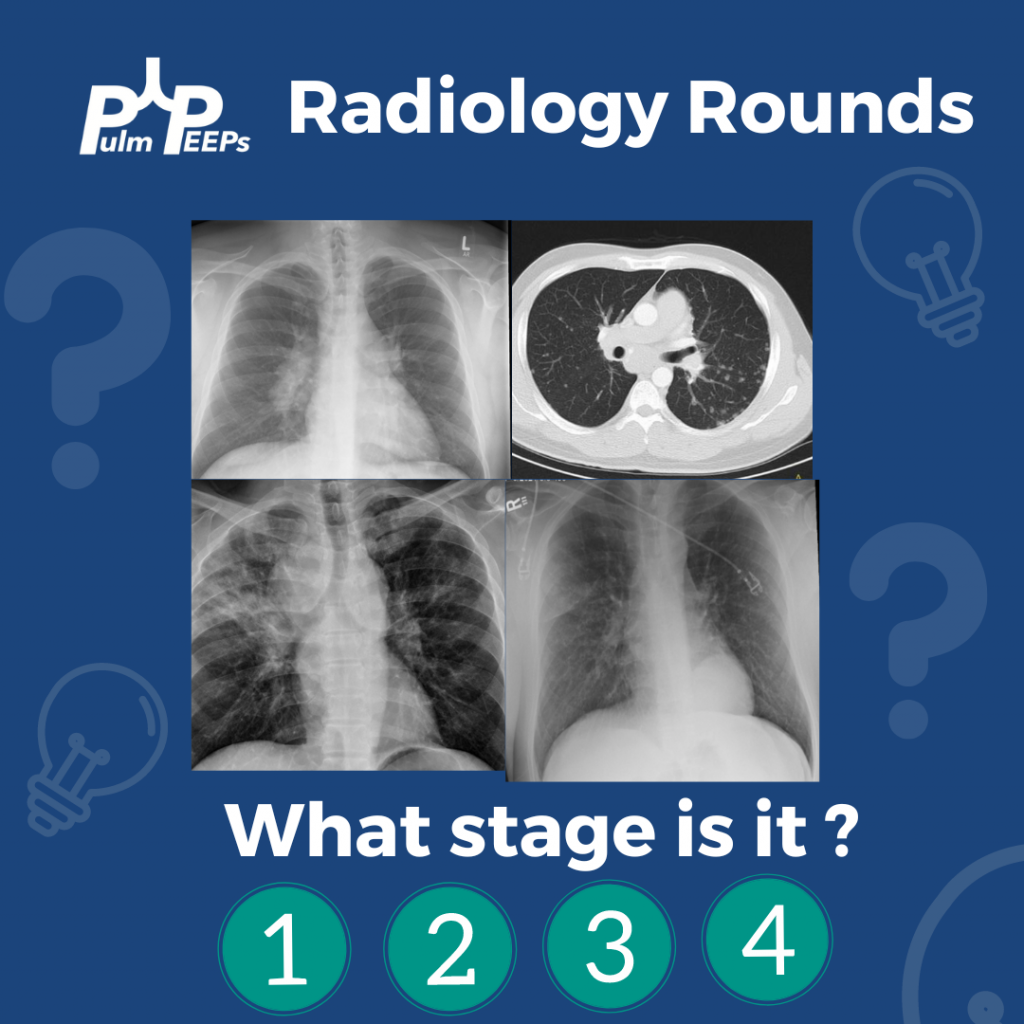
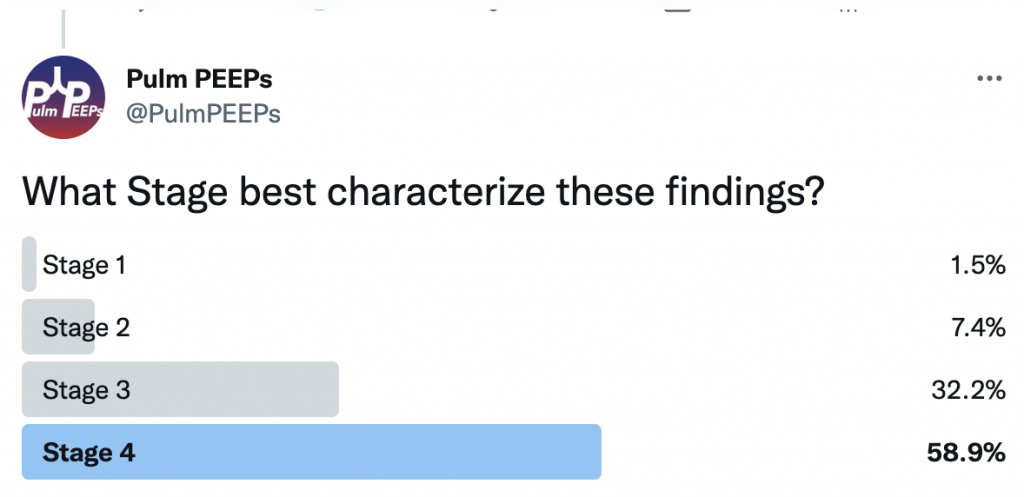
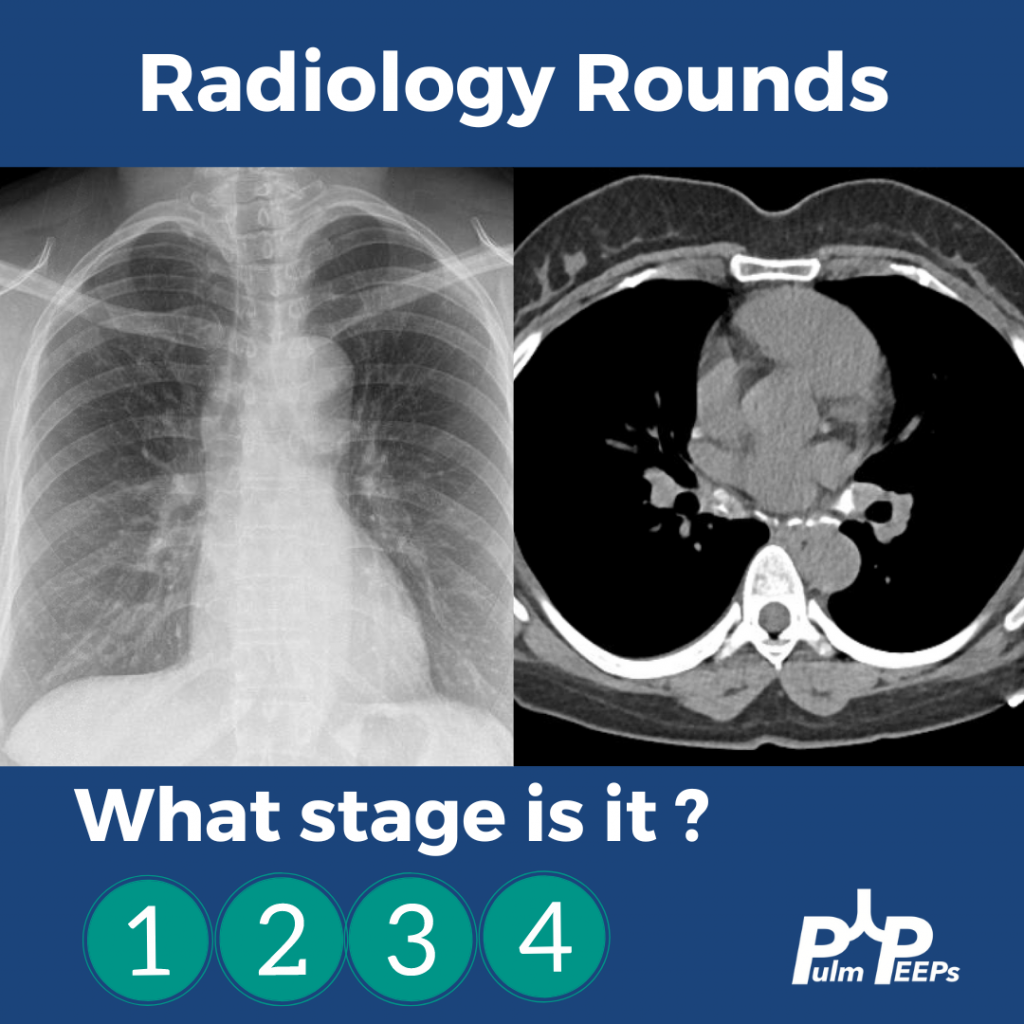
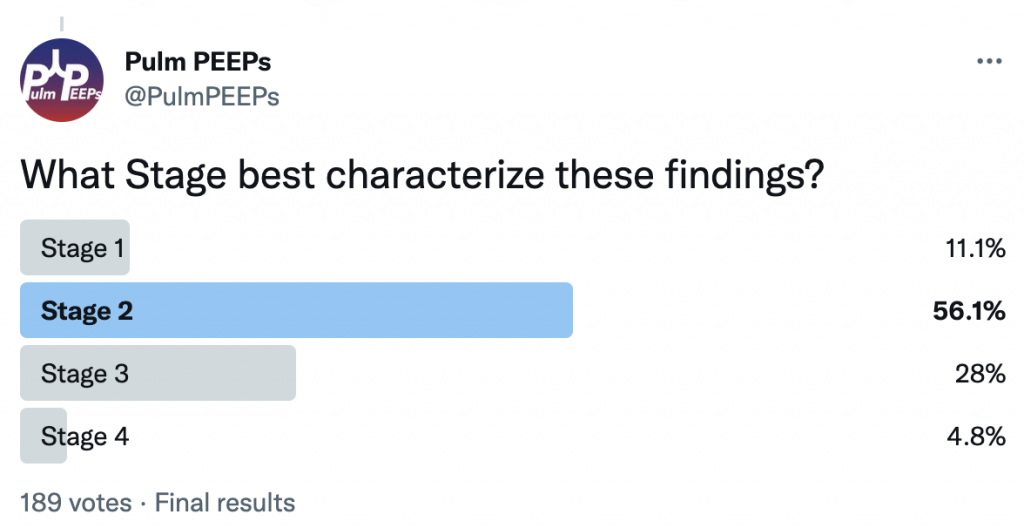
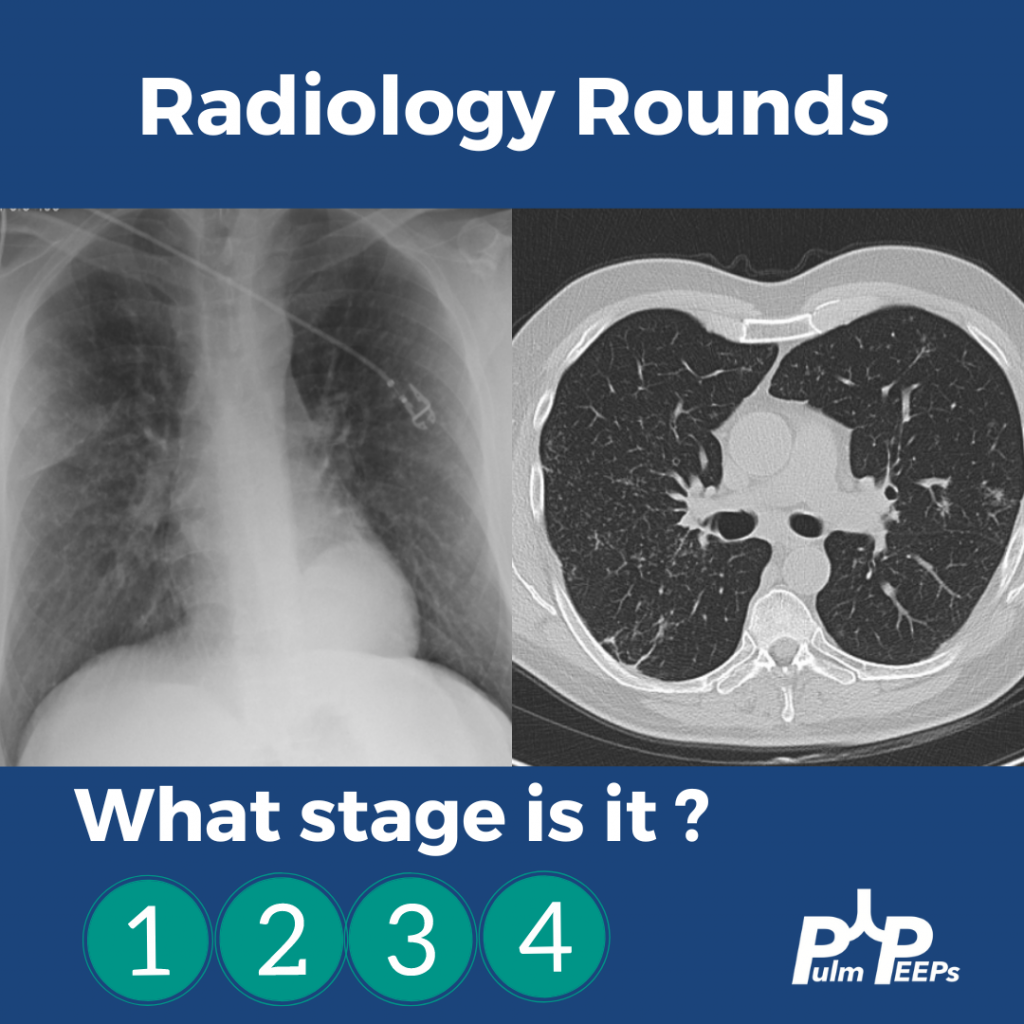
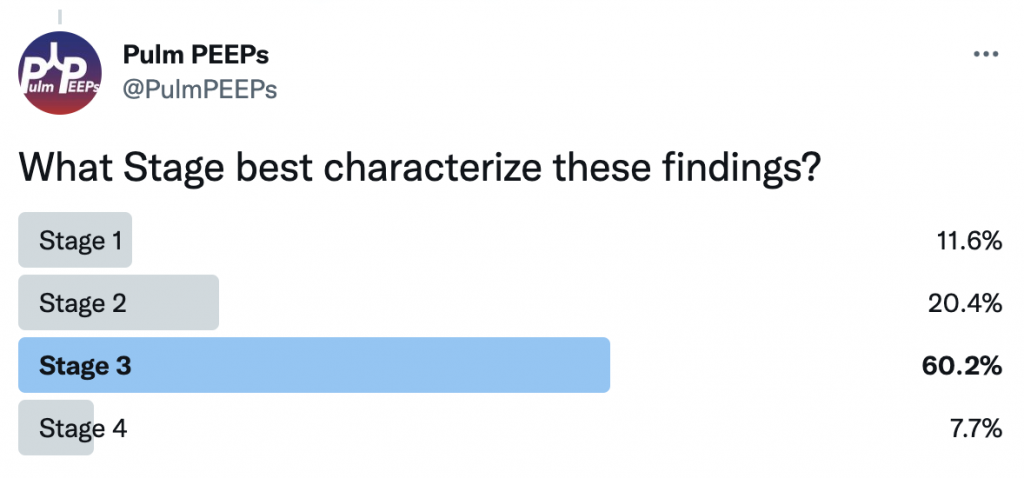
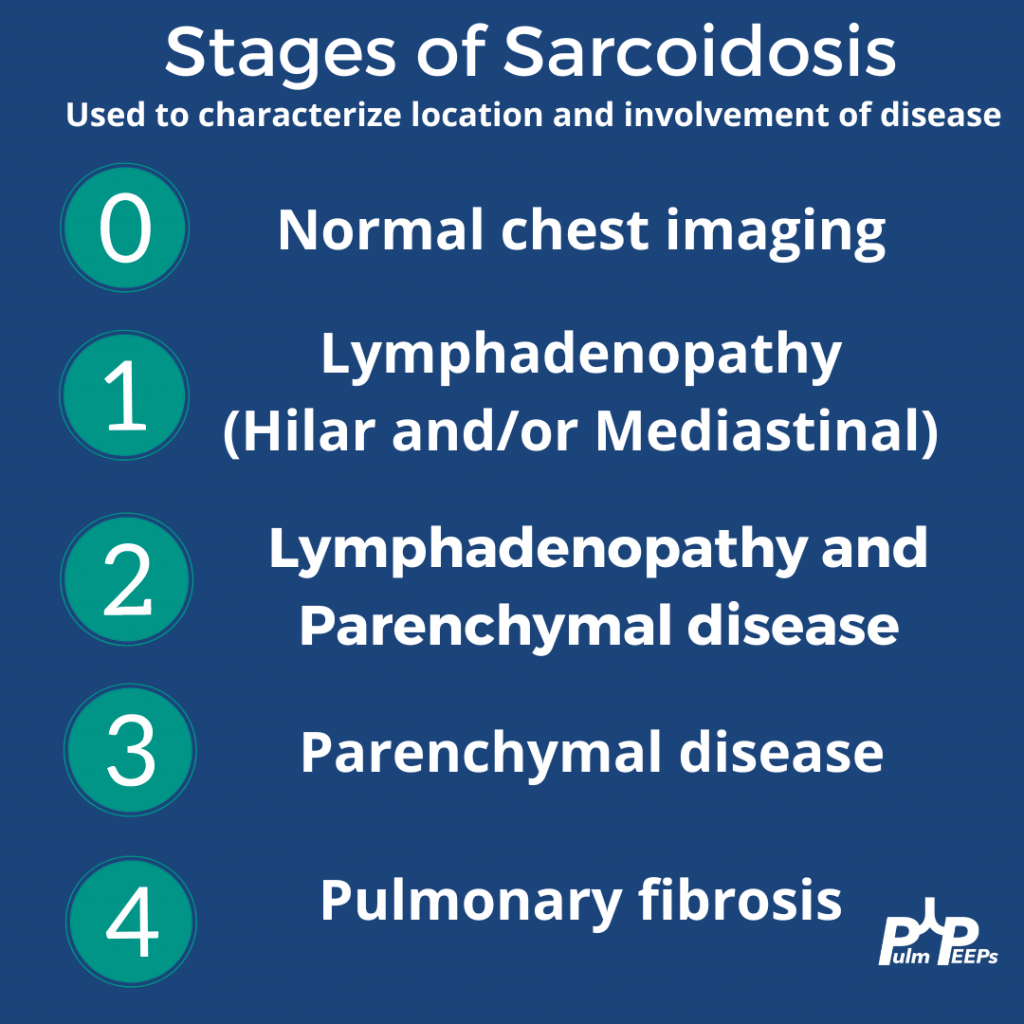
It is Tuesday and we have another Radiology Rounds we can’t wait to share with you. Follow along and see if you select the right answer as we go through different presentations of sarcoidosis and pick your answer! What stage is it?!
