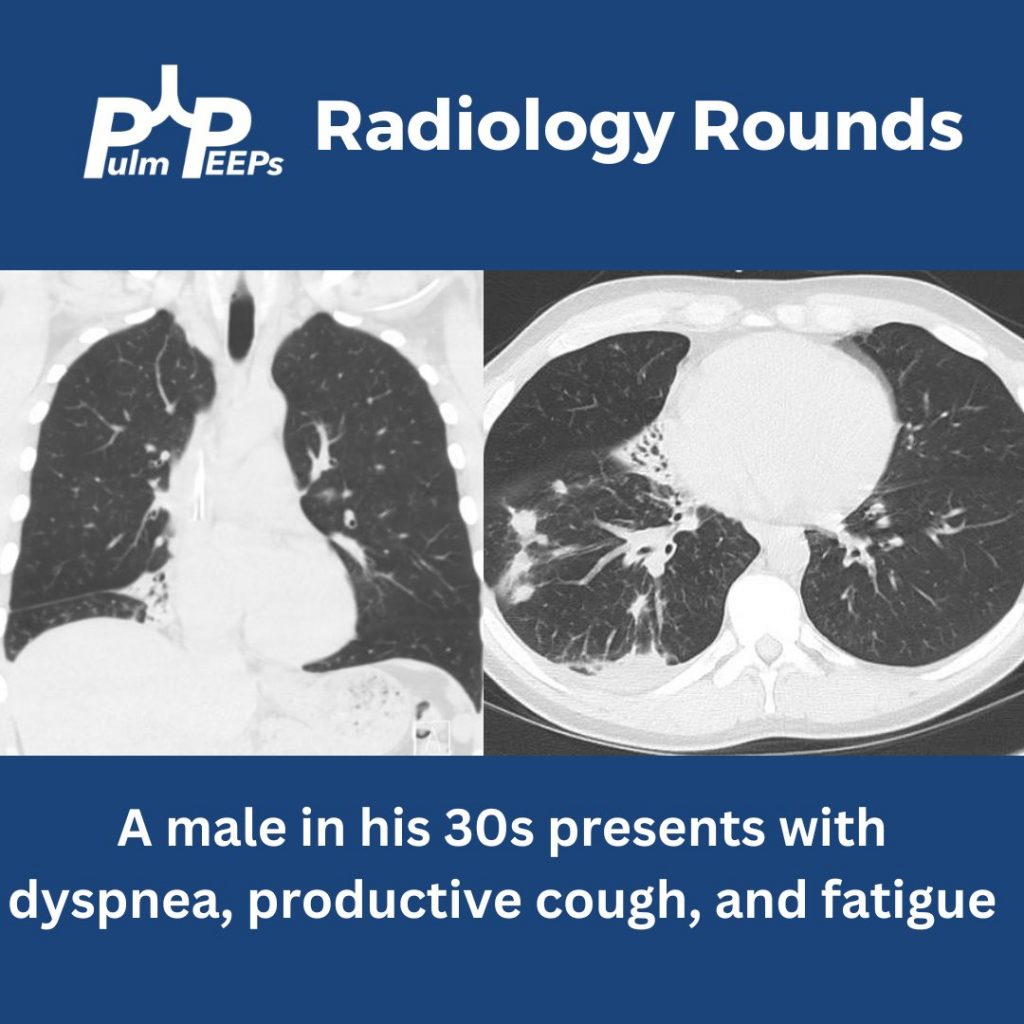
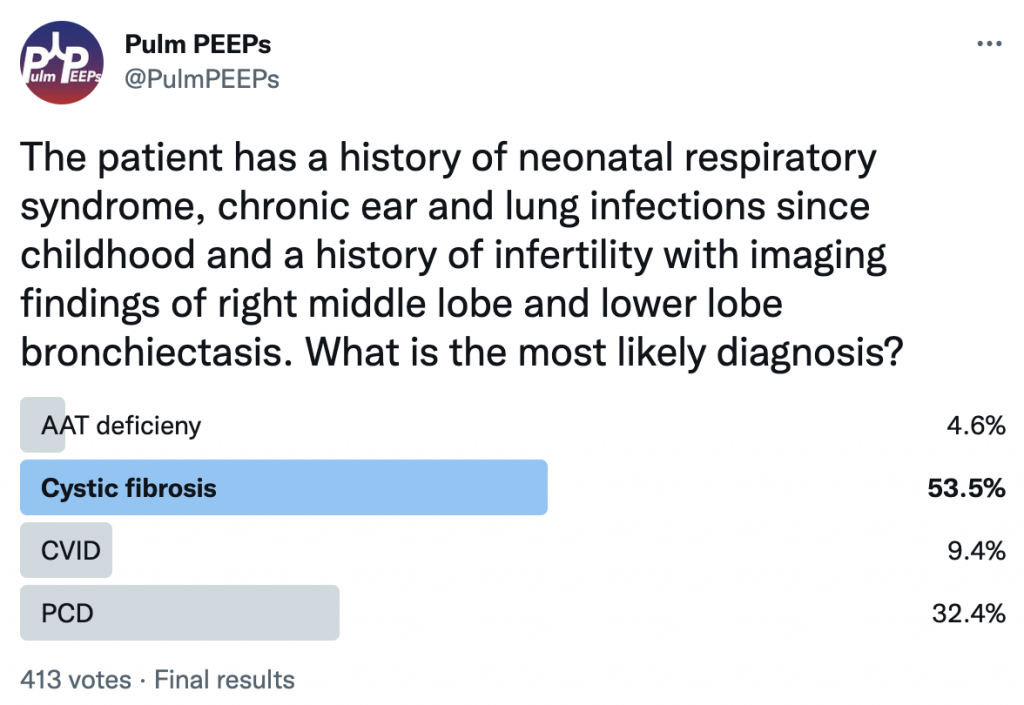
While chronic lung infections and infertility are overlapping symptoms for CF and Primary Ciliary Dyskinesia, the history of neonatal respiratory syndrome, ear infections and lower lobe bronchiectasis are most consistent with PCD
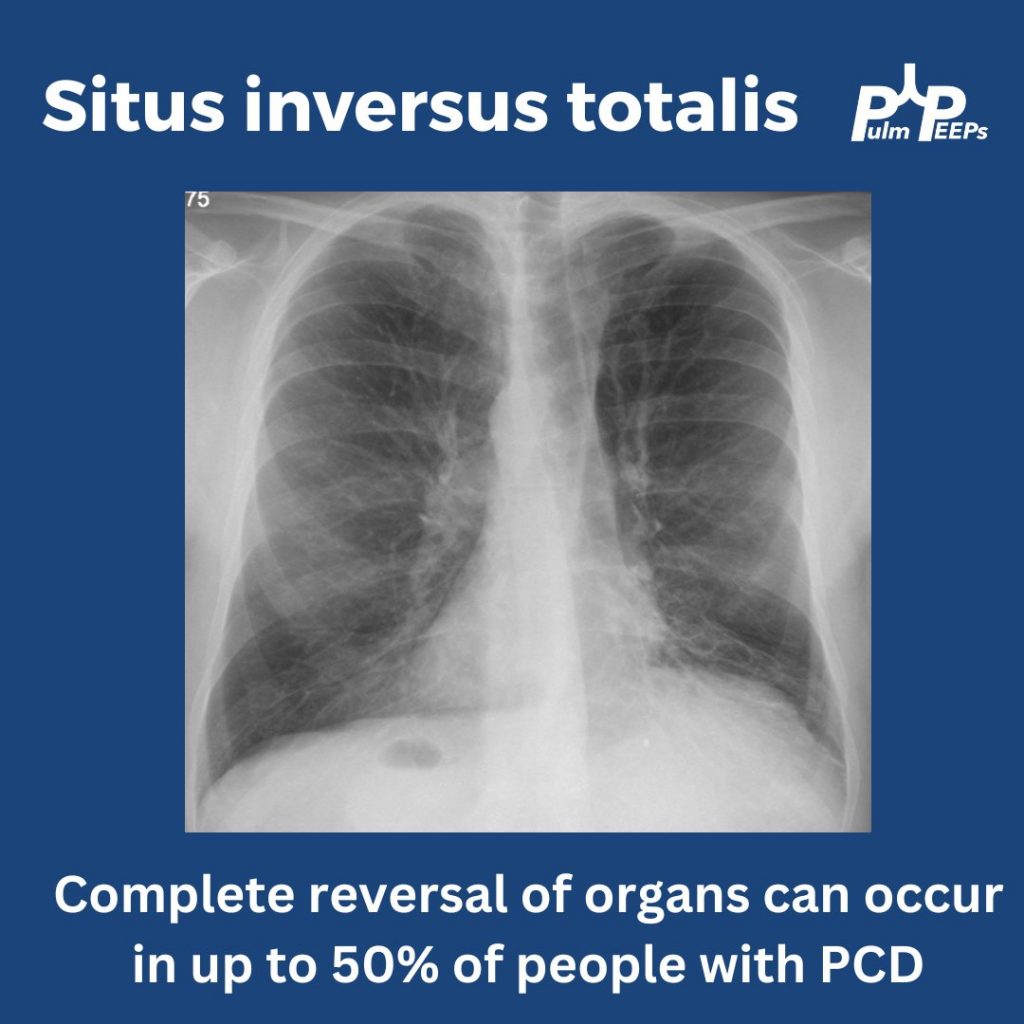
In up to 50% of people with PCD, you can get complete reversal of thoracic and abdominal organs. In this film you can see the heart in the right hemithorax, the gastric bubble on the right with the liver on the left resulting in elevation of the left hemidiaphragm
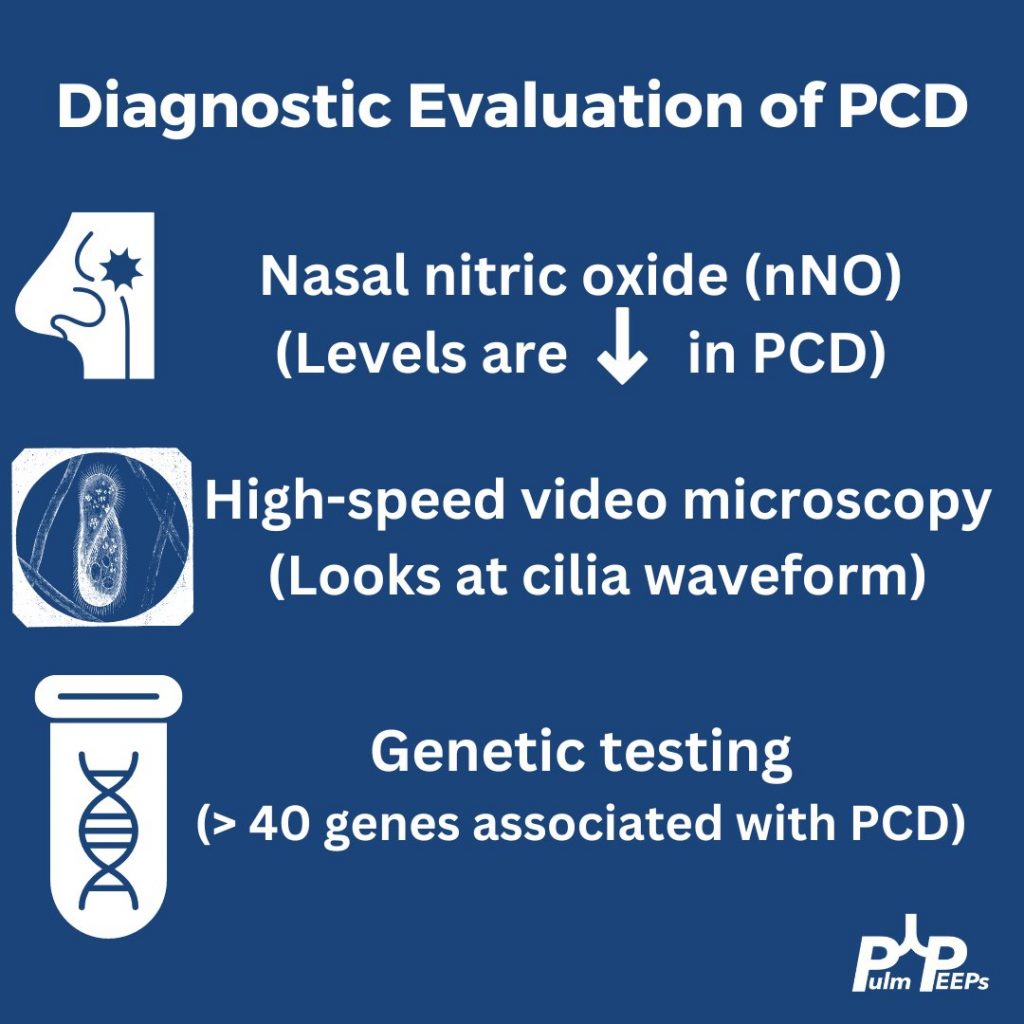
In patients with clinical symptoms and two decreased levels of nasal nitric oxide these findings suggest a PCD diagnosis but evaluation of the cilia structure and function as well as genetic testing are other diagnostic evaluations to confirm a diagnosis of PCD
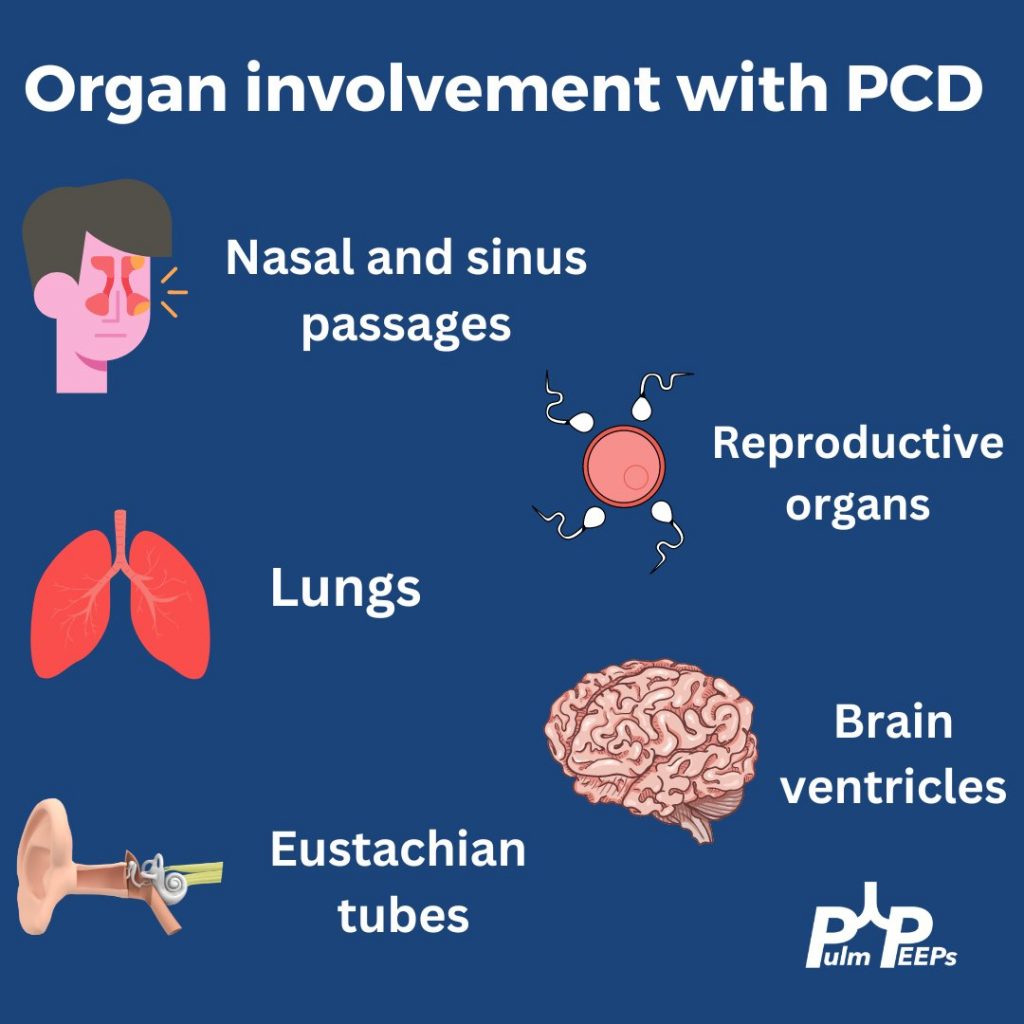
Primary ciliary dyskinesia is a autosomal recessive disorder that results in motile ciliary dysfunction and clinical manifestations can vary depending on which organs are involved
