding critical care doctors and medical educators to discuss the evaluation of patients with undifferentiated shock. We cover everything from the basics about defining shock, to advanced POCUS techniques to clarify the etiology of shock. Listen today and let us know your favorite technique for evaluating shock in the ICU.
Meet Our Guests
Molly Hayes is an Assistant Professor of Medicine at Beth Israel Deaconess Medical Center and Harvard Medical School, the Director of the MICU at BIDMC, and the Director of External Education at the Carl J Shapiro Institute for Education and Research. She is also a course director for a yearly CME course on principles of critical care medicine run by BIDMC and HMS.
Nick Mark is a Pulmonologist and Intensivist at Swedish Medical Center in Seattle, Washington. He is also the founder of ICU One Pager, which produces high yield critical care education one-page guides that have been downloaded by thousands of learners.
Matt Siuba is an Assistant Professor of Medicine and intensivist at the Cleveland Clinic, where he is the associate program director for the Critical Care Medicine fellowship. He founded and runs the website Zentensivist.com, has his own associated podcast, and is a senior editor at CriticalCareNow.com.
Key Learning Points
Key graphics
Definition of shock
– Shock is defined as inadequate oxygen delivery to meet the body’s needs. Decreased perfusion and oxygen delivery leads to cell injury and death
– If you define just as hypotension, you will miss people who have cryptic shock, and categorize some people with shock who don’t have it
– Cryptic shock = a patient with normal blood pressure (MAP > 65), but who still has shock based on inadequate O2 delivery
– O2 delivery is broken down in to cardiac output and arterial oxygen content
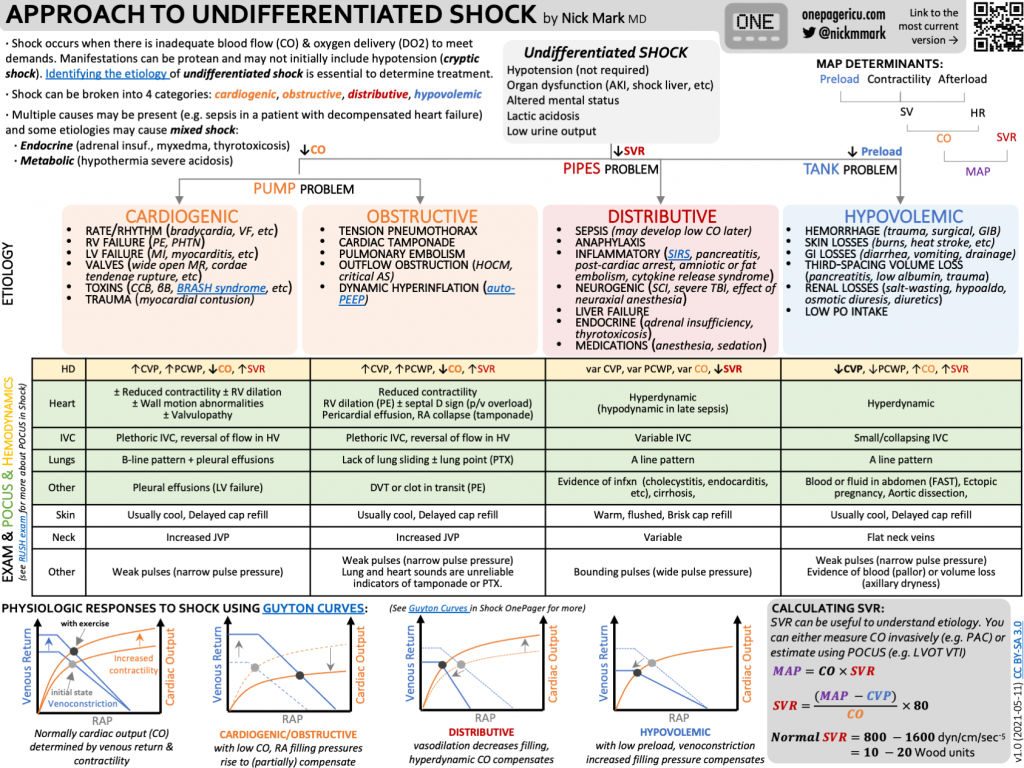
Causes of shock
Shock can be divided into three large categories:
1) A pump problem – low cardiac output. This includes cardiogenic and obstructive shock. Make sure to remember to look for tamponade and valvulopathies.