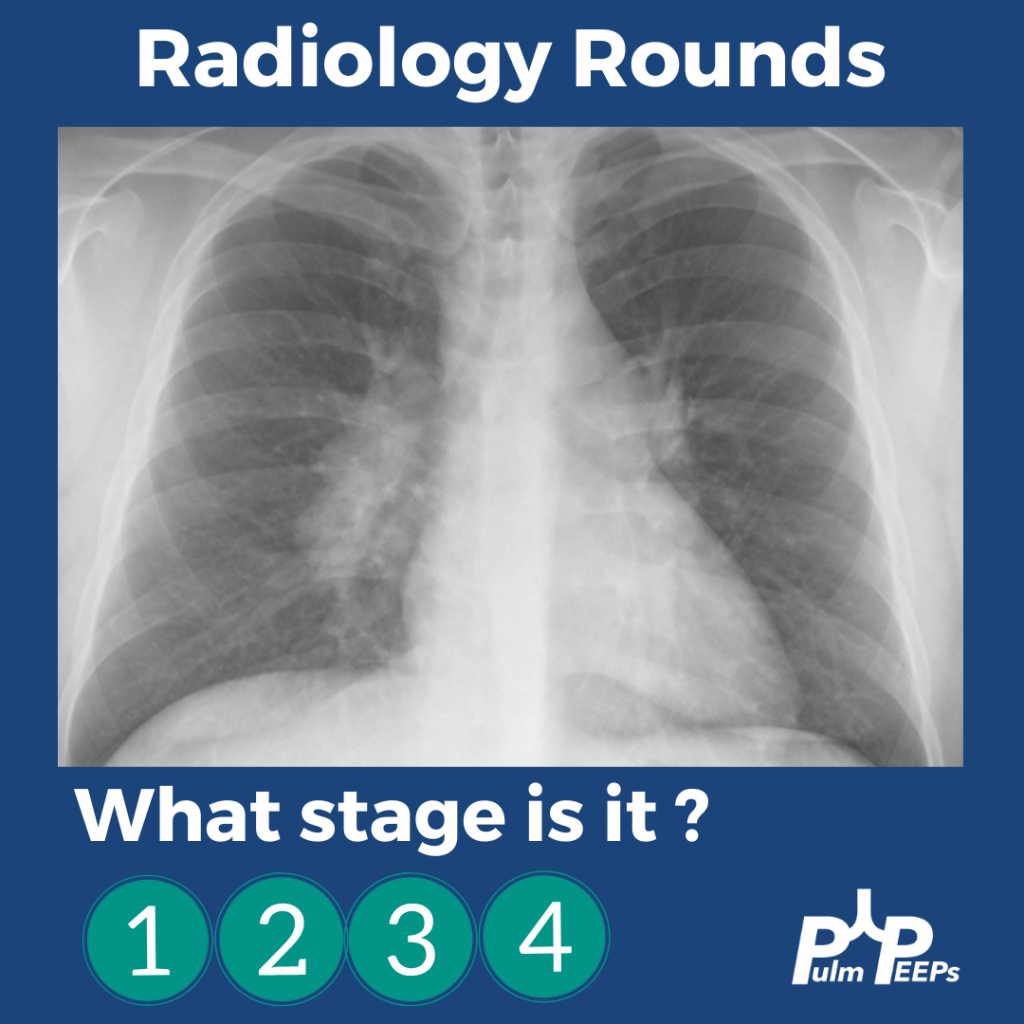
A middle-aged man presents to you after he was found to have hilar adenopathy on a routine chest x-ray.
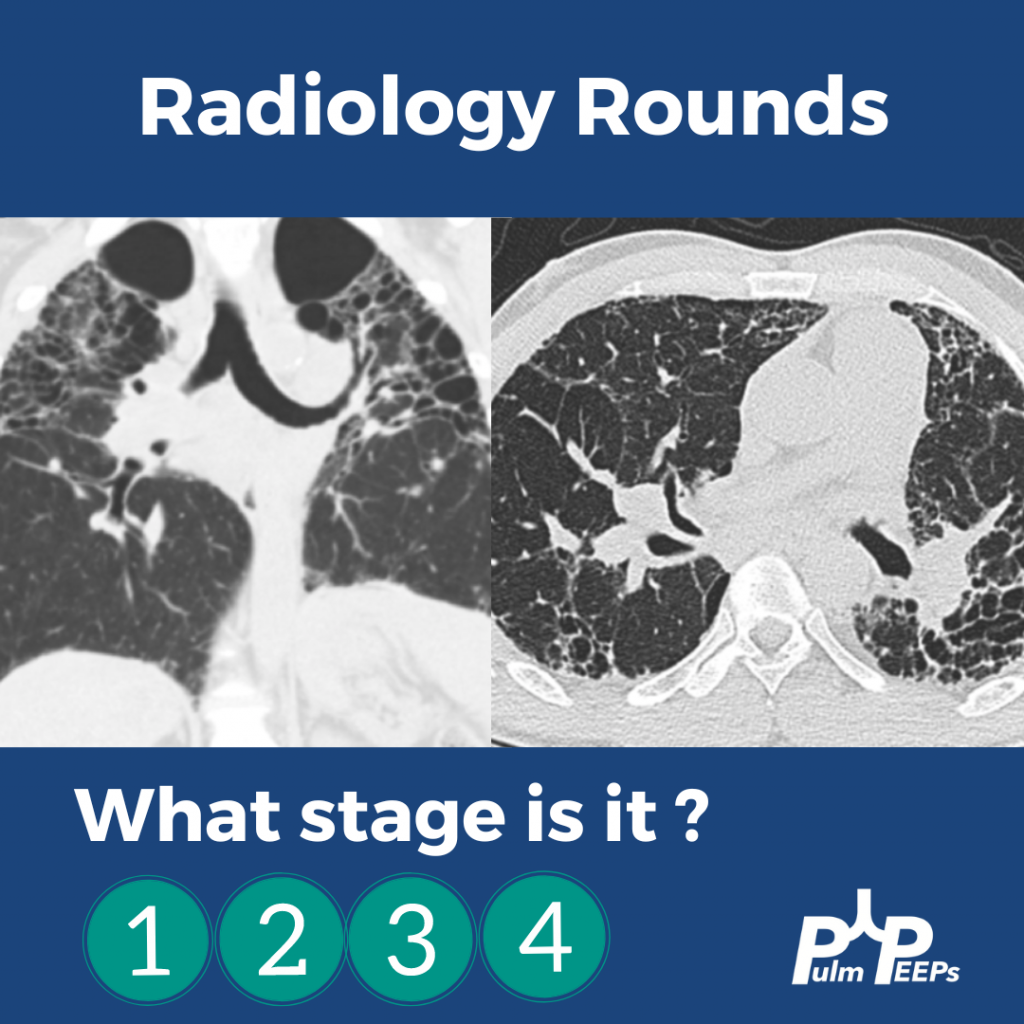
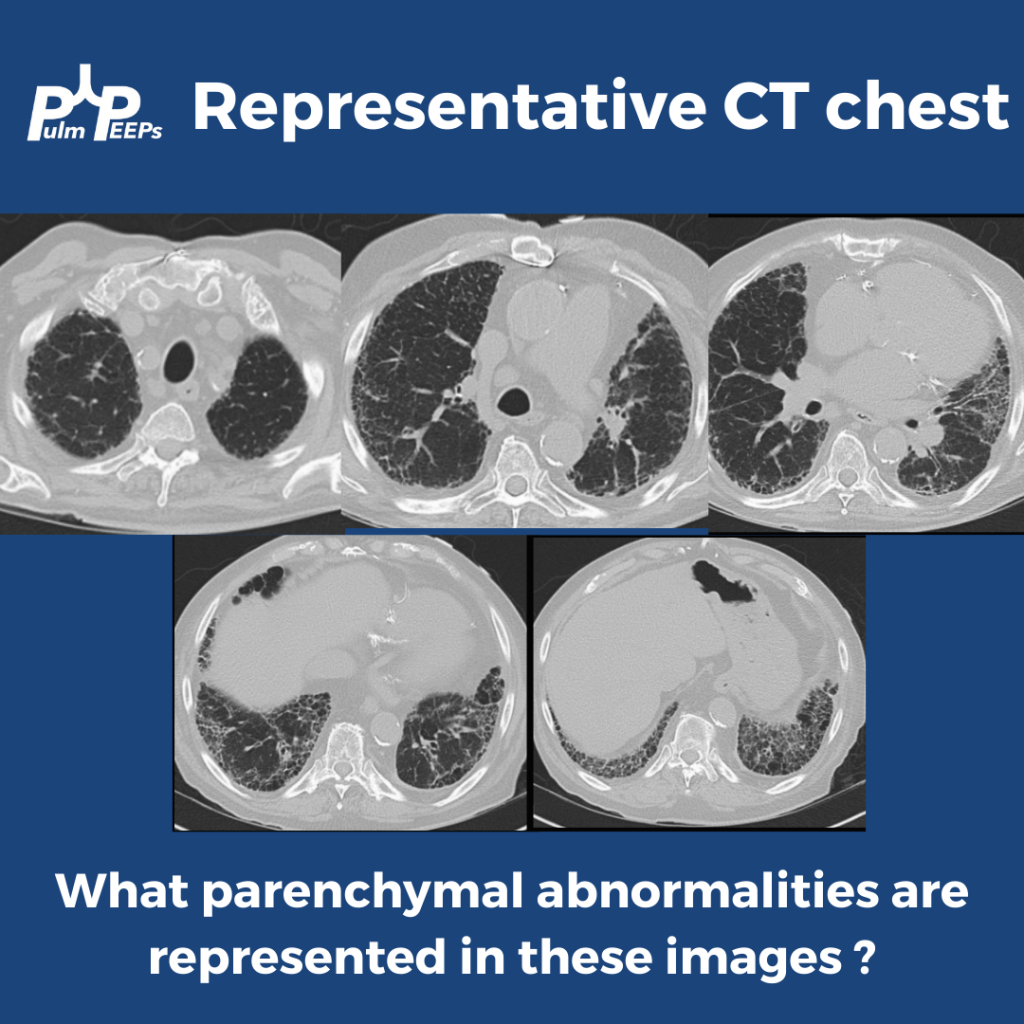
A middle-age man presents with dyspnea on exertion, night sweats and weight loss. You see evidence of bilateral apical disease, and fibrosis with evidence of honeycombing on chest CT.