For the first Pulm PEEPs episode of 2023, we are starting off with a bang and a Roundtable discussion about venovenous extracorporeal membrane oxygenation (VV-ECMO). VV-ECMO has been increasing in use in the intensive care unit for patients with severe respiratory failure, especially during the COVID-19 pandemic. We are joined by experts in the field, Cara Agerstrand, Eddy Fan, and Nida Qadir, to discuss the basics of how ECMO works, physiologic goals, when to use ECMO for patients with ARDS, and much more. Let us know your thoughts and stay tuned for more great content in 2023.
Meet Our Guests
Cara Agerstrand is an Associate Professor of Medicine at Columbia University Irving Medical Center / NewYork-Presbyterian Hospital, where she is also the Director of the Medical ECMO Program. She is an international renown ECMO expert and is the current Conference Chair for the Extracorporeal Life Support Organization (or ELSO). Finally, she is a lauded educator and has received the American College of Chest Physicians Distinguished Educator Award.
Eddy Fan is an Associate Professor at the University of Toronto, and the University Health Network / Mount Sinai Hospital. He is also the Director of Critical Research and the Medical Director of the Extracorporeal Life Support Program. He has literally 100s of publications about ARDS, ECMO, and critical care, chairs the ELSO Research Committee, and spearheads multiple international collaborative studies.
Nida Qadir is an Associate Professor at the University of California Los Angeles and is an Associate Director of the MICU, as well as the co-director of the Post-ICU Recovery Clinic. Nida is also on the Critical Care Editorial Board for CHEST and is a highly regarded pulmonary and critical care educator.
Key Learning Points
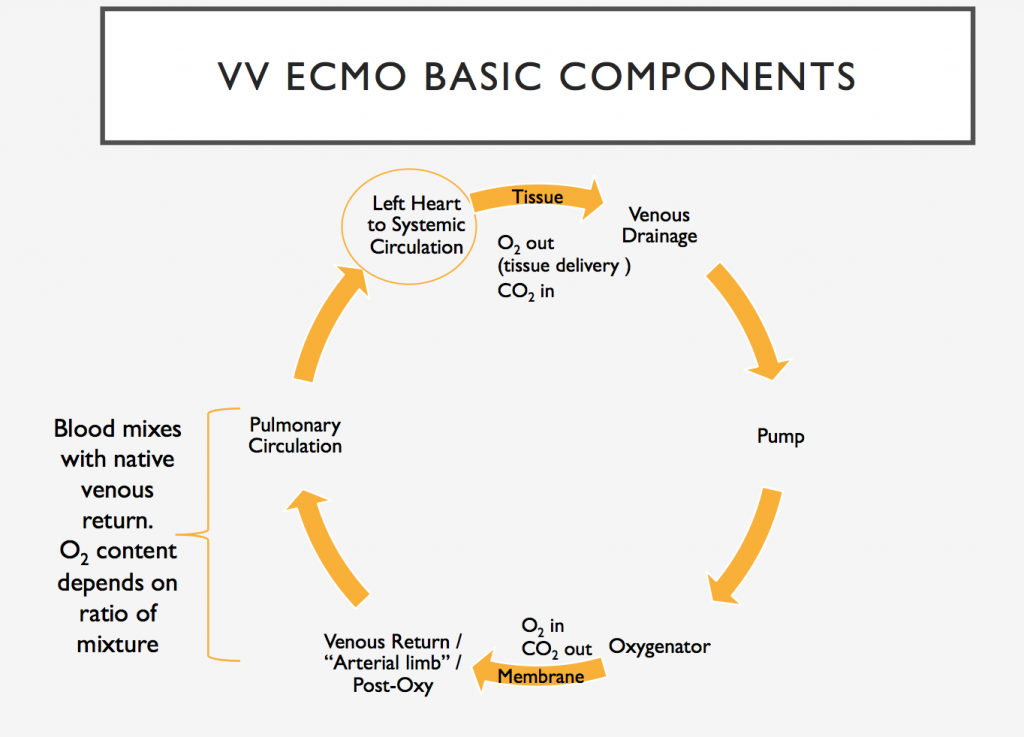
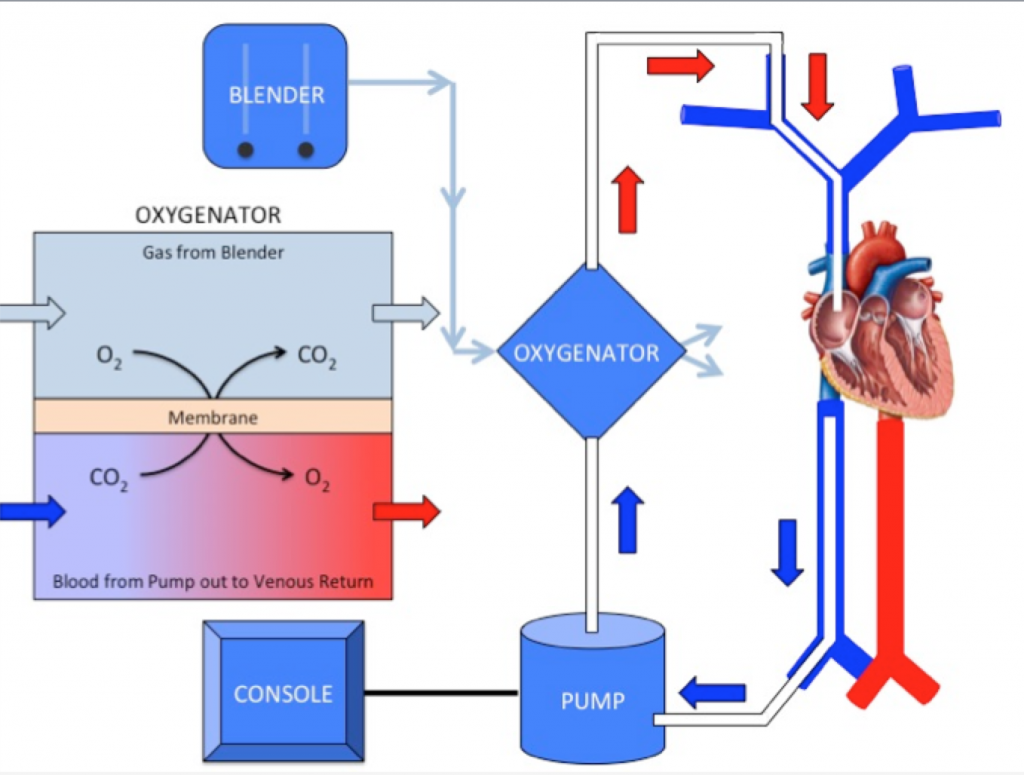
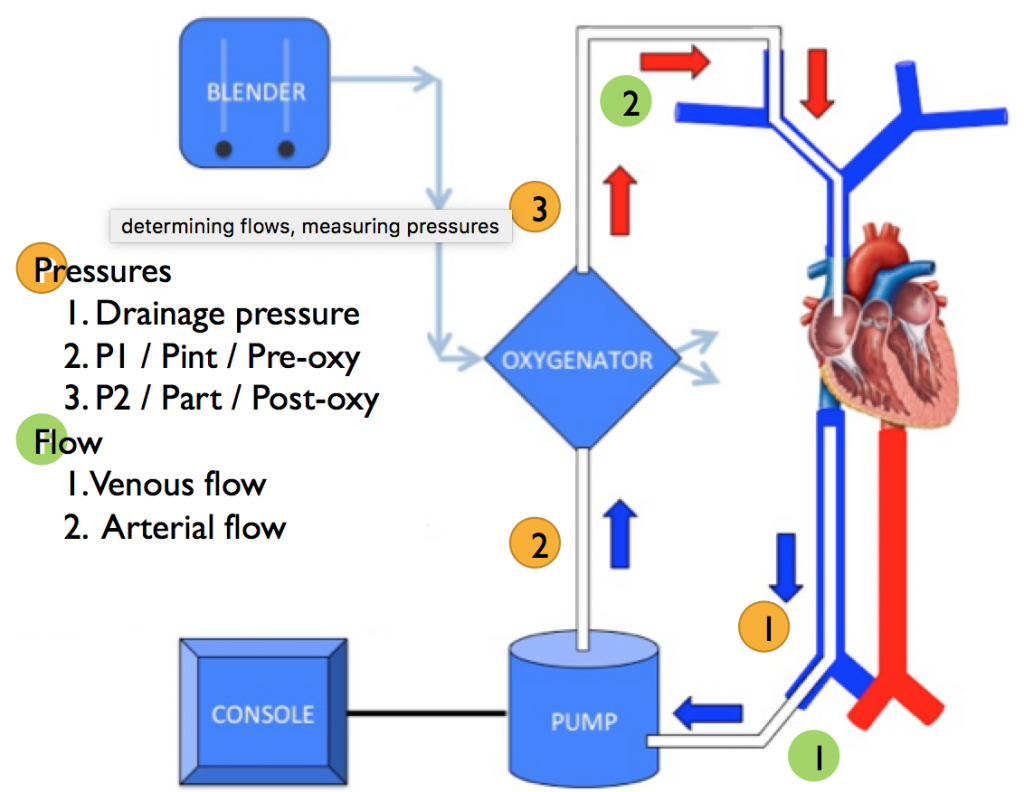
VV- ECMO Basic Components and Core Physiology
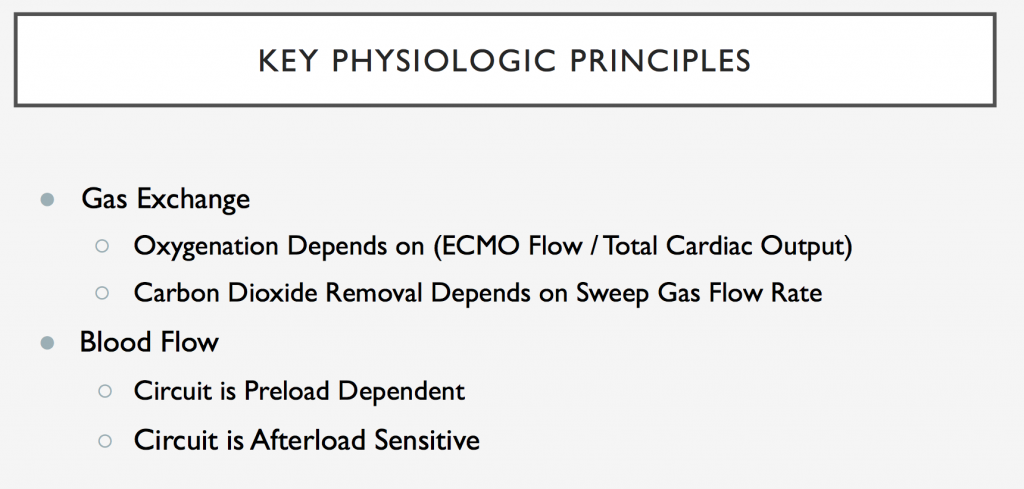
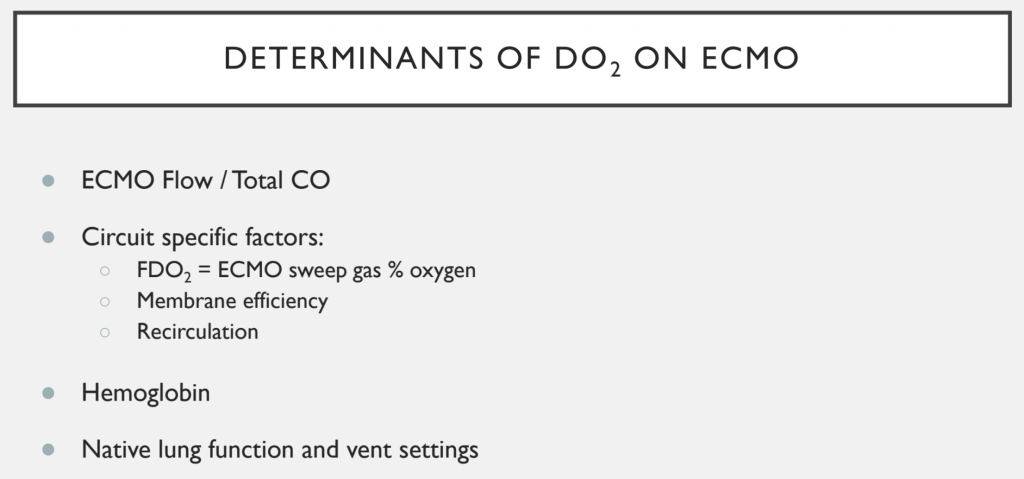
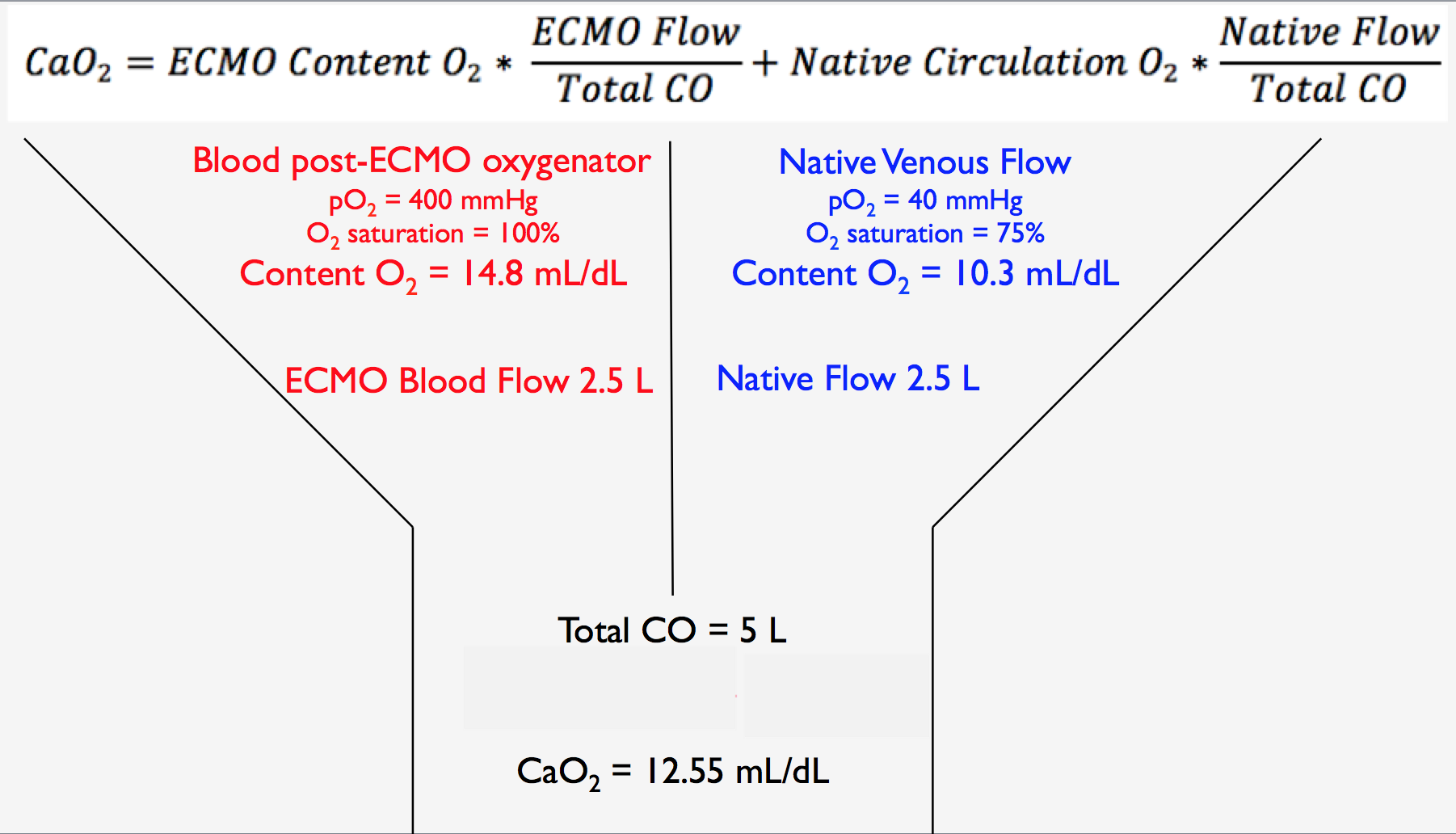
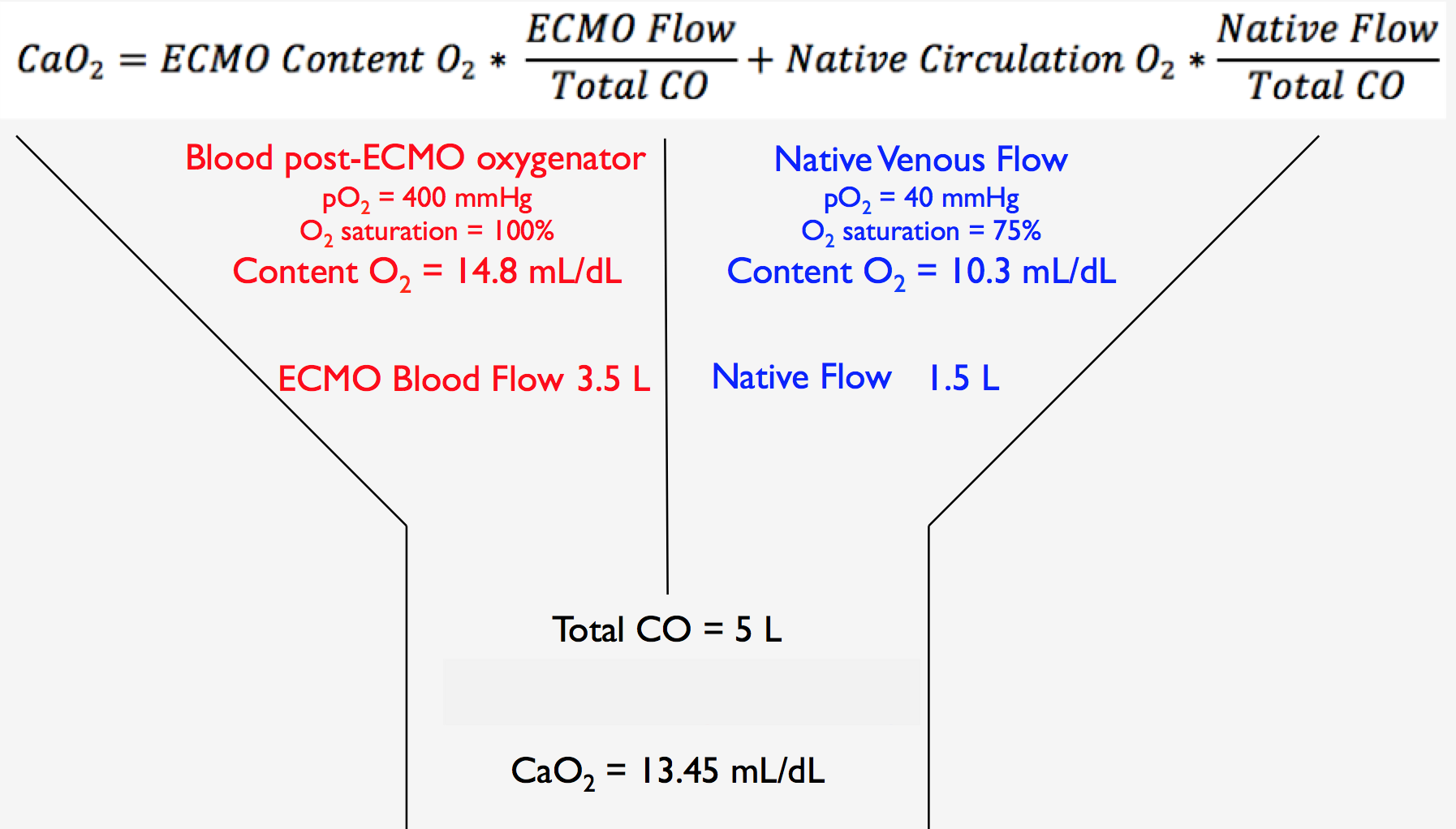
Oxygenation Delivery on VV-ECMO
ECMO Flow / Total CO = 0.5ECMO Flow / Total CO = 0.7
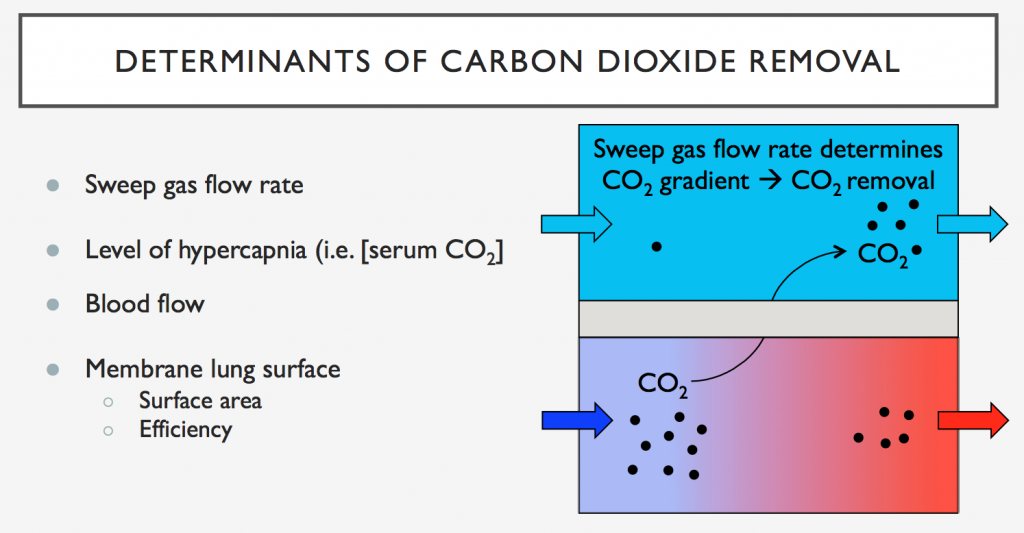
Carbon Dioxide Removal on VV-ECMO
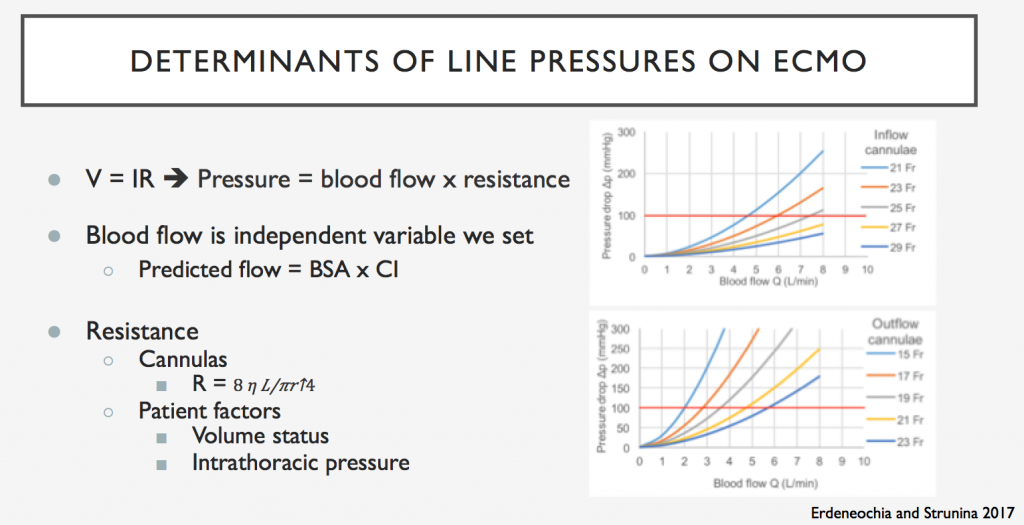
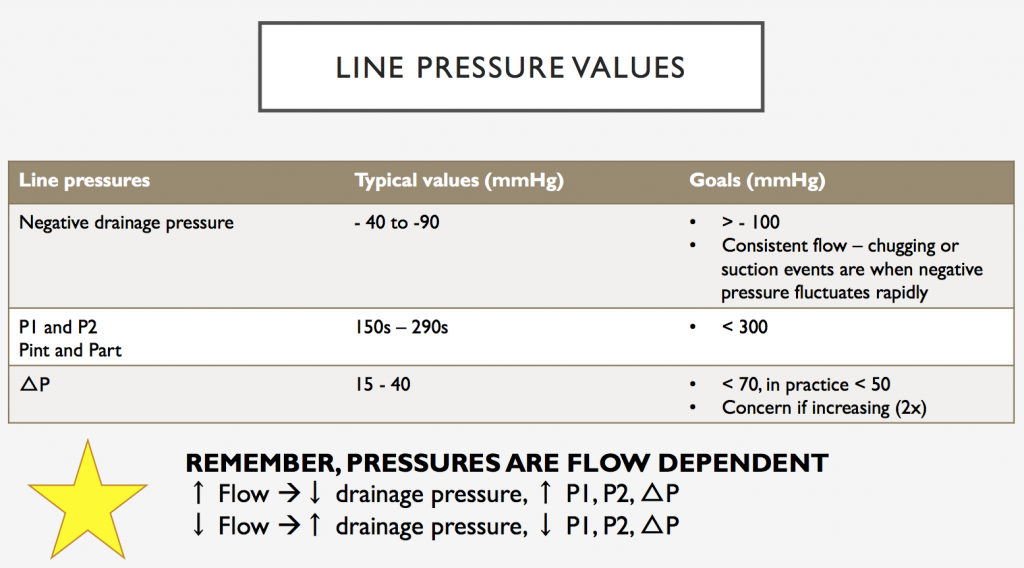
Flows and Line Pressures on VV-ECMO
ECMO for ARDS
Should be considered after conventional therapies have failed (including ventilator optimization and proning)