2) A pipe problem – low systemic vascular resistance. This includes distributive shock. Distributive shock is most often due to sepsis but can be due to anaphylaxis, endocrinopathies, cirrhosis, or spinal shock.
3) A tank problem – low preload. This includes hypovolemic and hemorrhagic shock. Make sure to remember about high intrathoracic pressure, which can decrease effective preload.
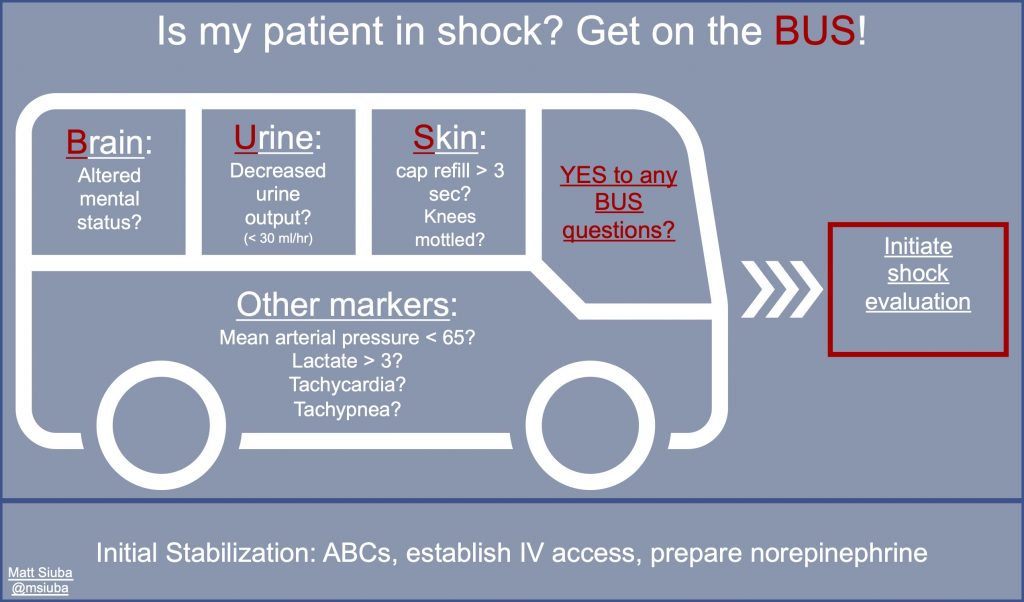
Examining a patient with undifferentiated shock
– See if the patient is on the “Shock BUS” by examining their brain (mental status), urine output, and skin
– Feel if their skin is warm vs cold and if it is mottled
– Feel the patient’s pulses to see if they are bounding, normal, or thready
Point of Care Ultrasound
– “Ultrasound is the new stethoscope”
– The first step is to always look at the heart and look for chamber size and function. You can then look for pericardial effusion
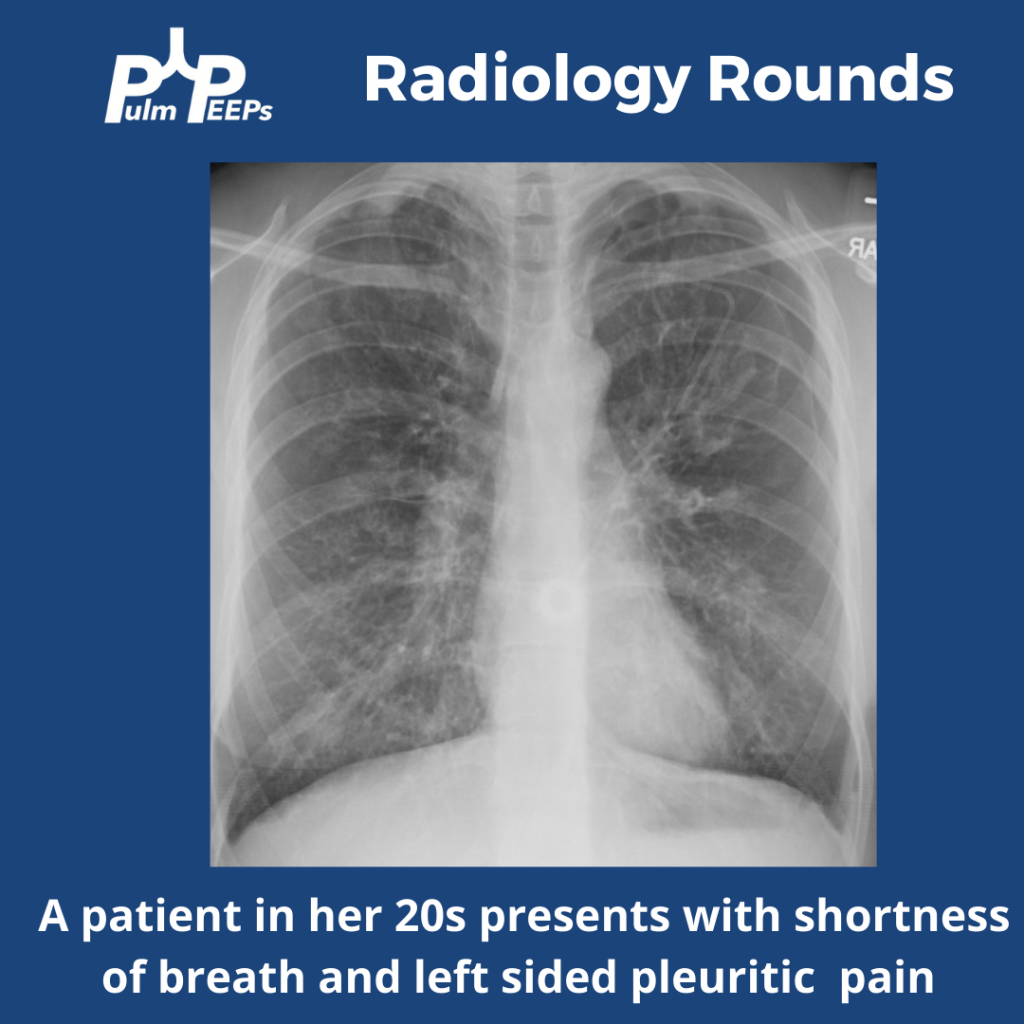
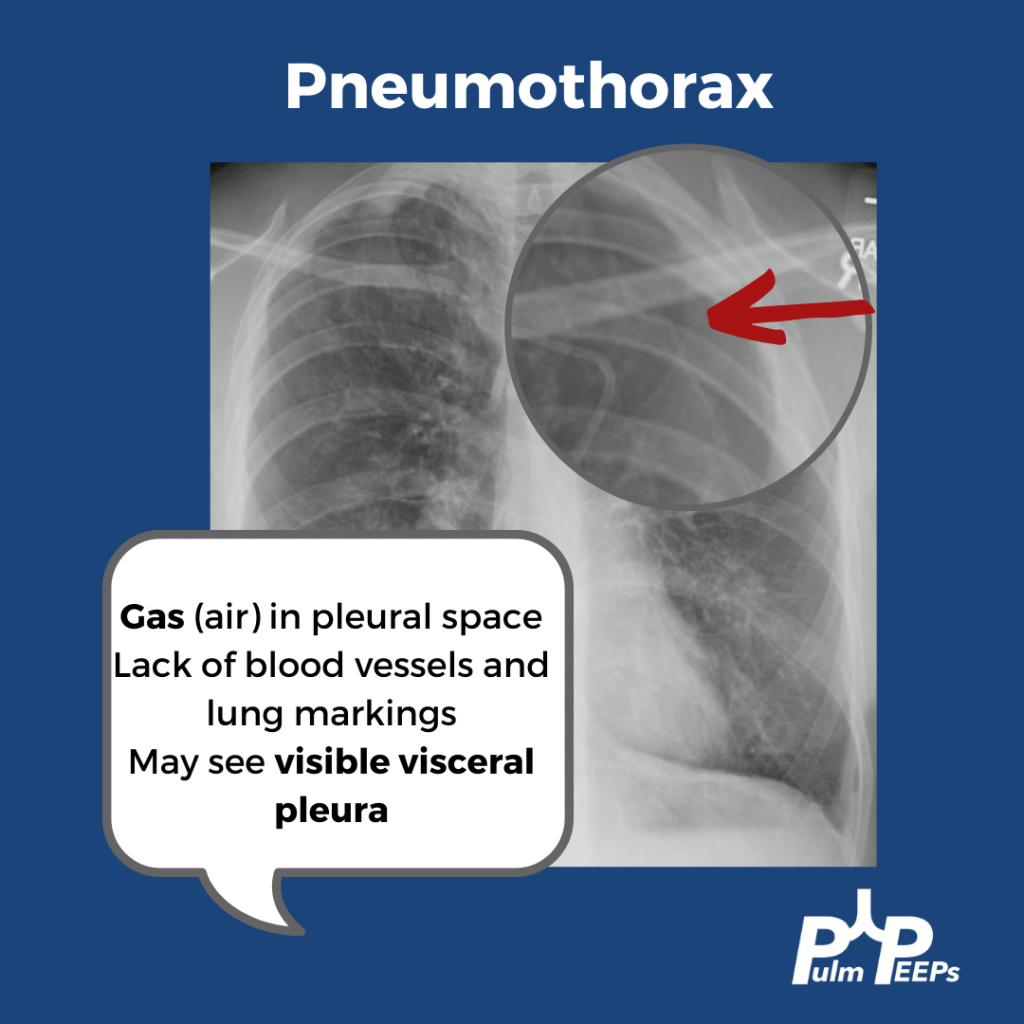
– Point of care ultrasound then includes looking at the lungs for signs of fluid overload, consolidation, or pneumothorax
– A complete ultrasound also involves looking at the abdomen and at the extremities for DVT
– More specific ultrasound techniques include looking at:
1) IVC exam to estimate right atrial pressure. This test is often misused. It is most helpful in states when the patient has low stroke volume and trying to figure out if they have cardiac limitation to stroke volume vs if they are hypovolemic.
2) Velocity time index as a measure of cardiac output to trend with interventions
References and links for further reading
- Vincent JL, De Backer D. Circulatory shock. N Engl J Med. 2013;369(18):1726-1734. doi:10.1056/NEJMra1208943
- Seymour CW, Liu VX, Iwashyna TJ, et al. Assessment of Clinical Criteria for Sepsis: For the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA. 2016;315(8):762-774. doi:10.1001/jama.2016.0288
- Chukwulebe SB, Gaieski DF, Bhardwaj A, Mulugeta-Gordon L, Shofer FS, Dean AJ. Early hemodynamic assessment using NICOM in patients at risk of developing Sepsis immediately after emergency department triage. Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine. 2021;29(1):23. doi:10.1186/s13049-021-00833-1
- Hernández G, Ospina-Tascón GA, Damiani LP, et al. Effect of a Resuscitation Strategy Targeting Peripheral Perfusion Status vs Serum Lactate Levels on 28-Day Mortality Among Patients With Septic Shock: The ANDROMEDA-SHOCK Randomized Clinical Trial. JAMA. 2019;321(7):654-664. doi:10.1001/jama.2019.0071