A young woman presents with dyspnea on exertion and was found to have hilar adenopathy with parenchymal disease.
An elderly man presents with dyspnea on exertion and was found to have nodular parenchymal disease without extensive lymphadenopathy.
This week we are absolutely thrilled to be launching a new series here at Pulm PEEPs. This is the first episode in our new Fellows’ Case Files series. The purpose of this series is to highlight the incredible clinical work that is done by pulmonary and critical care fellows everywhere, share fascinating cases from across the world, and assemble a diverse network of pulmonary and critical care educators. For each episode, we will visit a different institution, and be joined by a current fellow and the Pulmonary and Critical Care Fellowship Program Director. Our aim is to learn from them, amplify some incredible teaching points, and hear about their program. We hope you enjoy it, and if you have a case you want to bring on the series reach out to us on Twitter or at our email pulmpeeps@gmail.com.
Meet Our Guests
Fahid Alghanim is a senior pulmonary and critical care fellow at the University of Maryland. He attended medical school at the Lebanese American University Gilbert and Rose-Marie Chagoury School of Medicine and completed his internal medicine residency at Johns Hopkins Bayview. He has published on topics ranging from lung transplants to patient navigators in the ICU.
Dr. Van Holden is an Associate Professor of Medicine at the University of Maryland School of Medicine and the Pulmonary and Critical Care Fellowship Program director. Clinically, she specializes in interventional pulmonology. She is also an accomplished educator and is very active with the American Thoracic Society. She helped write the 2021 Critical Care Core Curriculum and helped coordinate the 2022 Resident Boot Camp.
Patient Presentation
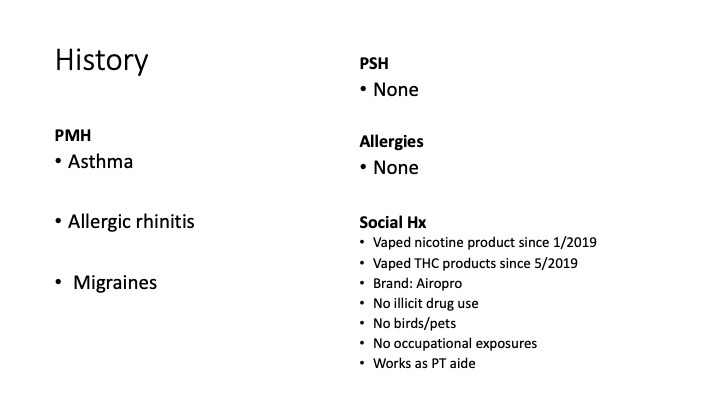
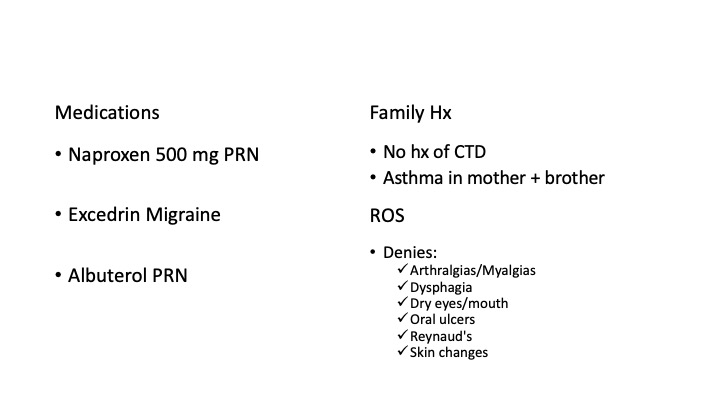
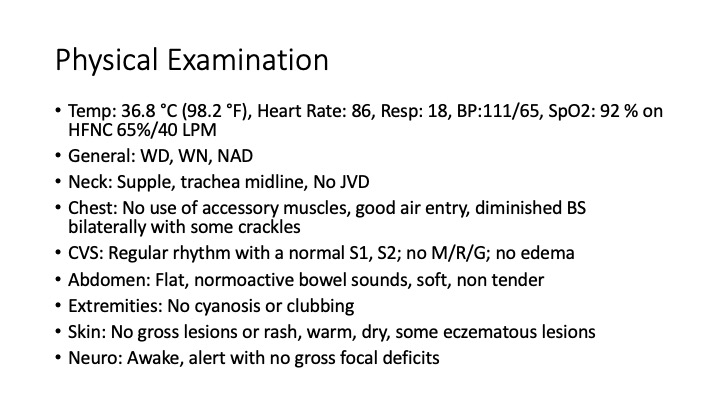
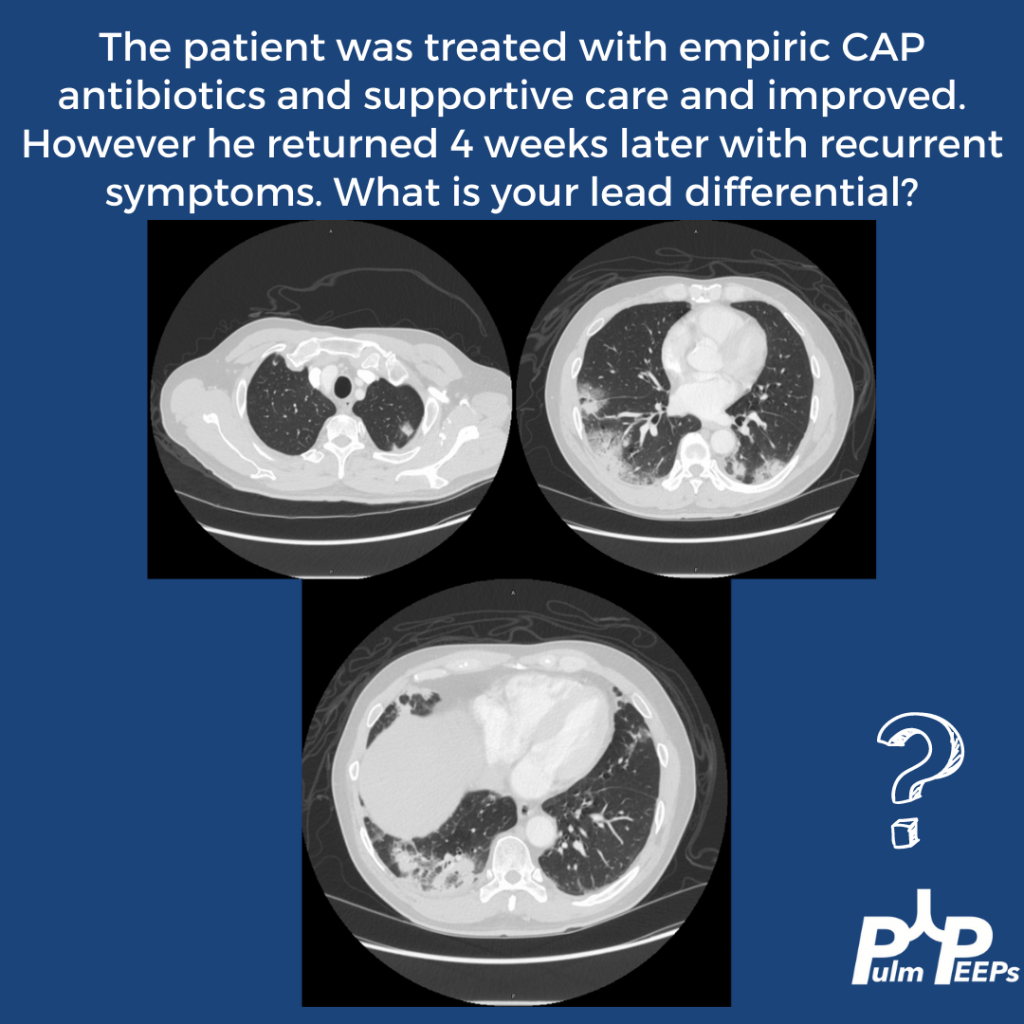
A 26-year-old man presents to his primary care doctor with 1.5 months of intermittent dyspnea, cough, chest tightness, and fatigue. His dyspnea was initially exertional, and he noticed he could do less at the gym. However, in the past 3-4 weeks it has progressed to being even with mild movement. His brother was recently diagnosed and treated for acute bronchitis so he thought this could be similar. In the office, he is noted to be tachypneic with an oxygen saturation of 83% breathing ambient air. A chest X-ray is obtained and he is sent urgently to the emergency department.
Key Learning Points
**Spoilers Ahead** If you want to think through the case on your own we advise listening to the episode first before looking at the infographics below
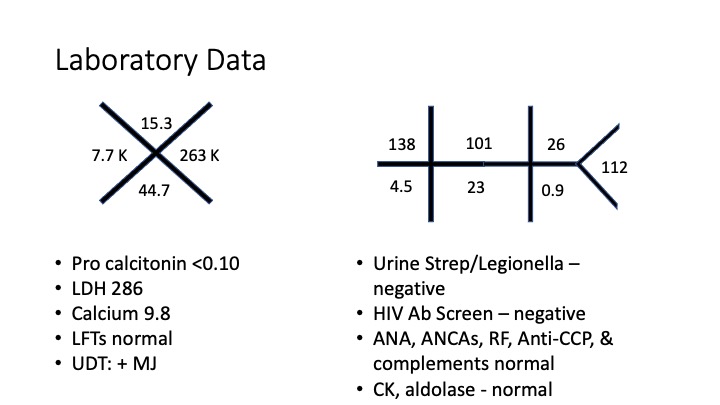
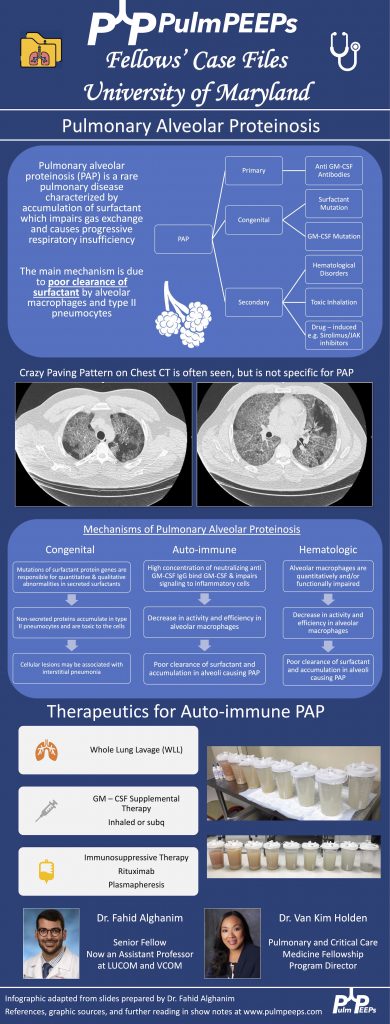
Crazy Paving is a radiological term describing ground glass opacities with superimposed interlobular septal thickening. The differential diagnosis is broad and includes infectious, neoplastic, and autoimmune processes. It is not limited to just Pulmonary alveolar proteinosis (PAP) but is suggestive in an appropriate clinical setting.
PAP is a disorder of surfactant production or clearance and its etiology is divided into three major subgroups. Primary or autoimmune; Secondary such as from toxic inhalations, hematological disorders, or medications; and Congenital
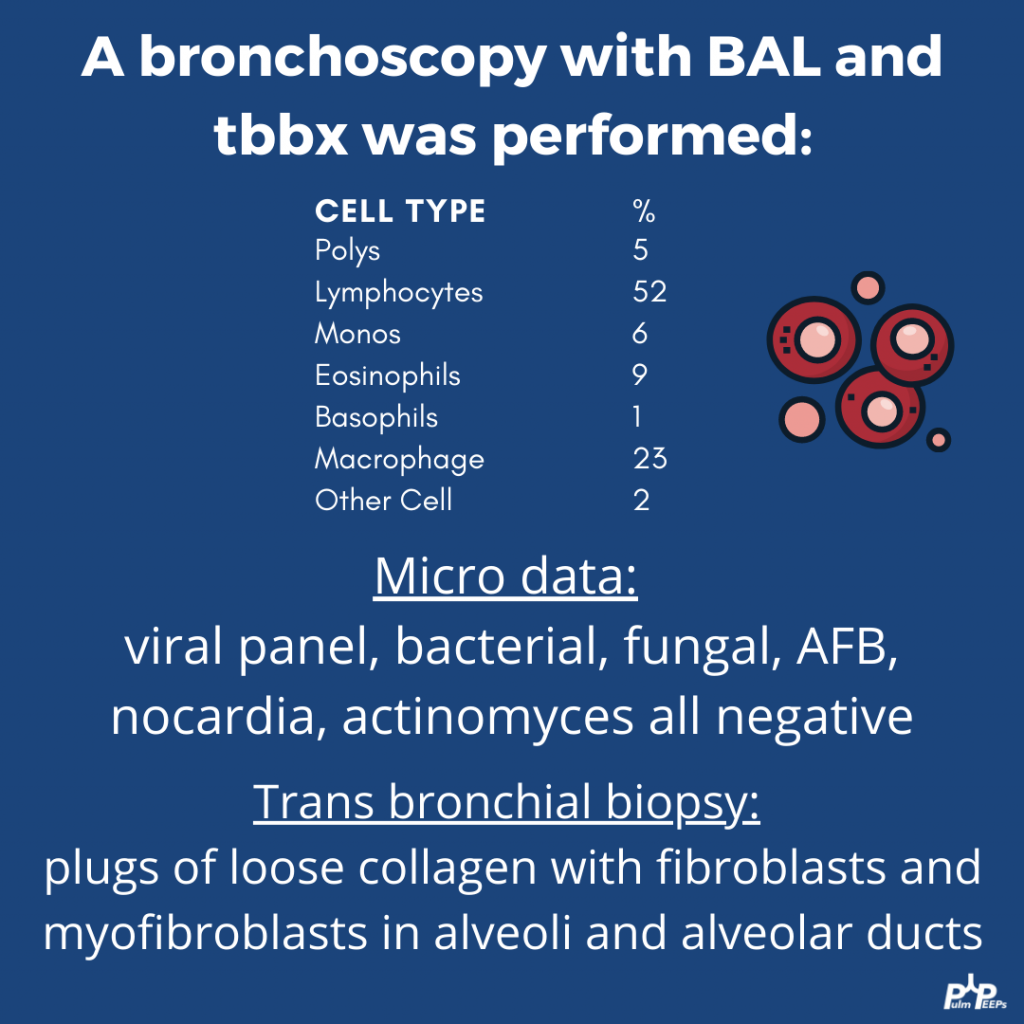
PAP is diagnosed by positive Periodic acid-Schiff (PAS) staining of lipo-proteinaceous material in the distal bronchioles and alveoli on lung biopsy. The diagnosis can be made with PAS-positive BAL staining, but this has limited sensitivity and lung biopsy is necessary for the diagnosis in up to 30 – 35% of cases.