Allows for ultra-lung protective ventilation
Lung rest means settings that minimize ventilator-induced lung injury
EOLIA Trial (see below) shows that ECMO can be delivered safely, and likely has a benefit in severe ARDS, although the magnitude of that benefit remains uncertain. A Bayesian re-analysis showed a high likelihood of benefit even if skeptical of ECMO
ECMO For Bridge to Lung Transplant
Allows for patients to maintain gas exchange while awaiting transplant
Ideally done with patient extubated
Can allow for patients to maintain nutrition and mobility while awaiting transplant
Today we have a Pulm PEEPs special episode! Dave and Kristina chat post-call about their respective nights in the ICU. Hear about clinical reasoning on the fly, some crucial learning points, insights on procedural troubleshooting, and about the value of end-of-life discussions. The post-call brain fog and jokes only add to the learning fun!
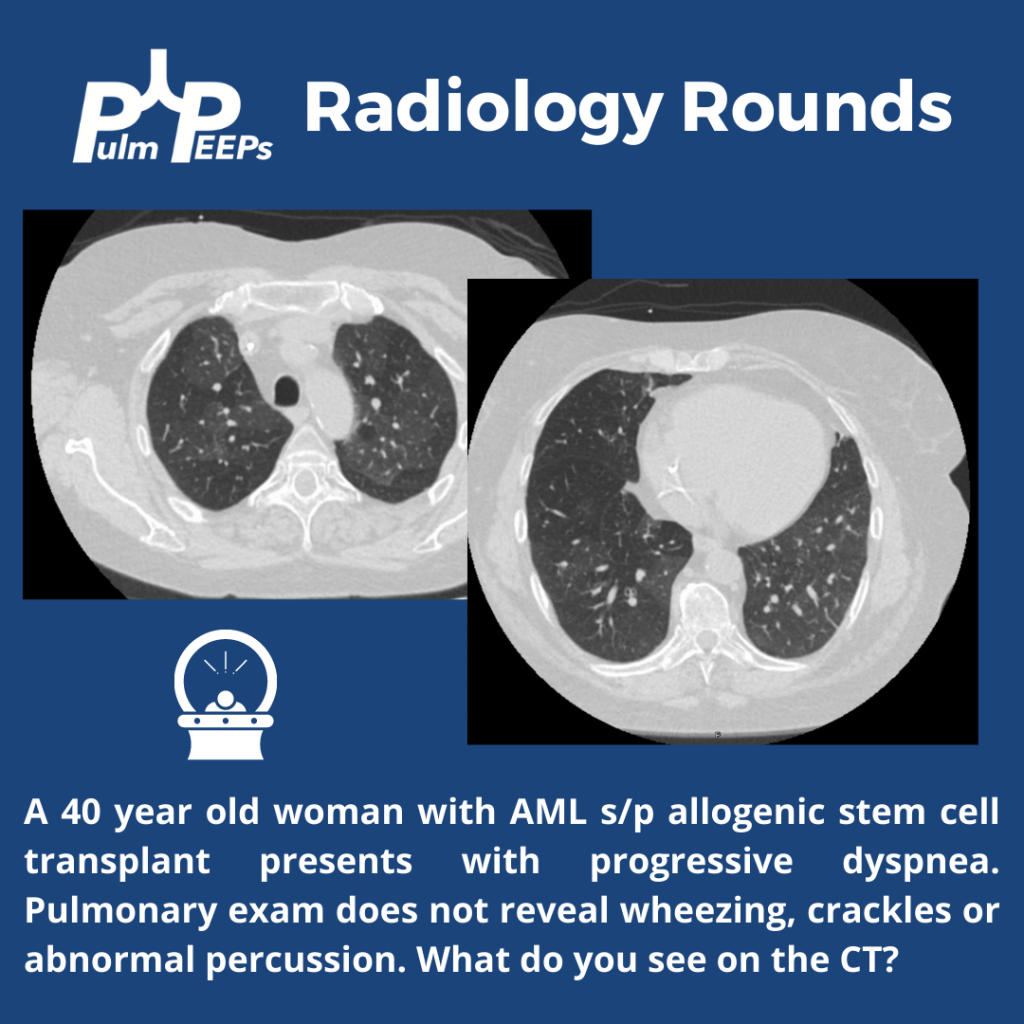
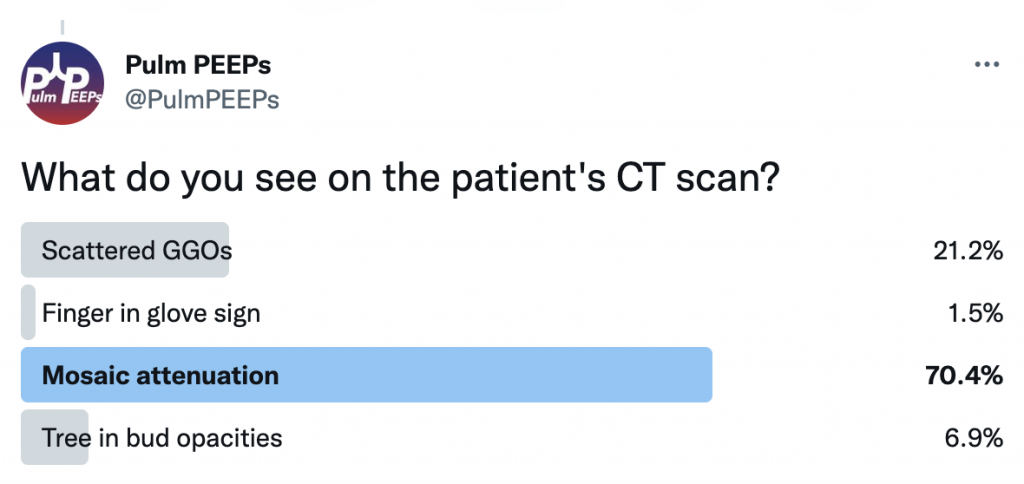
A 40-year-old patient s/p allogeneic stem cell transplant for AML 6 months prior presents with progressive dyspnea. The exam is unrevealing and imaging is obtained.