- Wang J, Zhou D, Gao Y, Wu Z, Wang X, Lv C. Effect of VTILVOT variation rate on the assessment of fluid responsiveness in septic shock patients. Medicine (Baltimore). 2020;99(47):e22702. doi:10.1097/MD.0000000000022702
- Sweeney DA, Wiley BM. Integrated Multiorgan Bedside Ultrasound for the Diagnosis and Management of Sepsis and Septic Shock. Semin Respir Crit Care Med. 2021;42(5):641-649. doi:10.1055/s-0041-1733896
- Yuan S, He H, Long Y. Interpretation of venous-to-arterial carbon dioxide difference in the resuscitation of septic shock patients. J Thorac Dis. 2019;11(Suppl 11):S1538-S1543. doi:10.21037/jtd.2019.02.79
- Volpicelli G, Lamorte A, Tullio M, et al. Point-of-care multiorgan ultrasonography for the evaluation of undifferentiated hypotension in the emergency department. Intensive Care Med. 2013;39(7):1290-1298. doi:10.1007/s00134-013-2919-7
- Perera P, Mailhot T, Riley D, Mandavia D. The RUSH exam: Rapid Ultrasound in SHock in the evaluation of the critically lll. Emerg Med Clin North Am. 2010;28(1):29-56, vii. doi:10.1016/j.emc.2009.09.010
Podcast: Play in new window | Download
Subscribe: Apple Podcasts | Spotify | Amazon Music | Android | iHeartRadio | Podcast Index |