It is important not to anchor on a diagnosis when a patient presents to you for re-evaluation even if seen by a prior expert. This was pivotal in this case!
Please don’t put anything in your lung. Any toxic inhalation exposure could result in significant damage to lung parenchyma and morbidity as a result.
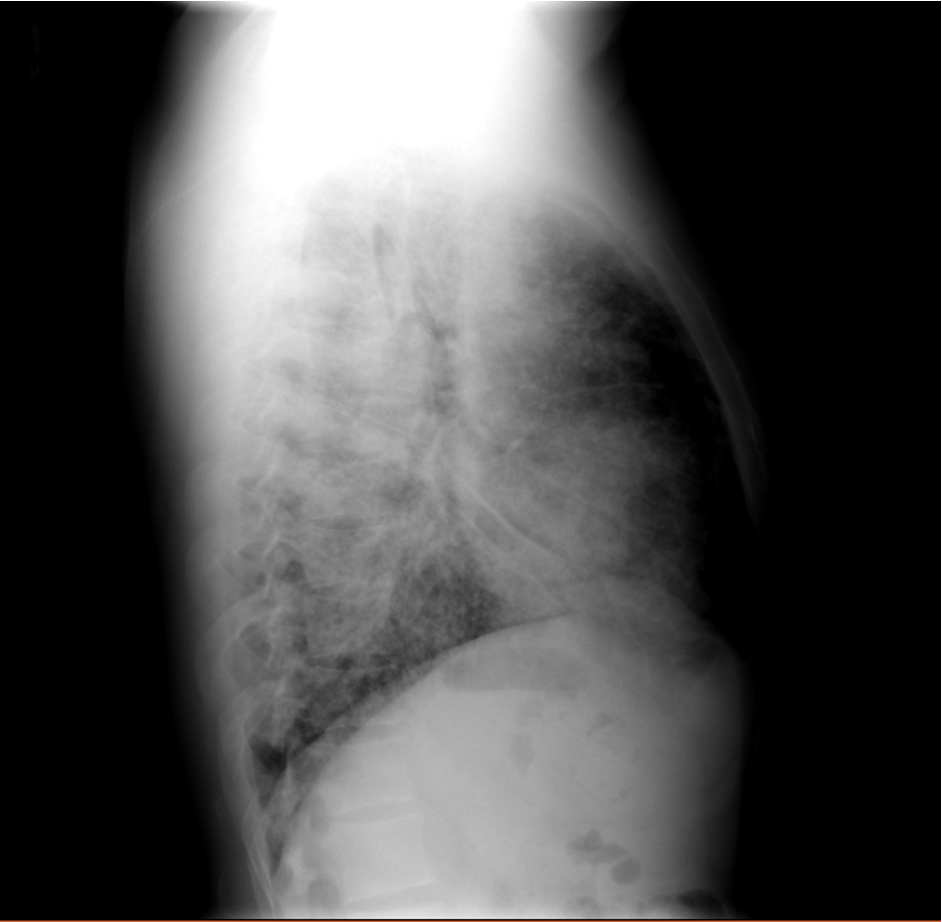
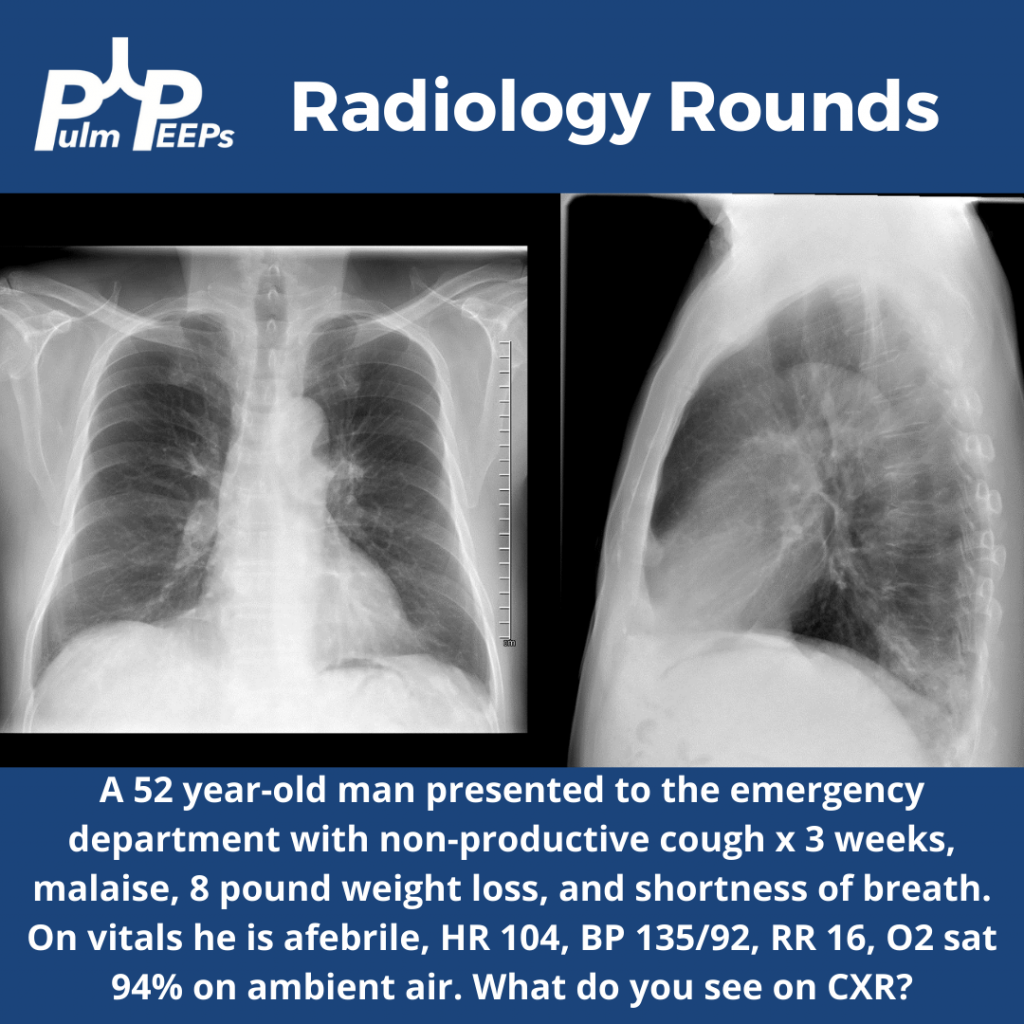
It is Tuesday and time for another #RadiologyRounds!! This is a patient who presented to the emergency department with symptoms of cough, dyspnea, malaise, and weight loss. A PA and lateral CXR was obtained.
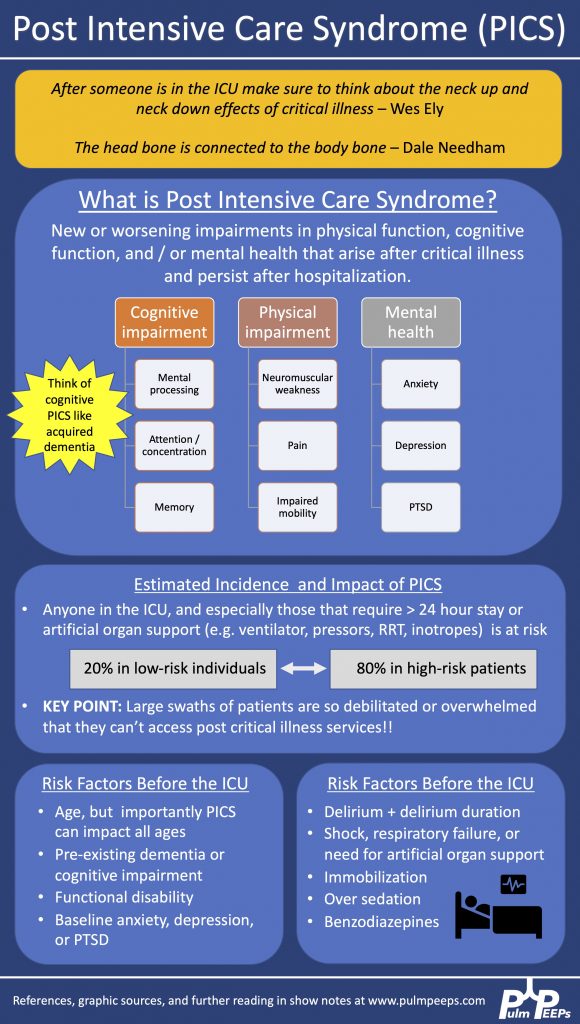
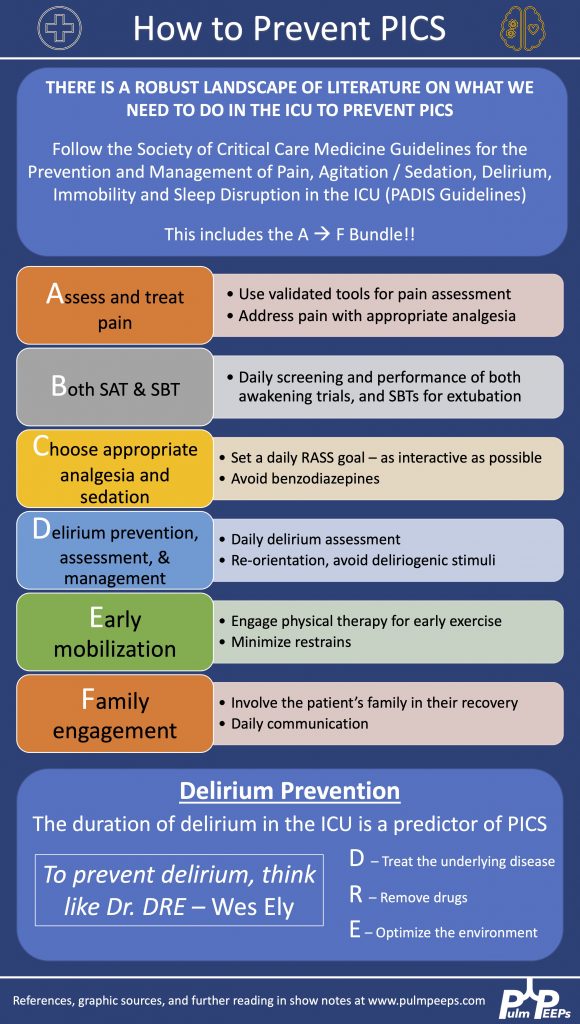
Today on Pulm PEEPs, we are joined by two pioneers in the field of post-intensive care outcomes and delirium research. Drs. Dale Needham and Wes Ely talk to us all about the Post Intensive Care Syndrome (PICS) and cover everything from how it was first recognized, to the impact it has, and, most importantly, what we can do to prevent it. This is a huge topic in the field of critical care and we’re thrilled to be delving into it with such knowledgeable guides.
Meet Our Guests
Wes Ely is the Grant W. Liddle Chair in Medicine and a Professor of Medicine at Vanderbilt University Medical Center. He is also the Associate Director of Aging Research at the VA Tennessee Valley Geriatric Research and Education Clinical Center and the co-director of the Critical, Illness, Brain Dysfunction and Survivorship Center. He has published 100s of manuscripts on critical illness survivorship and delirium. He also published a book called “Every Deep-Drawn Breath” about his and his patients’ experiences in the ICU and about the ramifications of critical illness. All net proceeds for the book are going to the CIBS Center Endowment for Survivorship
Dale Needham is a Professor of Medicine at Johns Hopkins, where he is also the Medical Director of the Critical Care Physical Medicine and Rehabilitation Program and the Director of the Outcomes After Critical Illness and Surgery Group. He is the author of 100s of publications focusing on post-ICU outcomes and has received numerous research grants from the NIH and other organizations.
Key Learning Points
Visit our website www.pulmpeeps.com to see the key learning points from this episode summarized in two infographics.