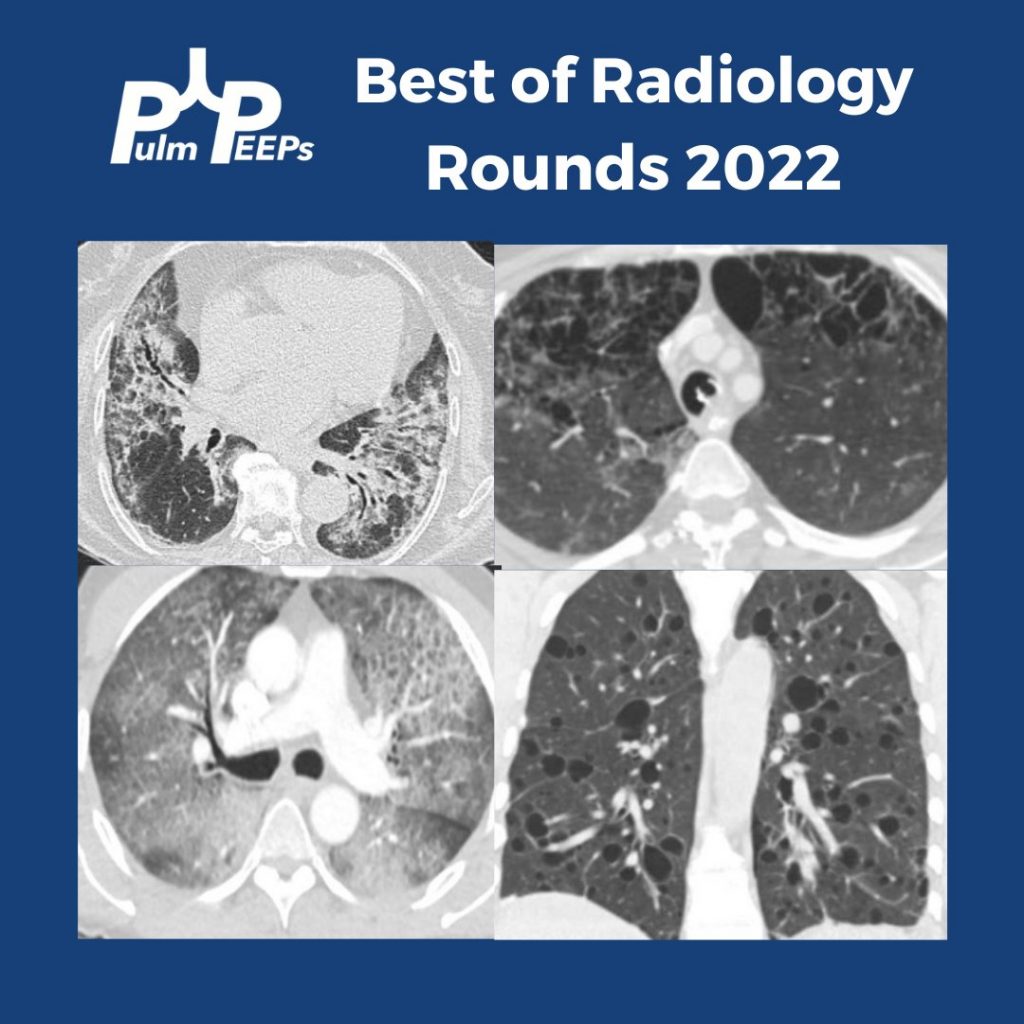
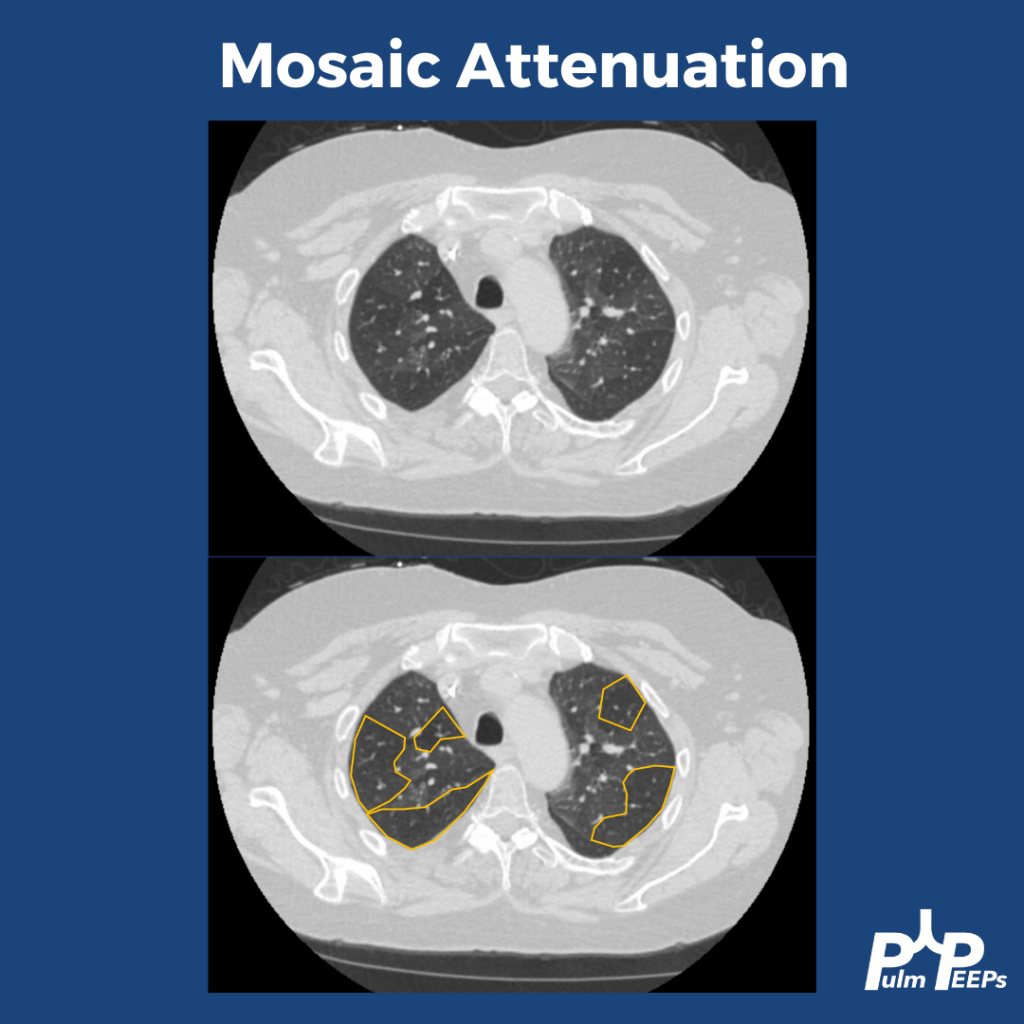
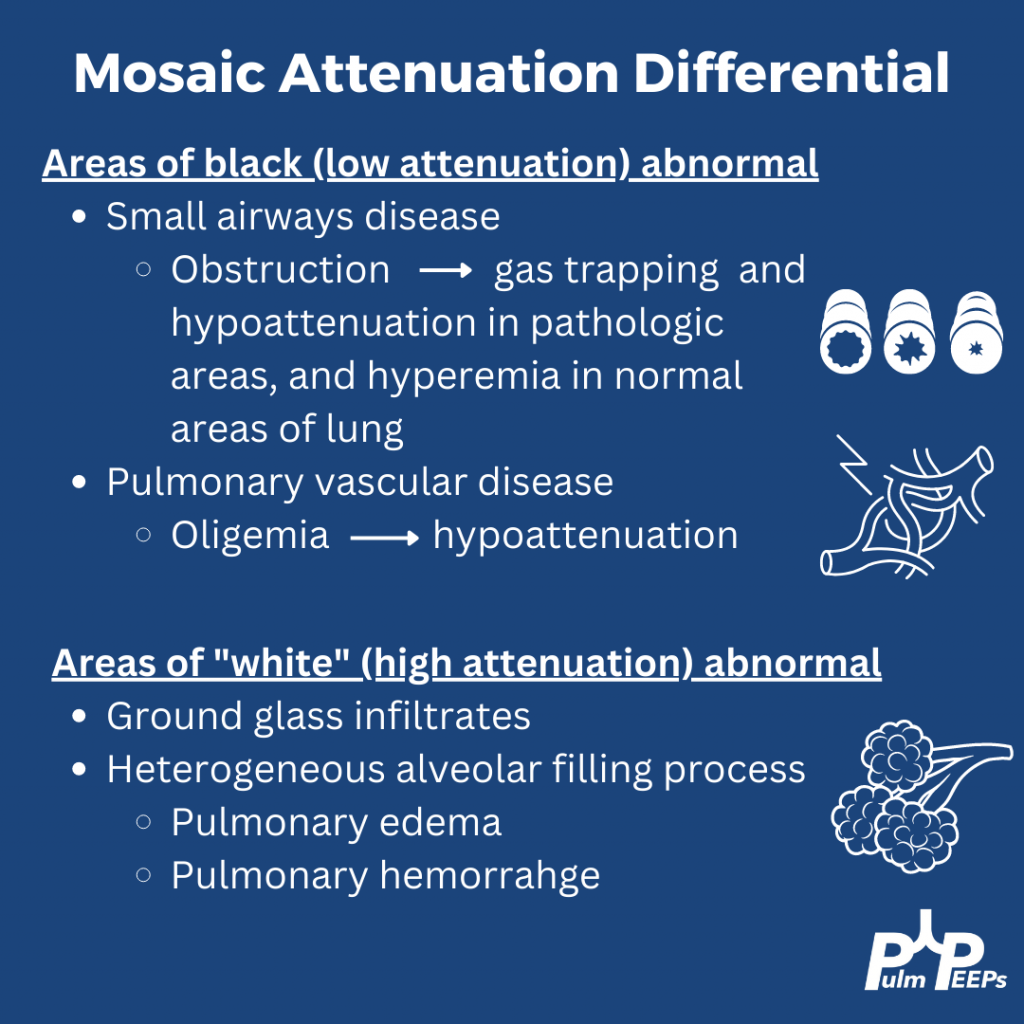
The patient’s CT reveals mosaic attenuation. Mosiac attenuation is a pattern of scattered regions of the lung with differing densities. The abnormal portions can be those that appear white or black.
Tip: Inspiratory and expiratory films can help identify the cause!
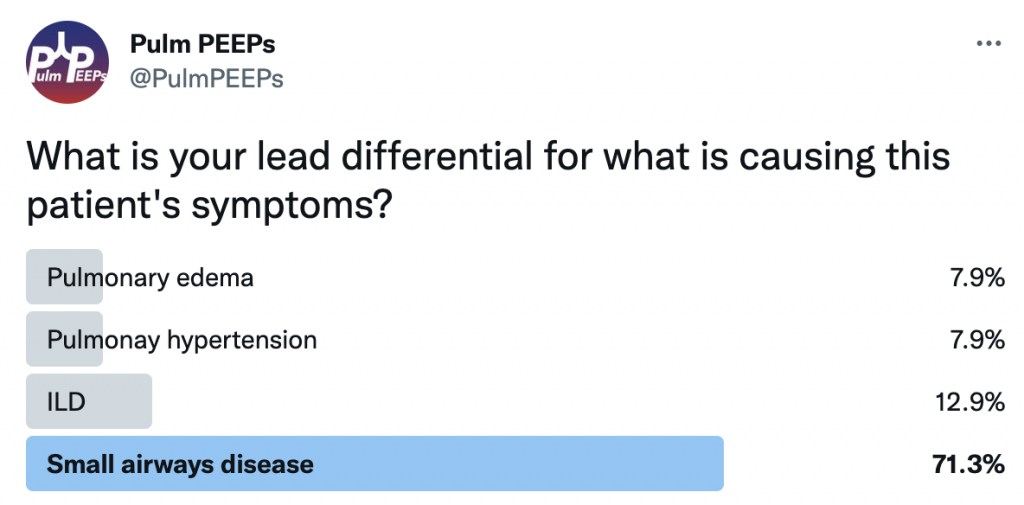
The patient had PFTs that showed severe obstruction, and significant change from PFTs prior to the stem cell transplant. Inspiratory and expiratory CT confirmed significant areas of gas trapping. She was diagnosed with bronchiolitis obliterans secondary to chronic GVHD
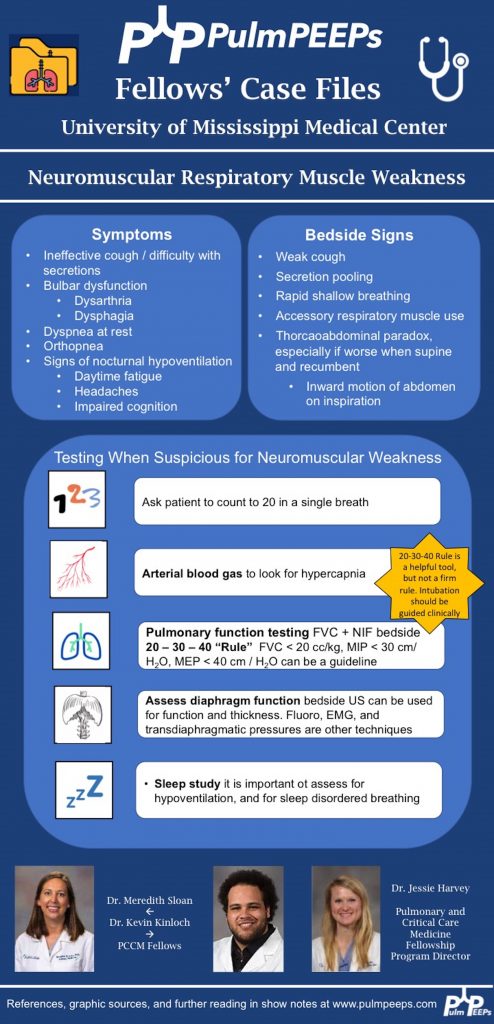
We’re excited to be back with another episode in our Pulm PEEPs Fellows’ Case Files series! This is a particularly exciting case since it is our first episode where some intrepid fellows reached out to us with an interesting case they had encountered. If you have a great case, please let us know and you can follow in their footsteps! Pack your bags, and let’s head to Mississippi to learn about another great pulmonary and critical care case.
Meet our Guests
Meredith Sloan is a pulmonary and critical care fellow at the University of Mississippi. She completed her medical school at the Medical University of South Carolina College of Medicine, and her residency at the University of Mississippi.
Kevin Kinloch is a senior fellow at the University of Mississippi Medical Center where he also completed his internal medicine residency. He completed medical school at Meharry Medical College.