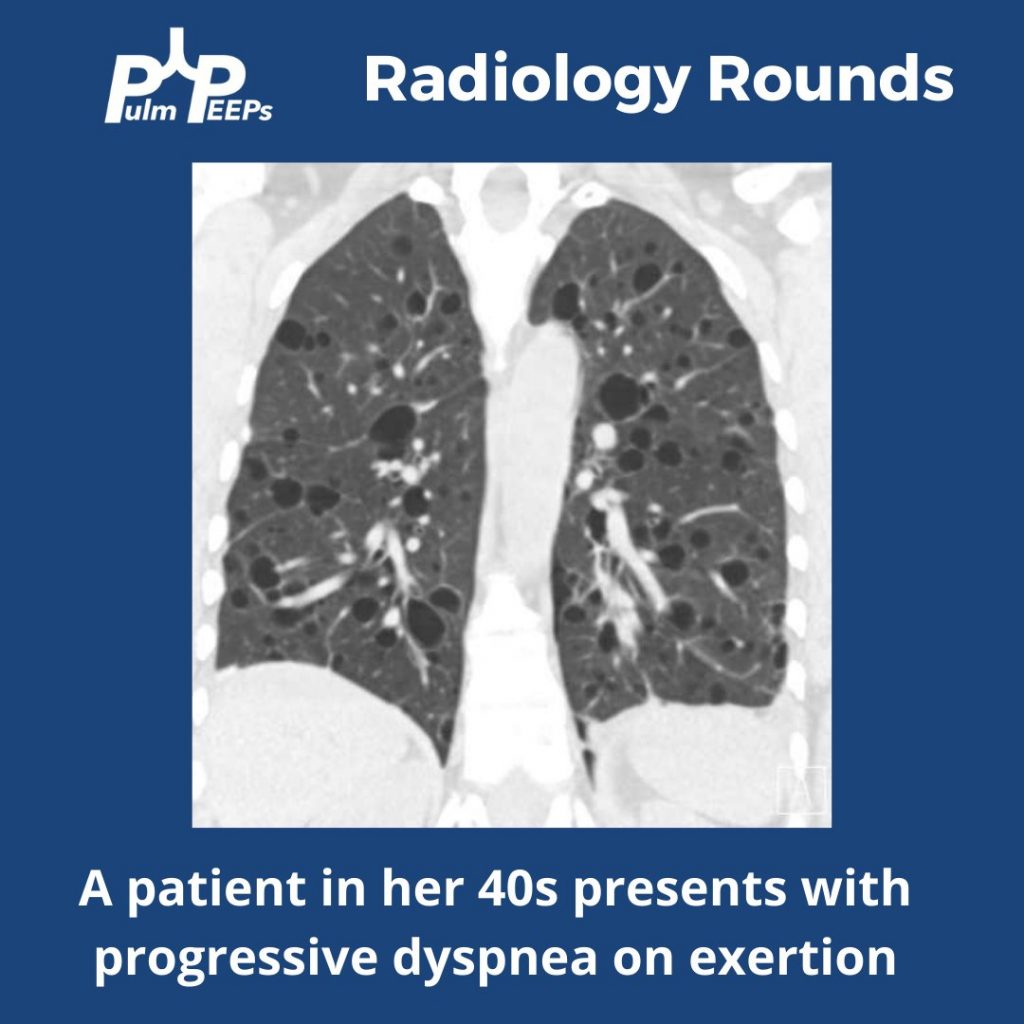
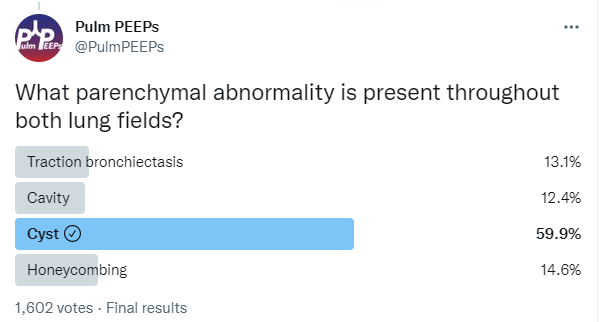
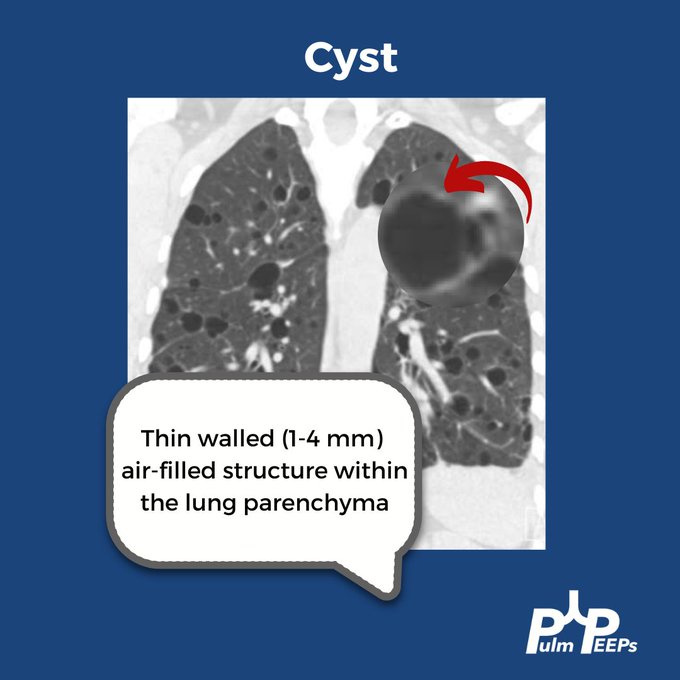
Time for another #RadiologyRounds!! This week we’re looking at the coronal CT scan views, which can be extremely helpful and are often under-utilized. Follow us on Twitter to work through Radiology Rounds cases as they come out.
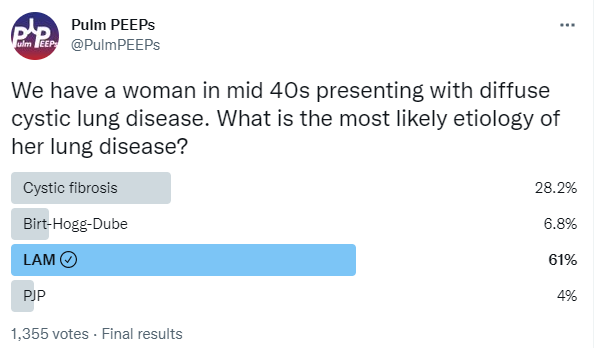
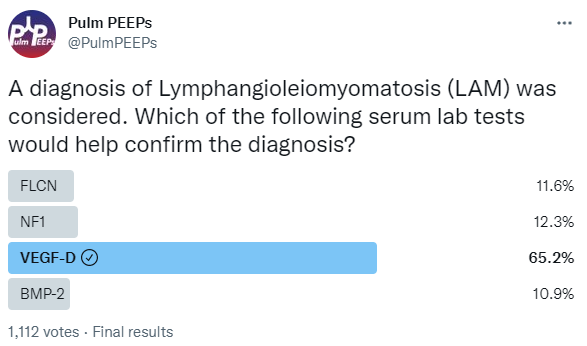
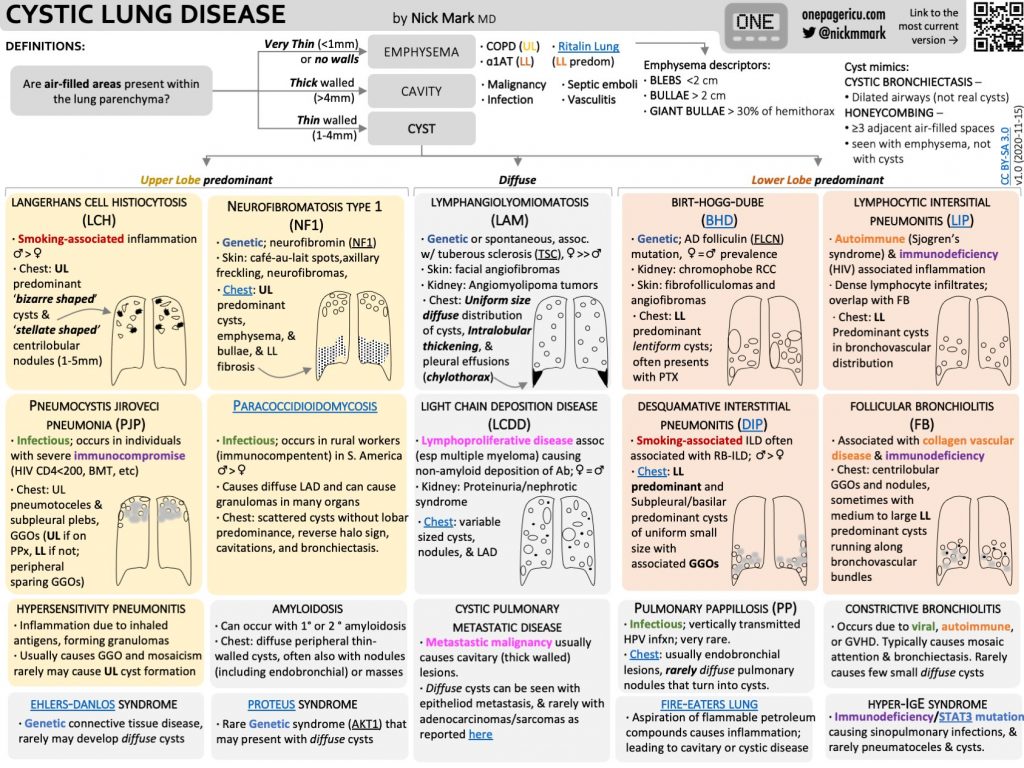
Our patient had an elevated VEGF-D level, a renal angiomyolipoma identified on CT abdomen, and imaging with diffuse cystic lung disease confirming her diagnosis of LAM. Make sure to check out the ICUOnePager made by Dr. Nick Mark.
This week on Pulm PEEPs, we are continuing our Top Consults series with a discussion on the work-up and diagnosis of Pulmonary Hypertension. See our prior Radiology Rounds on signs of PAH on CT scan, and listen to our follow-up episode on right heart catheterizations for some background before this episode… or dive right in! We’ll cover everything from history and physical, to recent guideline changes in the definition of PH, and much, much more!
Meet Our Guests
Erika Berman Rosenzweig is a Professor of Pediatrics and the Director of the Pulmonary Hypertension Center and CTEPH Program at Columbia University Medical Center / New-York Presbyterian Hospital. She is an active member of the Pulmonary Hypertension Association, was the Editor-in-Chief of Advances in Pulmonary Hypertension and is on the Scientific Board of the World Symposium on PH.
Catherine Simpson is an Assistant Professor of Medicine at Johns Hopkins Hospital and is one of the faculty members in our Pulmonary Hypertension group. Her clinical and research areas of expertise are in pulmonary vascular disease and right heart function. Her research is focused on novel biomarker discovery and metabolomics in pulmonary vascular disease.
Cyrus Kholdani is an Instructor in Medicine at Beth Israel Deaconess Medical Center and Harvard Medical School. He is also the director of the Pulmonary Hypertension Program at BIDMC, and is actively involved in clinical care and clinical research in a variety of pulmonary vascular disease domains.
Consult Patient
Ms. Pamela Harris (PH) is a 47-year-old woman with PMH of migraines, obesity s/p gastric sleeve (BMI now 33), and a history of remote DVT in her 20s while on OCP s/p 6 months of AC who is referred to pulmonary hypertension clinic for evaluation of dyspnea on exertion. She has actually had dyspnea for some time and previously it has been attributed to her weight. Based on this, she pursued a gastric sleeve and has lost 55 pounds, but continues to have shortness of breath. She has no cough, and does not get dyspnea at rest, but notes that after 1 flight of stairs, or 2-3 blocks on flat ground she has shortness of breath. She saw her PCP and had basic labs, basic spirometry, and an echocardiogram. He did not note anything significant on examination in the notes.
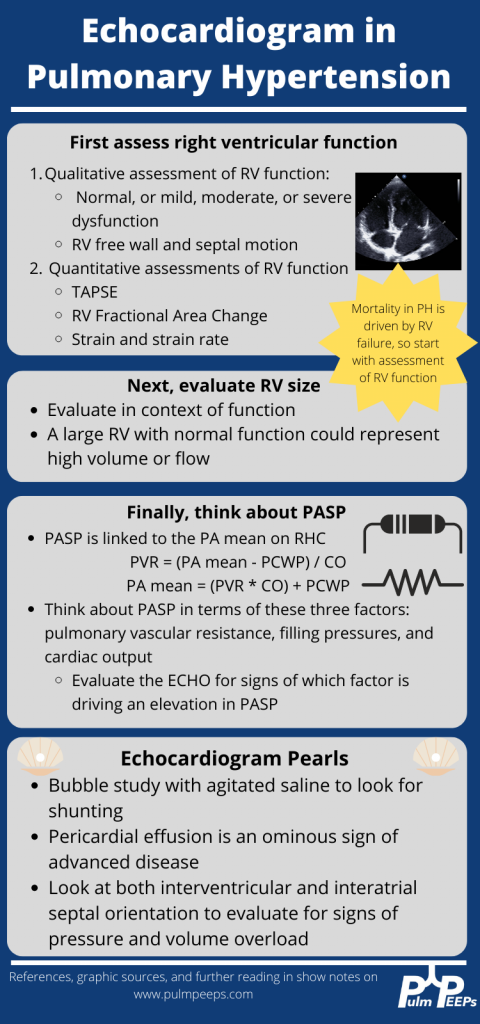
The labs had no anemia, and normal renal and liver function. Her serum bicarbonate was 25 and there was no blood gas. Spirometry showed an FVC 82% predicted, FEV1 83% predicted, and FEV1/FVC was 99% predicted. The echocardiogram had normal LVEF, mild LVH, normal RV size and function qualitatively. There was mild TR with tricuspid valve peak regurgitant velocity of 3.4 m/sec. The estimated PASP + RA pressure (based on normal IVC diameter 2.1 cm) was 46 mmHg.
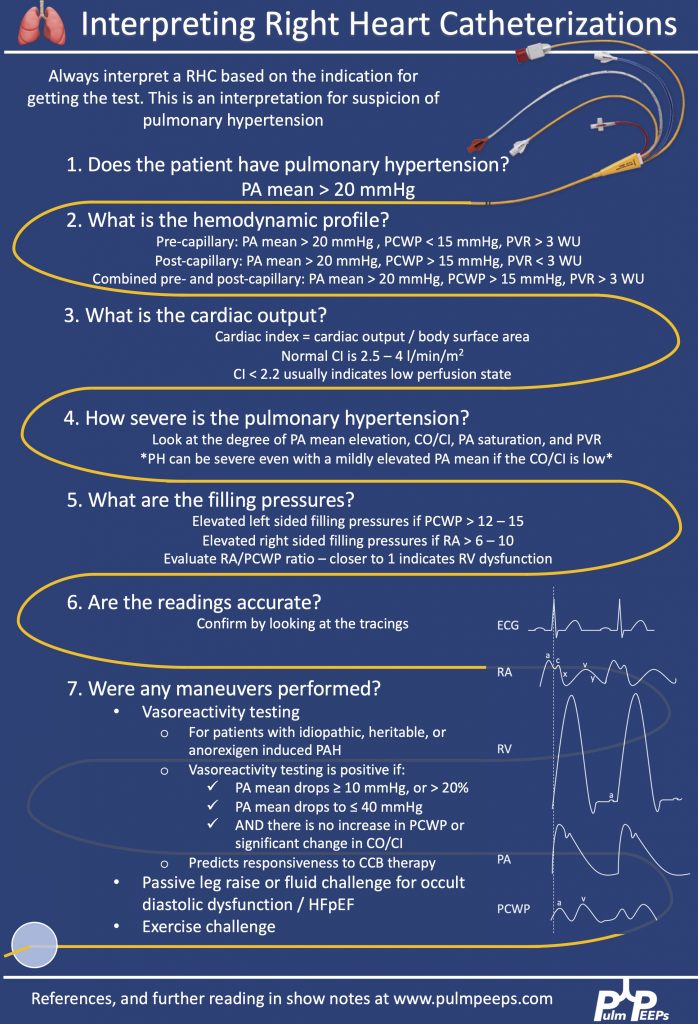
RHC: Systemic BPs 140s/90s, with O2 saturations 97-98% on RA throughout. RA mean pressure was 9, RV was 48 with an RVEDP of 17, PA was 48/27 with mean of 34, and PCWP mean was 11. CO/CI by Fick was 5.56 / 2.42, and by thermo was similar, 5.8 / 2.52. Her PA sat was 62%, and PVR was 3.97 WU.
Key Learning Points
History
Understand the constellation of symptoms and the functional limitation
The goal is to assign a WHO functional class by the end of the visit
Evaluate the time course and evolution of the symptoms
Concerning symptoms that need to be addressed
Palpitations
Pre-syncope
Syncope
Chest pain
LE edema
Evaluate for risk factors to explain or contribute to pulmonary hypertension
Signs or symptoms of OSA
Signs or symptoms of auto-immune disease
Raynauds
Skin changes
Family history
Heritable lung disease
Clotting disorders
Auto-immune disease
Social history
Exposure history
Smoking
Physical Exam
Look for signs that confirm PH
Loud P2
Accentuated with elevated PVR
Can hear pretty early on. Could be one of the earliest findings
TR murmur – pansystolic murmur at RUSB
Diastolic murmur if severe pulmonary insufficiency
Look for signs of right heart failure
JVD
S4 gallop – later in course
RV heave – later in course
Peripheral edema
Pulsatile liver or hepatosplenomegaly
Look for signs of other secondary causes of PH
Mitral regurgitation or aortic stenosis murmur
Asymmetric lower extremity edema
Pulmonary edema
Skin findings concerning for auto-immune disease or liver disease
Arthritis
Work up for etiology of PH
CBC with diff – myeloproliferative and hemolytic anemia
This week’s #RadiologyRounds is brought to you by our newest Contributor, Matthew Tsai! Matt will be continuing to work with us to bring you great cases and images and we are thrilled to have him on the team! Follow us on Twitter and Instagram for our Radiology Rounds, podcast episode releases, and more!
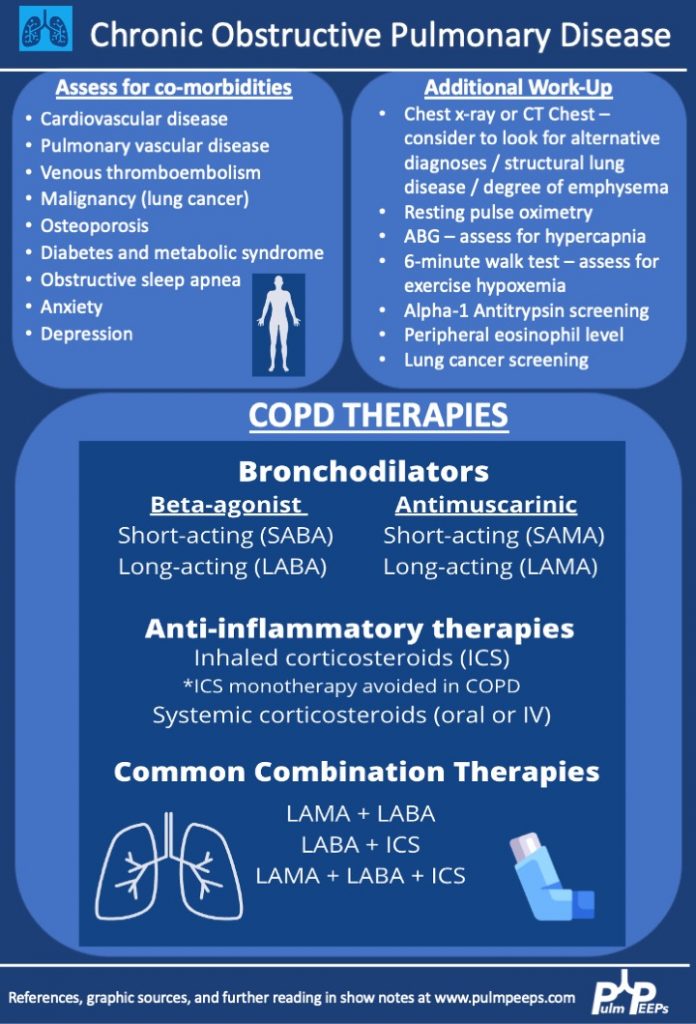
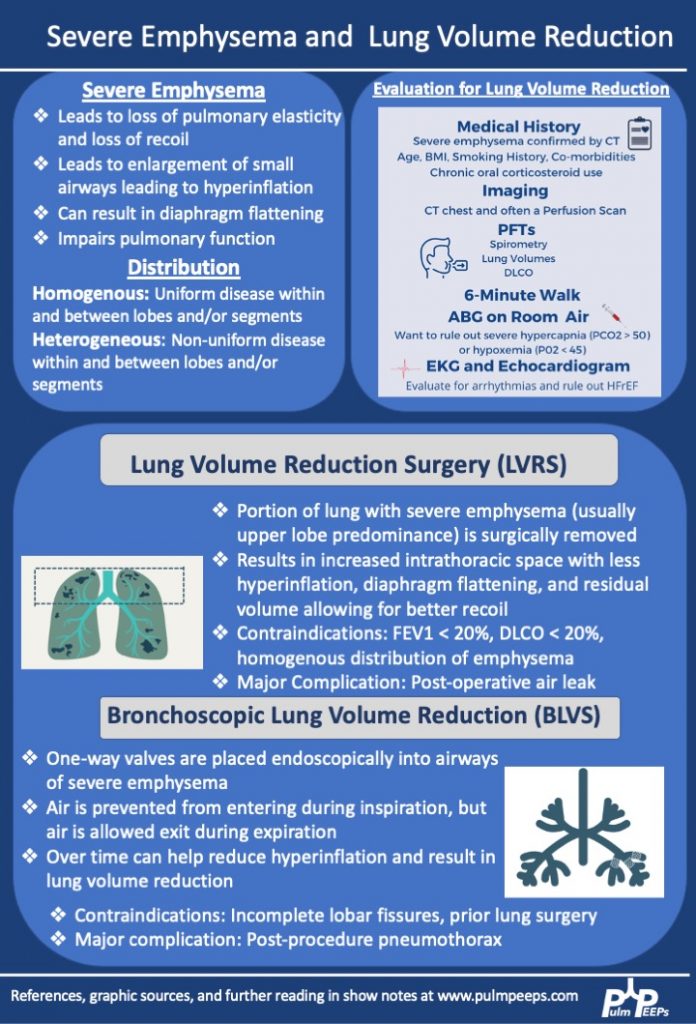
We are extremely excited for the third and final installment in our Pulm PEEPs and ATS Clinical Problems Assembly collaborative series on COPD. Today, we are joined by Drs. Jessica Bon, Michael Lester, and Niru Putcha to discuss severe COPD management and the role of lung volume reduction procedures. If you missed the first two parts of our series, make sure to check out episode 1 on COPD diagnosis and initial management, and episode 2 on COPD exacerbations.
Meet our Guests
Jessica Bon is an Associate Professor of Medicine at the University of Pittsburgh School of Medicine where she is also the Program Director for the Pulmonary and Critical Care Medicine Fellowship. Her research and clinical interests focus on lung disease progression in COPD and she manages patients with difficult-to-treat and severe COPD and evaluates patients for lung volume reduction surgery. Jessica was the chair of the ATS Clinical Problems Assembly Programming Committee from 2021 – 2022.
Michael Lester is an Assistant Professor of Medicine at Vanderbilt University Medical Center. Michael’s interests span both pulmonary and critical care medicine. He specializes in patients with advanced COPD and evaluation for bronchoscopic lung volume reduction surgery.
Niru Putcha is an Associate Professor of Medicine at Johns Hopkins School of Medicine and is an integral member and mentor in the Obstructive Lung Disease Group. Her research and clinical interests focus on the role of comorbidities on clinical outcomes in individuals with COPD. She also manages patients with difficult-to-treat and severe COPD and evaluates patients for lung volume reduction surgery. Niru is also the new chair of the ATS Clinical Problems Assembly Programming Committee.
Key Learning Points
Patients with advanced COPD should also be considered for lung transplantation. We will have an episode on lung transplant coming up soon!
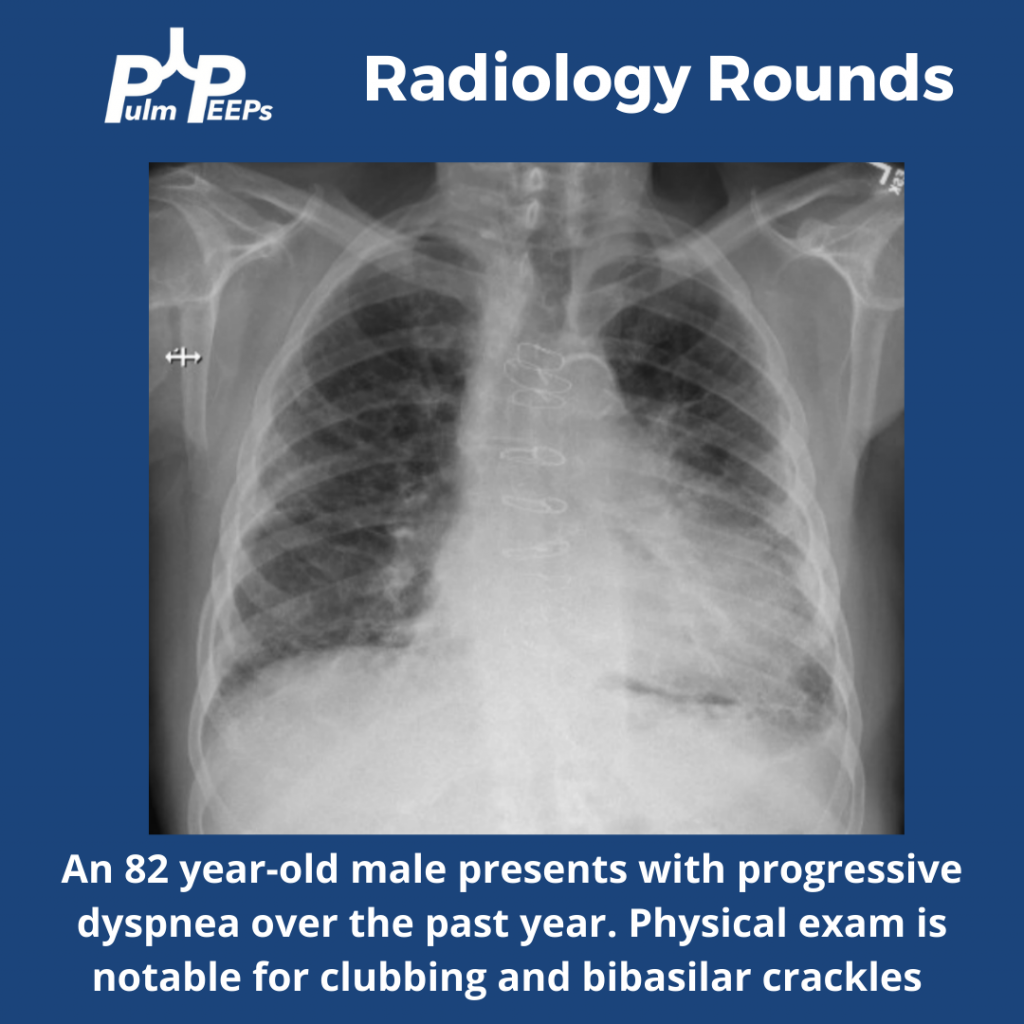
This week on #RadiologyRounds we are extremely excited to share a case brought to you by one of our new Associate Editors, Leon Mirson! Enjoy, and follow us on Twitter and Instagram for content delivered to you weekly!