Jessie Harvey is an Associate professor of Medicine at the University of Mississippi and is the Pulmonary and Critical Care Program Director. She is also the Director of the MICU, and has been at MMC since medical school. She is a dedicated educator and leads the POCUS curriculum for IM residents and PCCM fellows
Patient Presentation
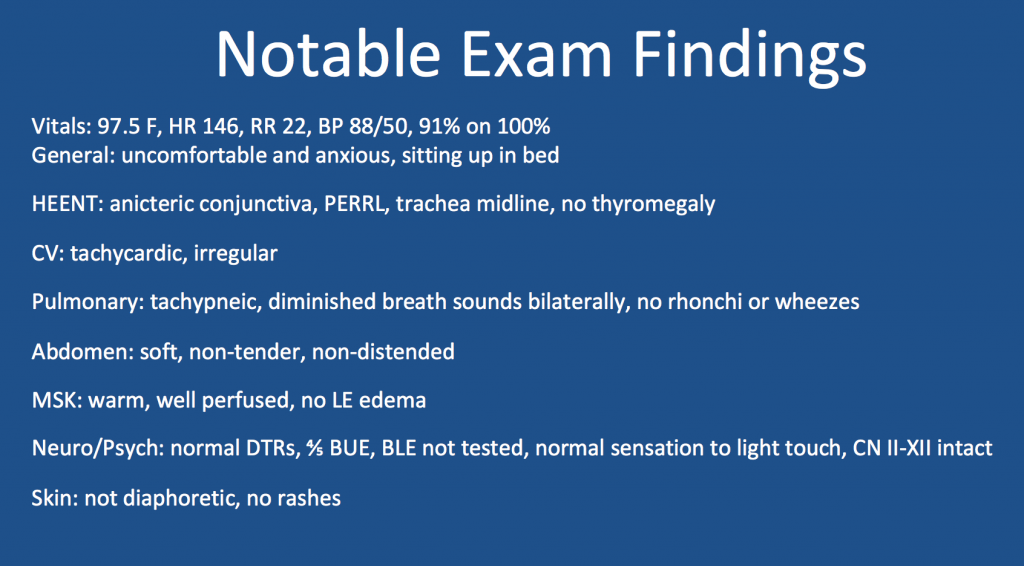
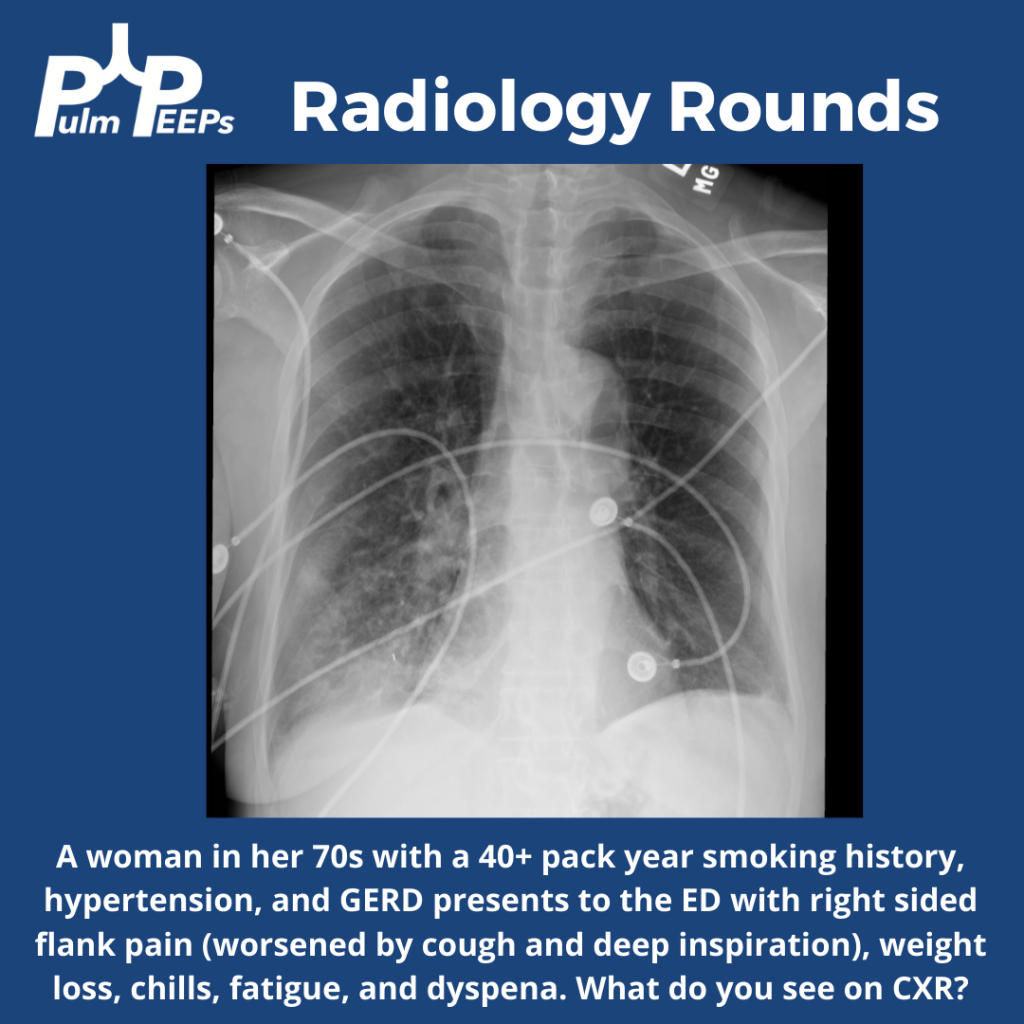
A 65-year-old man presented to the ED with worsening hemoptysis over the last several days after a recent lung biopsy. The patient is an active smoker with at least a 50-pack-year history, and he had been having a cough with small-volume hemoptysis. He ultimately had a chest CT that revealed a large LUL mass (10.3 x 6.4 cm). Given this suspicious mass, three days prior to his ED presentation, he was taken for bronchoscopy with BAL, transbronchial biopsies, endobronchial biopsy, EBUS guided TBNA of 11L, along with TBNA, brushing and radial EBUS TBNA of his left upper lobe mass.
Key Learning Points
**Spoilers Ahead** If you want to think through the case on your own we advise listening to the episode first before looking at these points.
Staging procedures for masses
Enough tissue so we can make a diagnosis and do molecular testing
Highest staging when getting your biopsy
POCUS for respiratory failure
Absence of lung slidings
Especially post procedure
The presence of a new pleural effusion after a procedure could indicate hemothorax
Hematocrit sign – an echogenic layering of material in an effusion
New B-lines, especially if prior there were only A-lines
Cardiogenic or non-cardiogenic pulmonary edema, alveolar hemorrhage, or infection
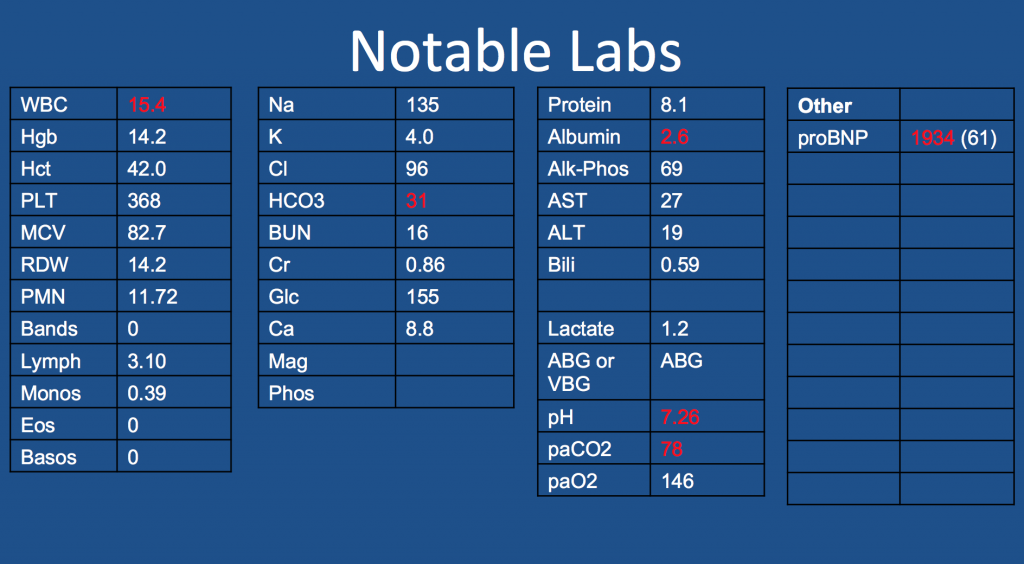
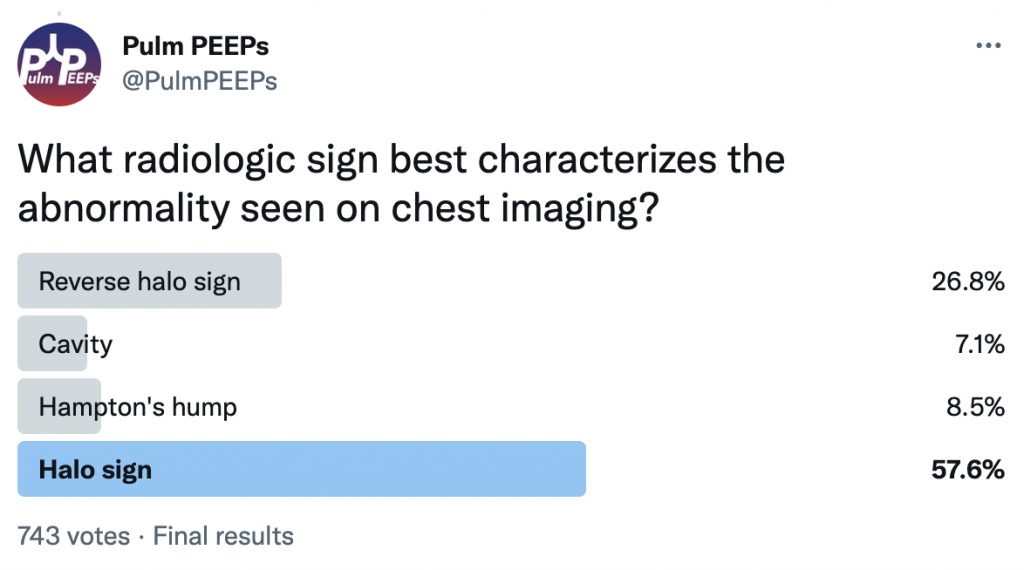
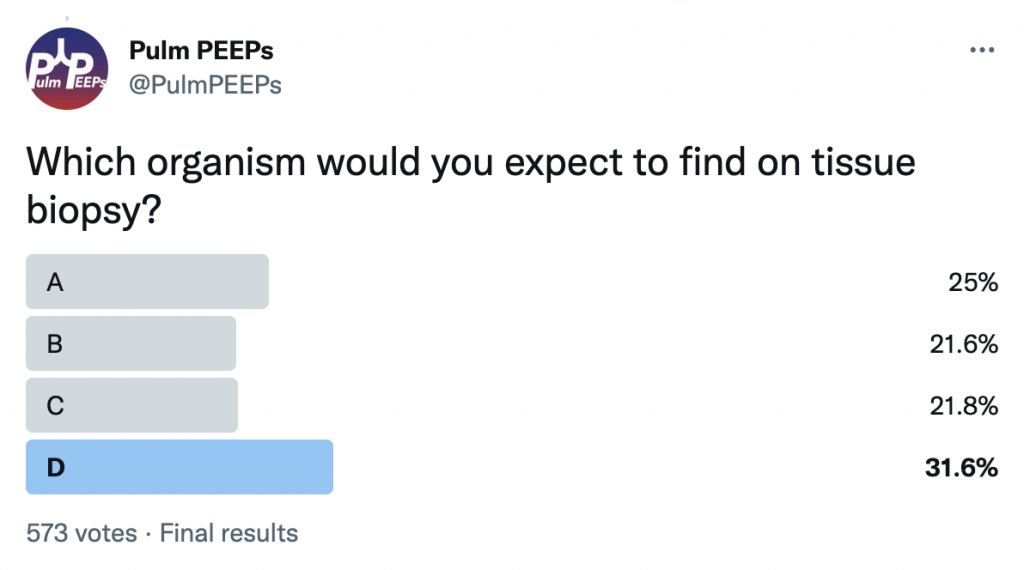
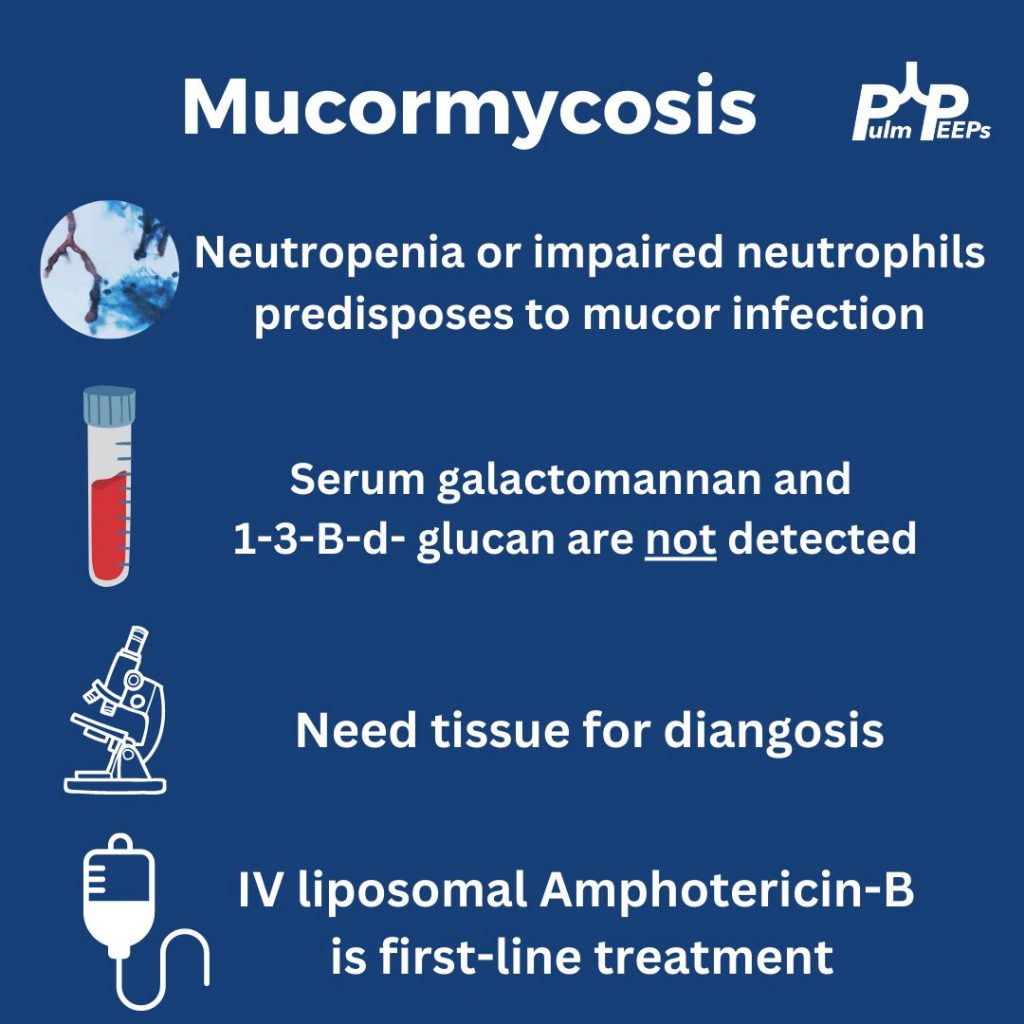
A middle-aged male presents with sub-acute fatigue, fevers and dyspnea on exertion. His admission labs are notable for severe neutropenia (ANC < 500)
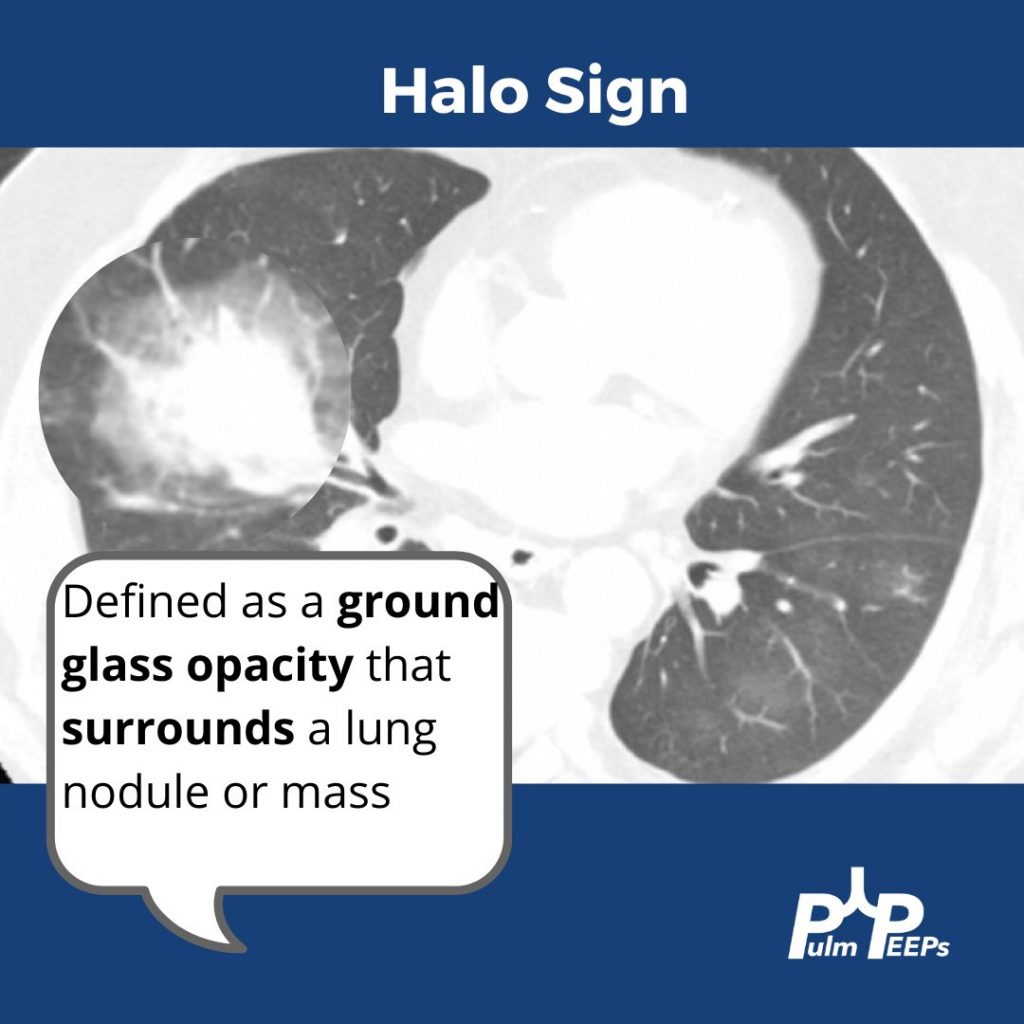
This patient has evidence of a halo sign which represents local vessel invasion or hemorrhage
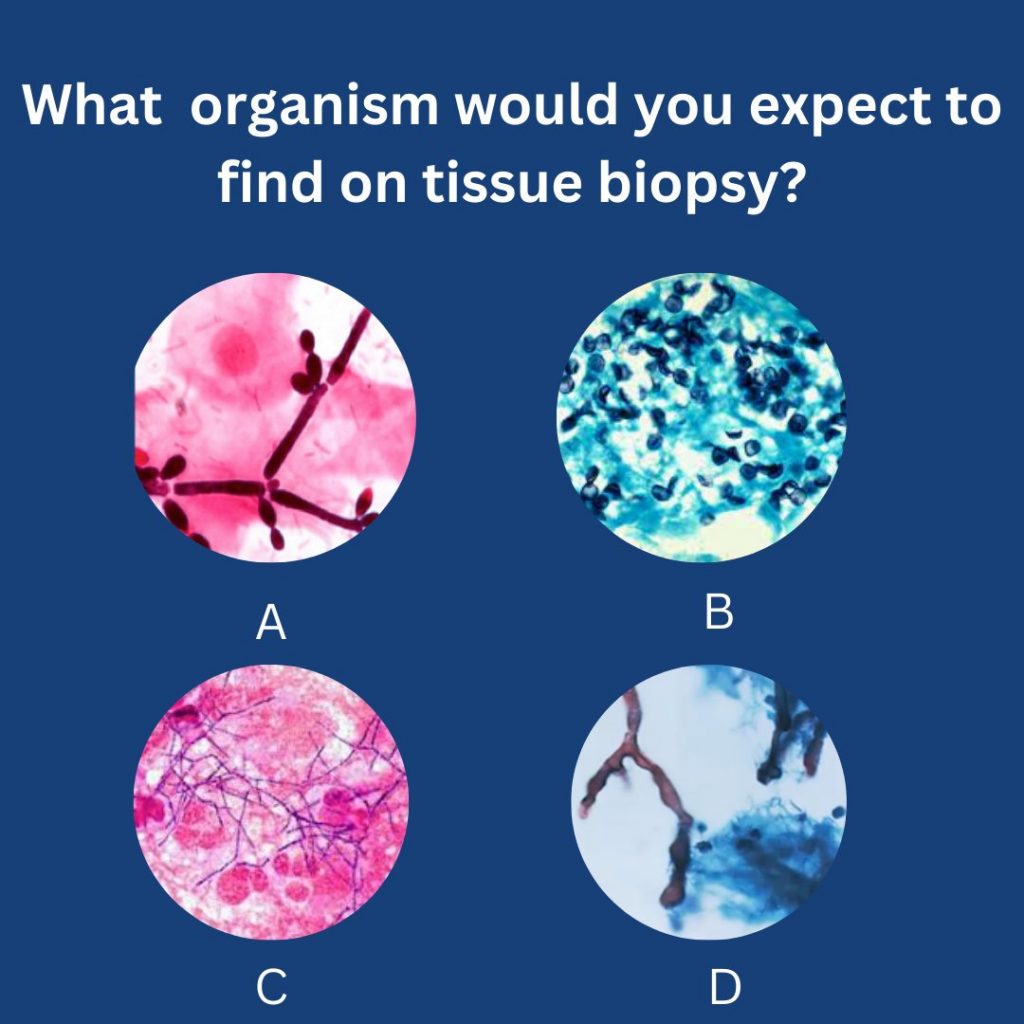
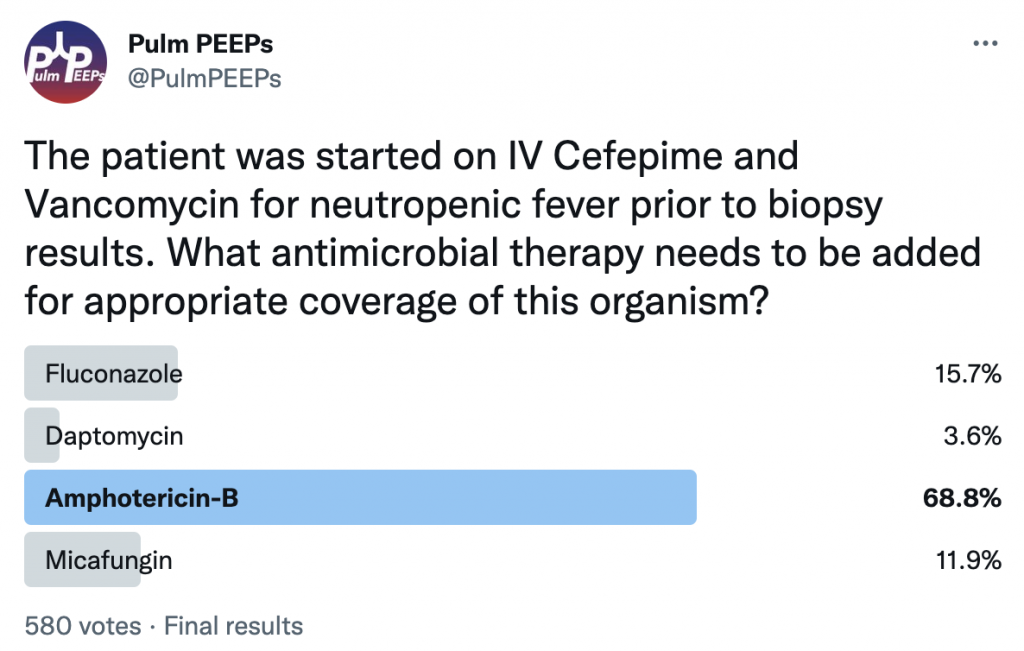
The patient undergoes evaluation. RVP, sputum culture and serum galactomannan and 1-3-B-d-glucan are negative. A BAL with transbronchial biopsies are obtained.
The patient was found to have pulmonary mucormycosis and was started on IV liposomal amphotericin-B.