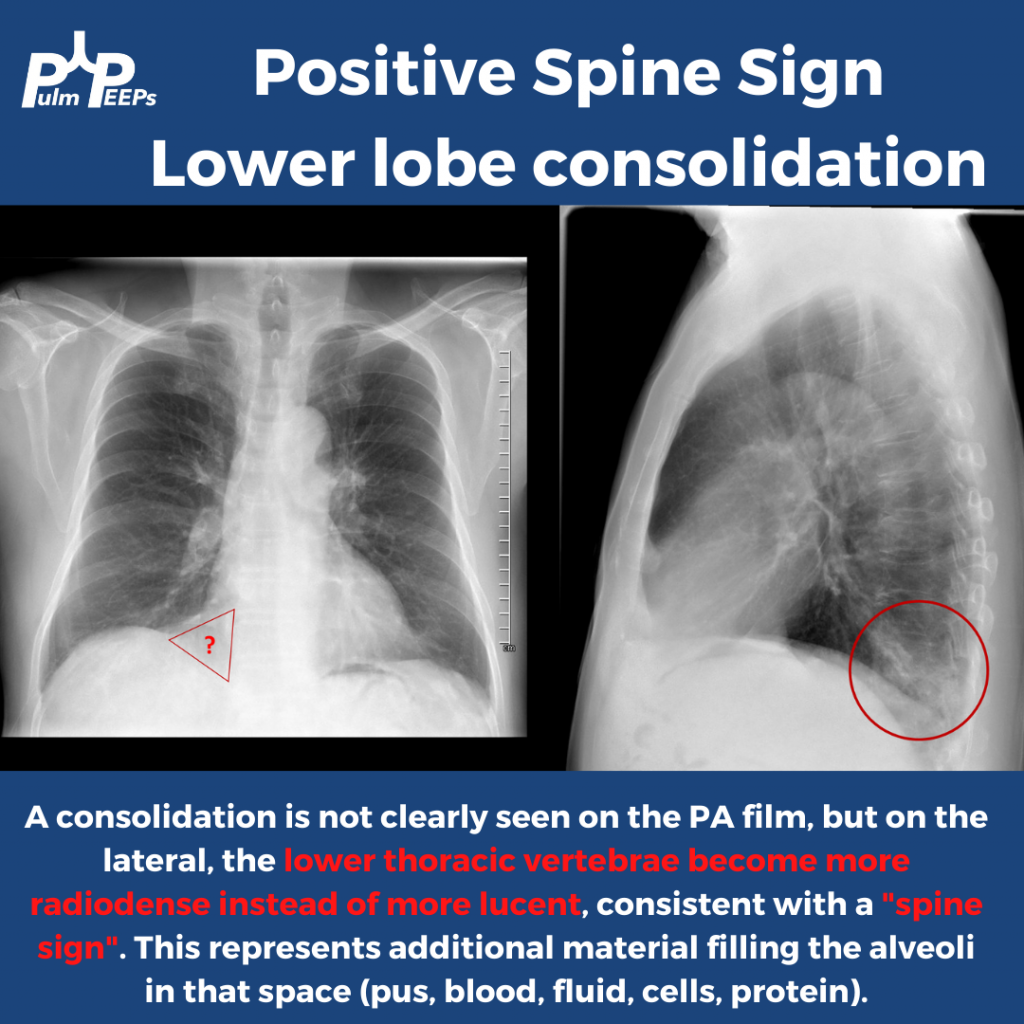
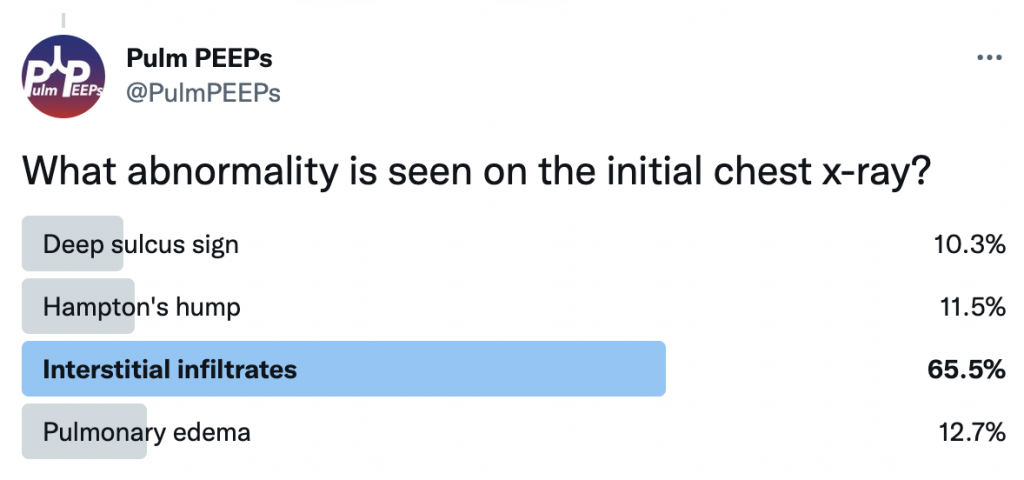
What abnormalities do you see on this CXR to help explain the patient’s presentation?
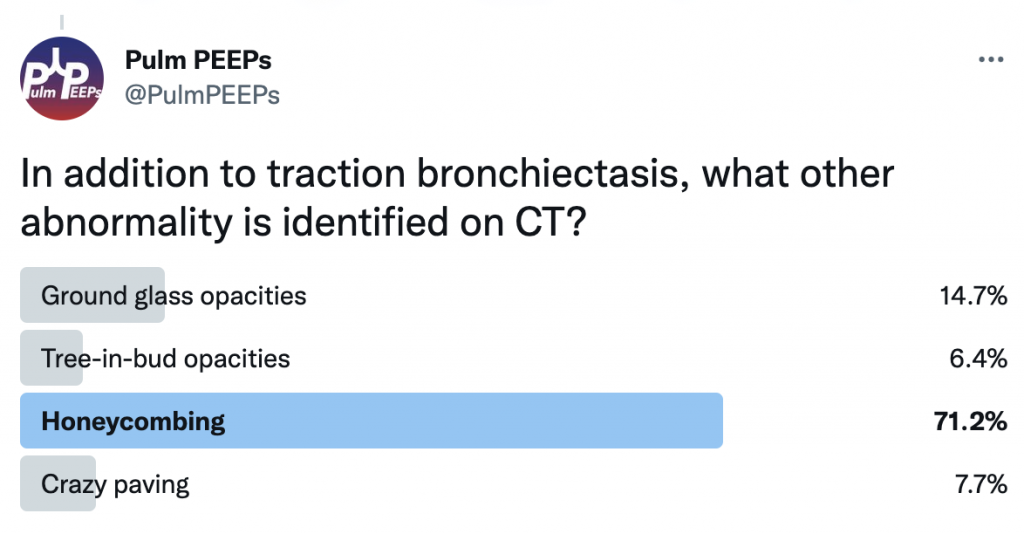
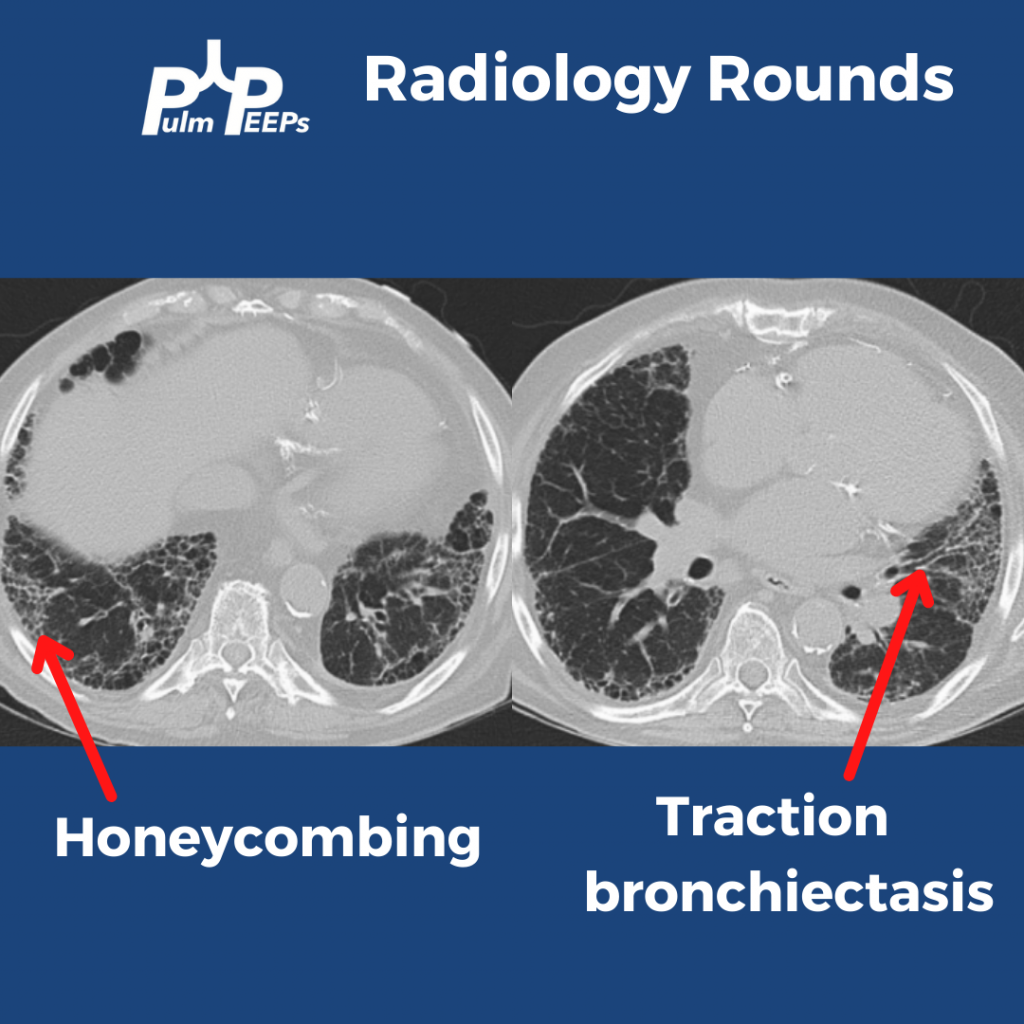
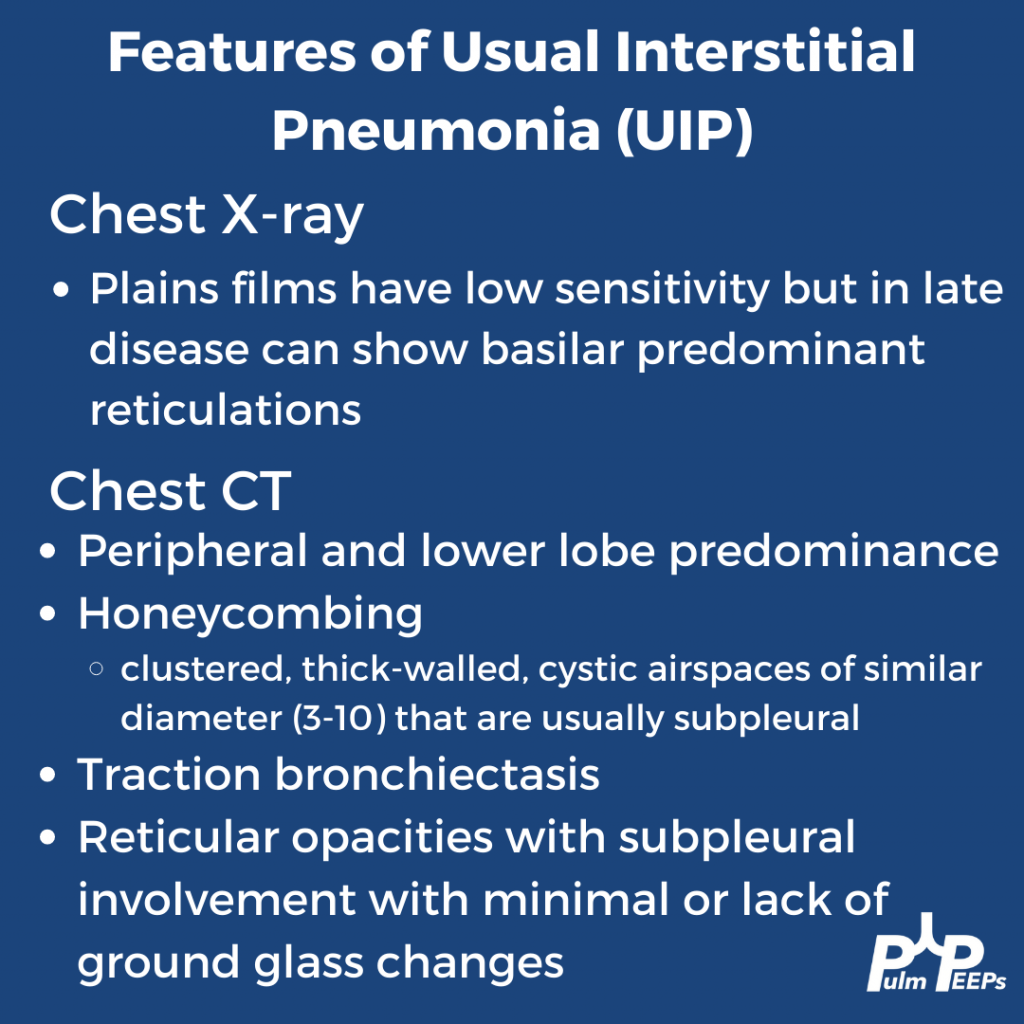
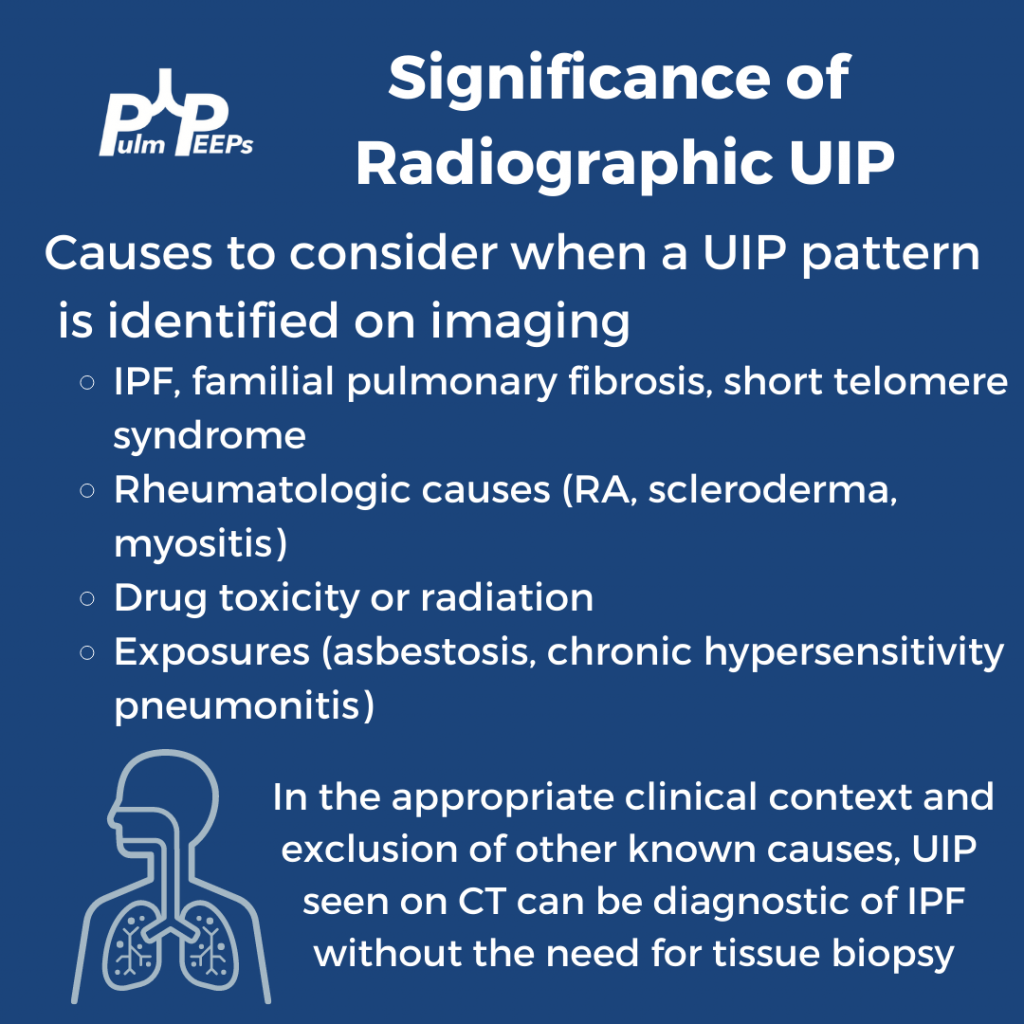
The CT scan has reticular changes consistent with interstitial lung disease and there are multiple features that help us define the pattern of the ILD. His CT notably has very few ground-glass opacities, there is traction bronchiectasis, and honeycombing with a basilar and peripheral / sub-pleural predominance.