This week on Pulm PEEPs, Dave and Kristina are joined by Jason Maley and Ann Parker, two pulmonary and critical care physicians who are leaders in treating patients with Long COVID, or Post-Acute Sequelae of SARS-CoV-2. Both of them help run the Long COVID clinics at their respective institutions and are part of broader consortiums dedicated to patient care. They also both participate in research to improve outcomes for patients with Long COVID and Post-Intensive Care Syndrome. In this conversation, we cover the diagnosis of Long COVID, common symptoms, abnormal test findings, possible mechanisms of disease, the impacts of variants and vaccines, treatments, and the natural history of this condition. We hope this will be helpful for providers, patients, and family members.
Meet Our Guests
Jason Maley is an Assistant Professor of Medicine at Beth Israel Deaconess Medical Center and Harvard Medical School. He is the Director of the BIDMC Critical Illness and COVID-19 Survivorship Program, and the Co-Chair of the American Academy of Physical Medicine and Rehabilitation Postacute Sequeleae of SARS-CoV-2 infection (PASC) initiative. He is NIH funded to study post-COVID patients.
Ann Parker is an Assistant Professor of Medicine at Johns Hopkins and is the Co-Director of the Johns Hopkins Post-Acute COVID-19 team. She is NIH funded with her research focusing on survivors of respiratory failure and critical illness.
Key Learning Points
Long COVID or Post-Acute Sequelae of SARS-CoV-2 or Post-COVID condition
Long COVID was first described this way by patients so this is the common nomenclature that is used. It is also referred to as Post-Acute Sequelae of SARS-CoV-2 or Post-COVID condition
Defined by patients that have not returned to their baseline health 3 months after their acute episode of COVID-19
Major organizations in describing this disease and doing research are:
World Health Organization
Multiple patient-led organizations
CDC – INSPIRE
NIH – RECOVER
Post-COVID Clinic
Seeing patients across the spectrum of illness. Not all patients had to be critically ill or hospitalized
The standard patient has changed over time and now the vast majority had a mild initial illness, but afterward had unusual and persistent symptoms
Patients are generally referred by their PCP or self-referred
The criteria for being seen in clinic are very loose to make sure patients are not excluded
Many patients do not have a confirmed case of COVID since patients early in the pandemic often did not have a positive test available, and now many people are testing positive at home
Initial records review to make sure that can help patients
Standardized questionnaires
Screening for physical impairment, mental health impairment, and cognitive impairment
Rehabilitation and multi-disciplinary based approach
It is extremely important to be aware of the bias in patient populations in Post-COVID clinics
The population that can make it to clinic may not, and does not, represent all patients who have had COVID or have Long COVID. Patients may be limited in their ability to get to clinic based on their physical condition, financial resources, location, support, and language barriers.