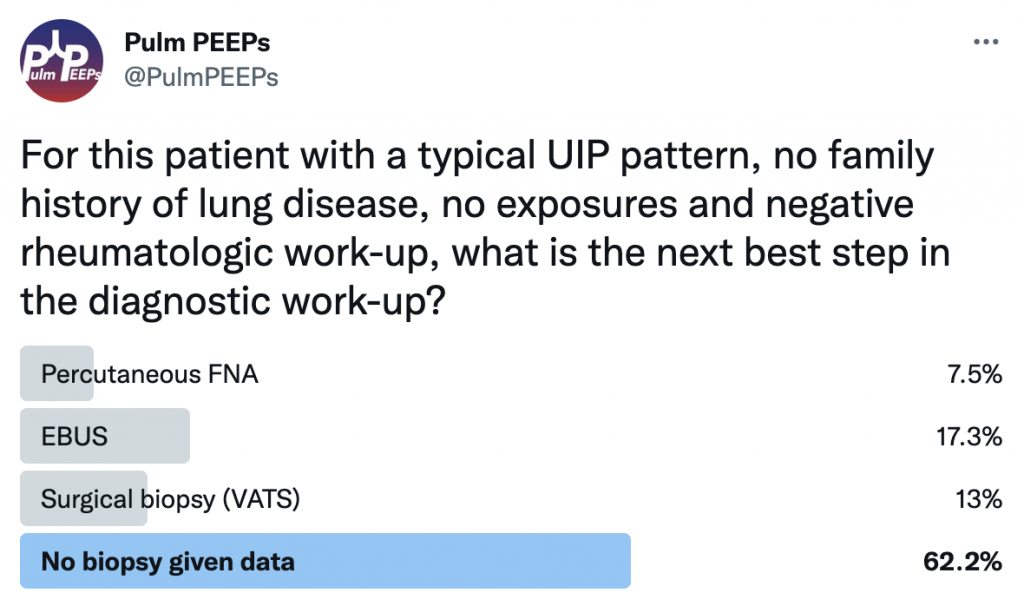
Taking all these features together, the patient’s radiographic presentation is consistent with Usual Interstitial Pneumonia (UIP)
This patient had a thorough history taken and he had no prior smoking and no occupational or environmental exposures of significance. He had no family history of interstitial lung disease. A broad history was taken regarding symptoms of connective tissue disease and a broad serologic workup was sent, all of which were unremarkable. What would you want to do next diagnostically?
We are thrilled here @PulmPEEPS to have our first episode with one of our new Associate Editors Luke Hedrick, and our first nephrology consultant Jeff William. Luke will walk us through an interesting case presentation, and we will discuss an approach to severe weakness in our patient in the ICU.
Meet Our Guests
Jeff William is an Assistant Professor of Medicine at Harvard Medical School and Beth Israel Deaconess Medical Center, where he is also the Associate Director of the Nephrology Fellowship Program. He completed a Medical Education Research Fellowship at Harvard Medical School, and is very involved in residency, fellowship and medical student education.
Patient Presentation
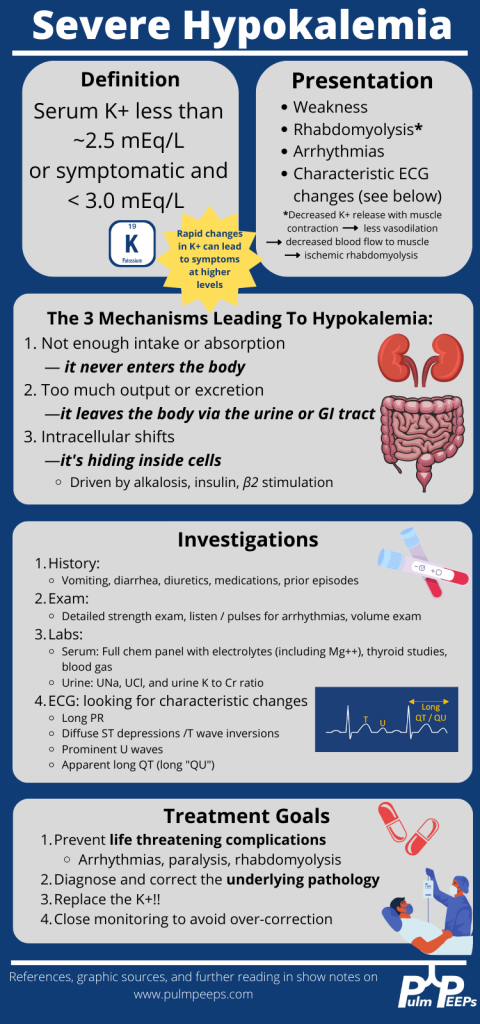
We have a man in his 40s with a past medical history of asthma, hypertension, and acid reflux who was brought in by EMS with back pain and profound proximal lower extremity weakness. He reports mild weakness in his legs which started 2 days ago, but this morning his weakness acutely worsened to the point that he can’t lift his legs out of the bed. He also has some cramping pain in his thighs. He additionally has had mild shortness of breath and yesterday went to an urgent care where he was given steroids and swabbed for COVID (which was negative).
Key Learning Points
**Spoilers Ahead** If you want to think through the case on your own we advise listening to the episode first before looking at the infographics below
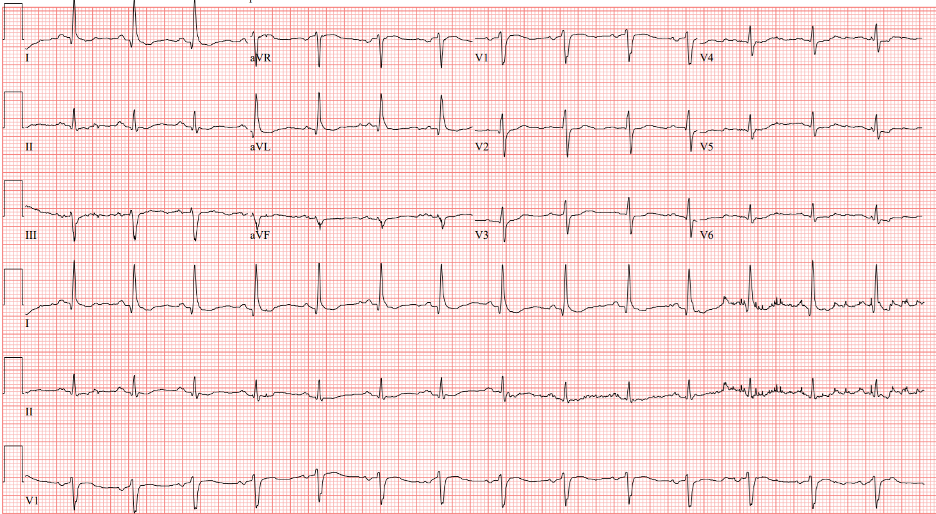
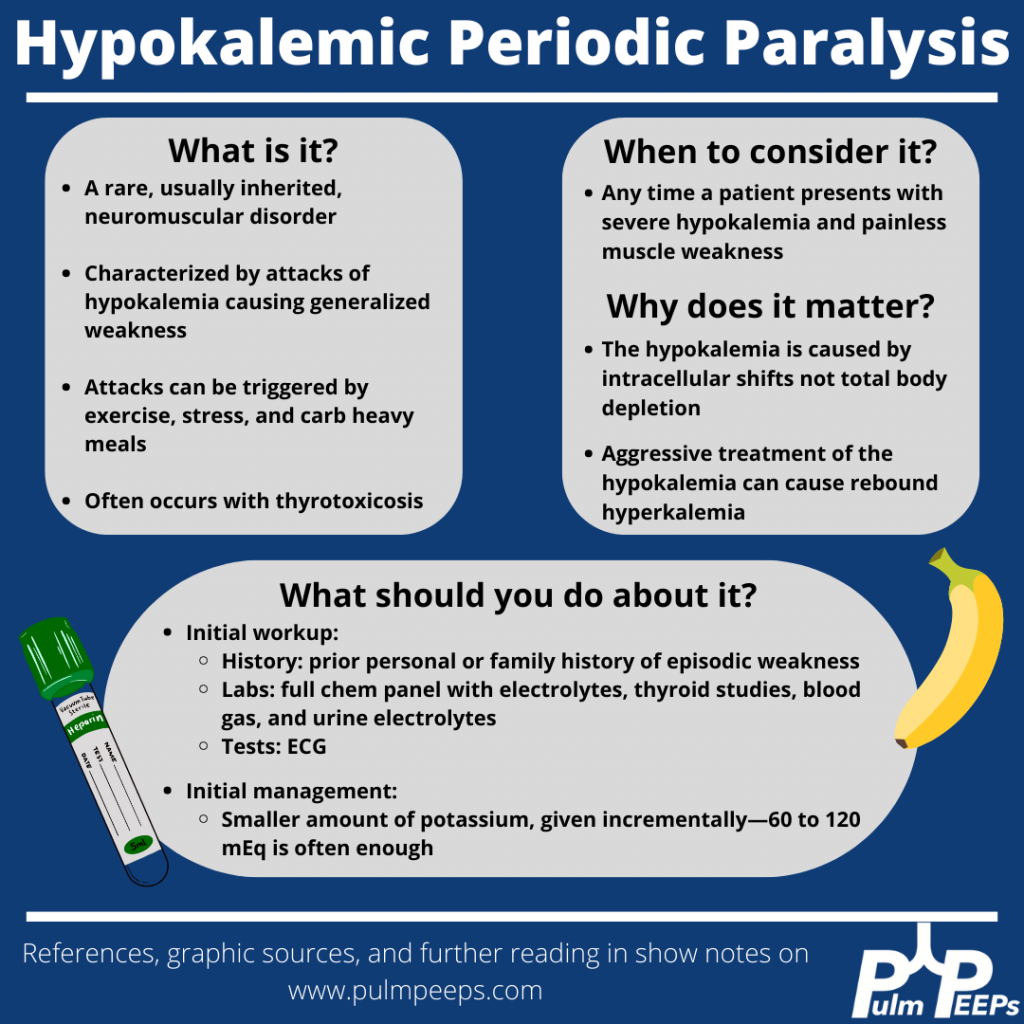
Although our patient’s etiology of severe hypokalemia was thought to be secondary to thiazide diuretic use, it is important to be familiar with hypokalemic periodic paralysis.
References
Knochel JP, Schlein EM. On the mechanism of rhabdomyolysis in potassium depletion. J Clin Invest. 1972 Jul;51(7):1750-8. doi: 10.1172/JCI106976.
Wang X, Han D, Li G. Electrocardiographic manifestations in severe hypokalemia. J Int Med Res. 2020 Jan;48(1):300060518811058. doi: 10.1177/0300060518811058.
Venance SL, Cannon SC, Fialho D, Fontaine B, Hanna MG, Ptacek LJ, Tristani-Firouzi M, Tawil R, Griggs RC; CINCH investigators. The primary periodic paralyses: diagnosis, pathogenesis and treatment. Brain. 2006 Jan;129(Pt 1):8-17. doi: 10.1093/brain/awh639.
Lin SH, Lin YF, Halperin ML. Hypokalaemia and paralysis. QJM. 2001 Mar;94(3):133-9. doi: 10.1093/qjmed/94.3.133.
Lin SH, Lin YF, Chen DT, Chu P, Hsu CW, Halperin ML. Laboratory tests to determine the cause of hypokalemia and paralysis. Arch Intern Med. 2004 Jul 26;164(14):1561-6. doi: 10.1001/archinte.164.14.1561.