Overlap of Long COVID and PICS
These conditions are very similar and certainly have a lot of overlap
For patients coming out of the ICU, screening should start with looking for known PICS symptoms.
These domains are mental health, physical impairment, and cognitive function
There may be some unique aspects, such as:
Severe persistent fatigue
Extreme changes in taste and smell
Common symptoms
Many symptoms are complex and multifactorial
Neuropsycholgoicl impairment – termed “brain fog”
Difficulty with concentration, and cognition
Anxiety
Depression
Persistent shortness of breath
Dyspnea can be reported even with just talking for long periods of time
“Deep breaths are just not satisfying”
Cough
Chest pain
Dysautonomia
Palpitations, dizziness, orthostasis
Fatigue
Post-exertional malaise
Cognitive blunting or “brain fog”
Changes in sleep
Headaches
Common findings on testing in patients with Long COVID
Shortness of breath
Some may have impaired diffusion (low DLCO) on PFTs
However, often patients have normal or near-normal PFTs
10 – 20 % have air trapping on inspiratory/expiratory chest CTs that could indicate bronchiolitis
One study showed that CPETs showed impaired oxygen extraction
Preserved cardiac output to exercise and no evidence of deconditioning
This study indicated an issue at the peripheral level (ex: vascular, mitochondrial) with oxygen extraction.
Variants
It is very difficult to say if variants differ in rates of Long COVID given that often patients do not get sequencing to know the variant and because there is overlap in the timing of variants
Further testing will continue on this going forward
Vaccines
Reduced risk of Long COVID with vaccination
Boosting further decreases the risk compared to just the initial vaccination
There is a variable response to getting vaccinated if a patient has Long COVID
Most patients tolerate it well and some patients have relief of symptoms
There are some patients who can develop worsened Long COVID symptoms
References and further reading
Chippa V, Aleem A, Anjum F. Post Acute Coronavirus (COVID-19) Syndrome. In: StatPearls. StatPearls Publishing; 2022. Accessed November 14, 2022. http://www.ncbi.nlm.nih.gov/books/NBK570608/
Crook H, Raza S, Nowell J, Young M, Edison P. Long covid—mechanisms, risk factors, and management. BMJ. 2021;374:n1648. doi:10.1136/bmj.n1648
Durstenfeld MS, Sun K, Tahir P, et al. Use of Cardiopulmonary Exercise Testing to Evaluate Long COVID-19 Symptoms in Adults: A Systematic Review and Meta-analysis. JAMA Network Open. 2022;5(10):e2236057. doi:10.1001/jamanetworkopen.2022.36057
Nalbandian A, Sehgal K, Gupta A, et al. Post-acute COVID-19 syndrome. Nat Med. 2021;27(4):601-615. doi:10.1038/s41591-021-01283-z
Soriano JB, Murthy S, Marshall JC, Relan P, Diaz JV. A clinical case definition of post-COVID-19 condition by a Delphi consensus. Lancet Infect Dis. 2022;22(4):e102-e107. doi:10.1016/S1473-3099(21)00703-9
Sudre CH, Murray B, Varsavsky T, et al. Attributes and predictors of long COVID. Nat Med. 2021;27(4):626-631. doi:10.1038/s41591-021-01292-y
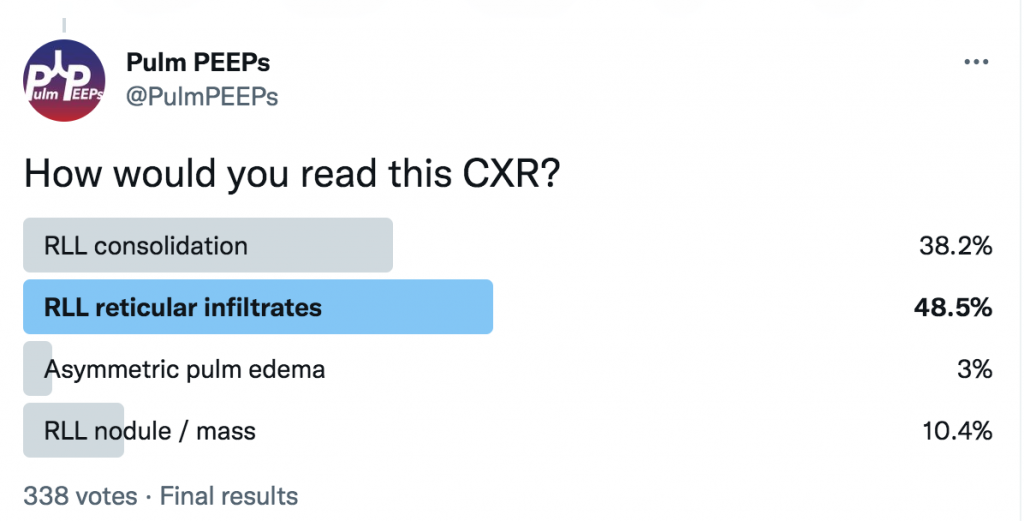
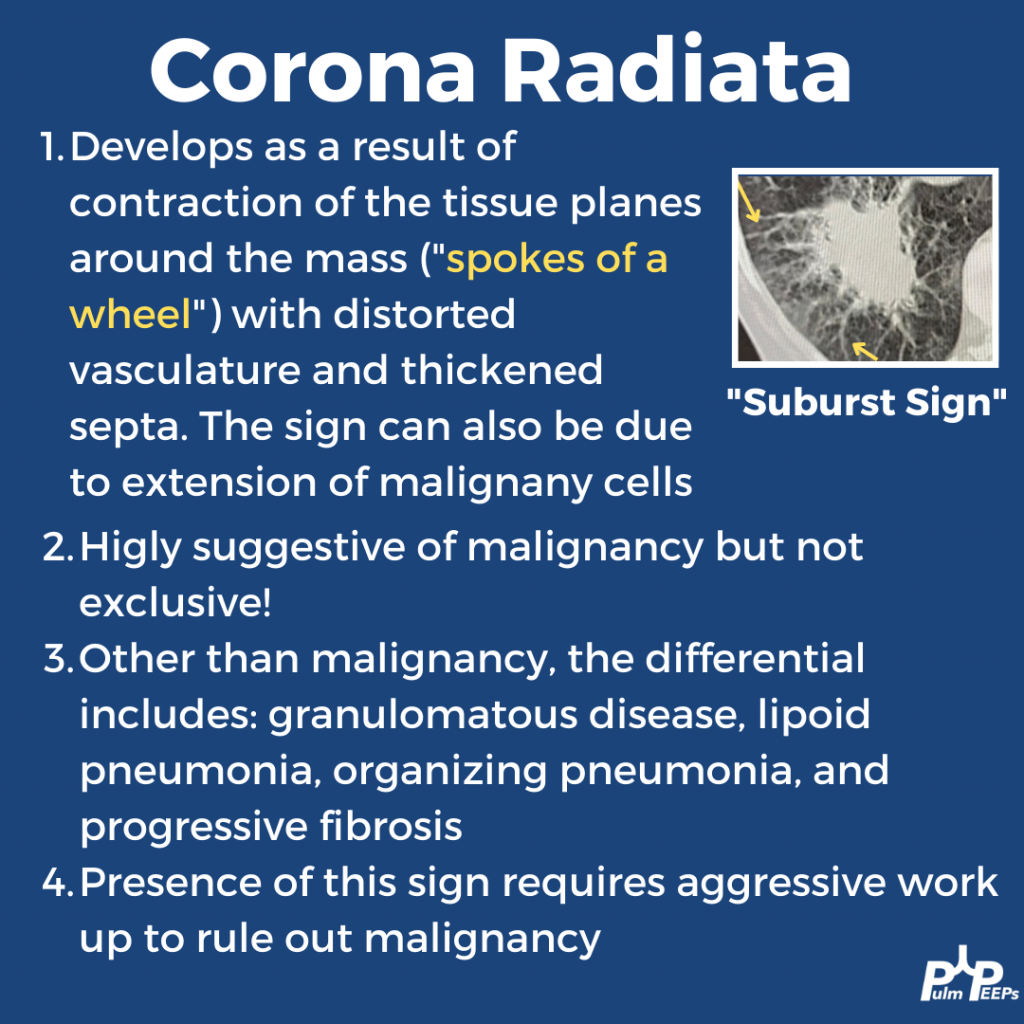
This week’s #RadiologyRounds is brought to you by our newest contributor, Nick Ghionni! We’ll dive into a classic Radiology Sign and talk about what it represents, and how it helps inform your differential.
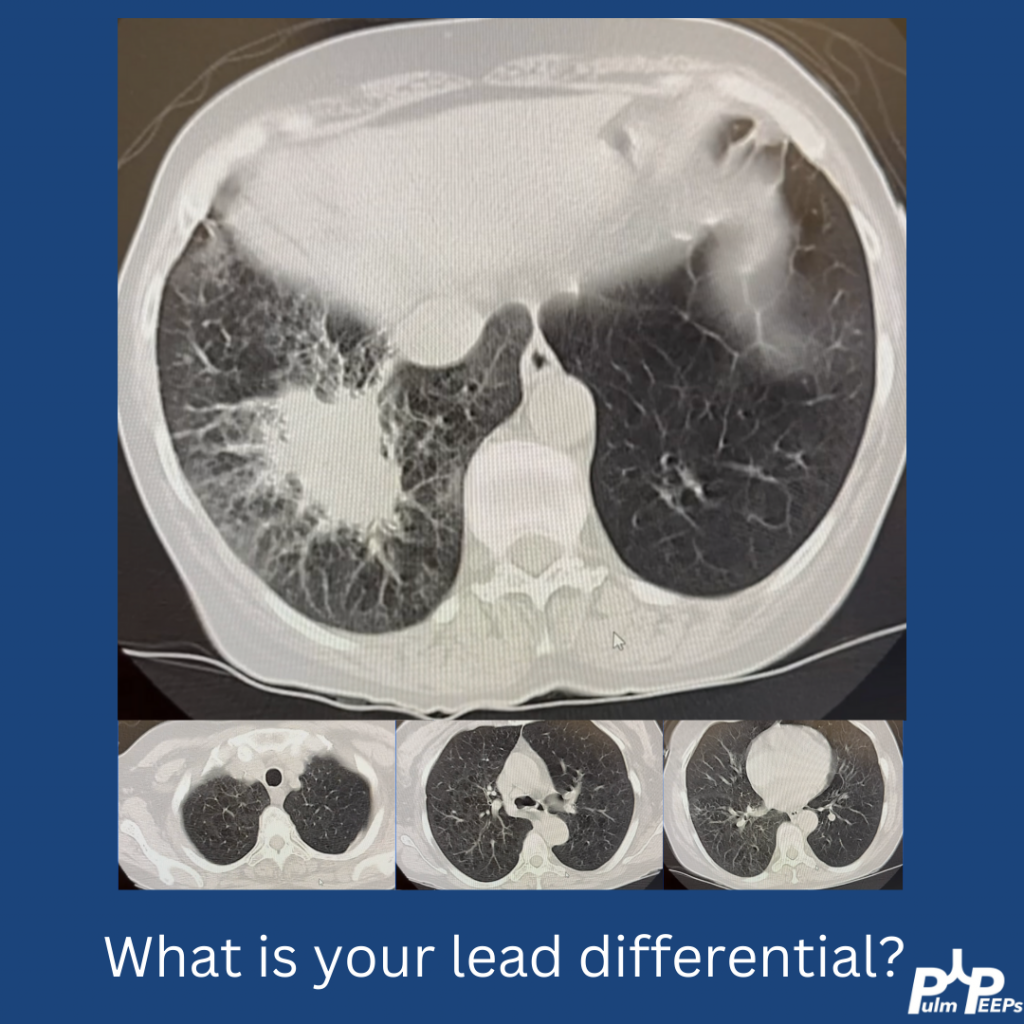
In this case, the patient underwent a biopsy that showed no malignancy but grew NTM! Given that NTM can be superimposed on malignancy, repeated biopsies were done that corroborated. She is being treated with close monitoring.
Welcome back to our Pulm PEEPs Fellows’ Case Files series! We are joined this week by a fellow and the program director from the Harvard combined PCCM fellowship at Massachusettes General Hospital and Beth Israel Deaconess Medical Center. Listen in for a great learning case and let us know on Twitter, if you have a great case to share!
Meet our Guests
Brian Rosenberg is a third year fellow at the Harvard MGH/BI program. He completed his undergraduate degree at Harvard, received his MD from Yale where he also got a PhD in cell biology, and then did his internal medicine residency at Columbia University Medical Center in NYC.
Asha is an Assistant Professor Medicine at Beth Israel Deaconess Medical Center and Harvard Medical School, and is the Program Director of the Harvard MGH/BI combined fellowship. She is also the Director of the Pulmonary Consult Service at BIDMC, was a Rabkin Fellow in Medical Education and has received multiple leadership and teaching awards