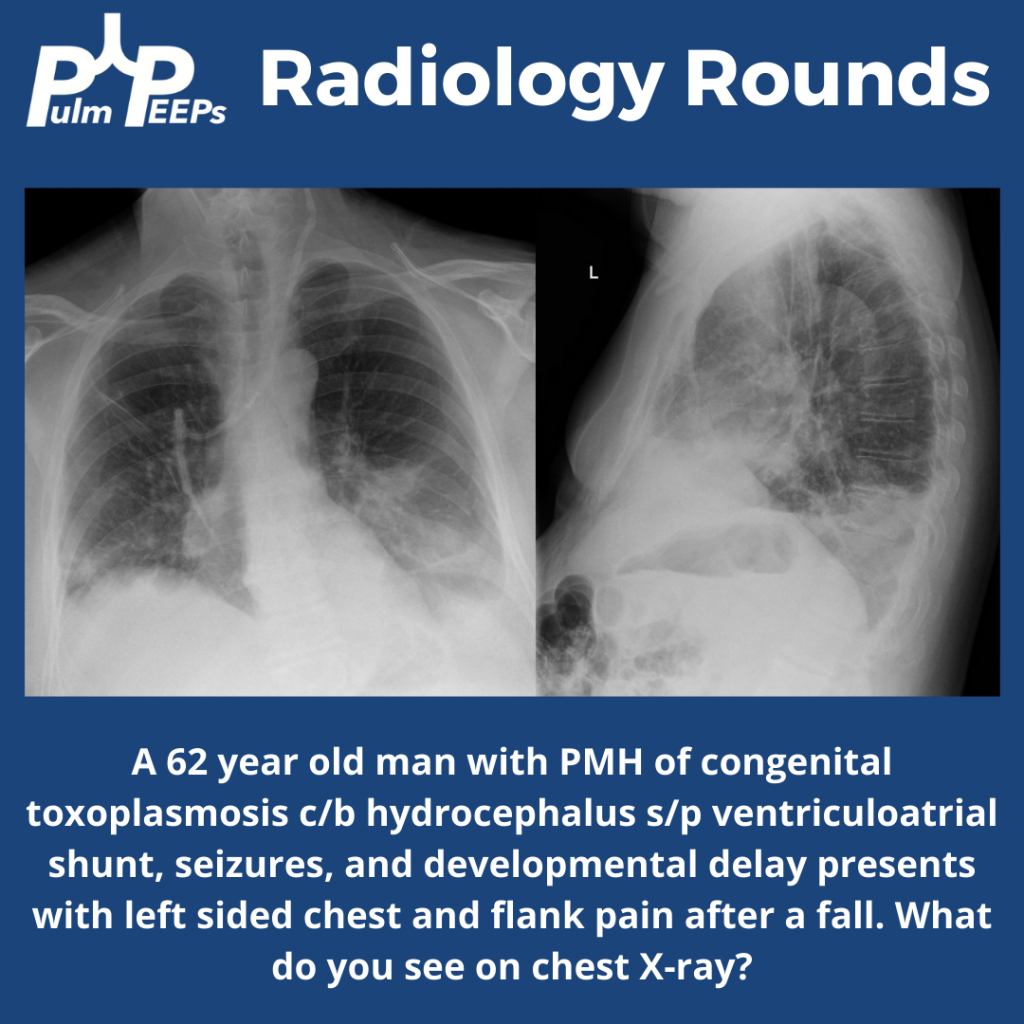
What better way to celebrate Valentine’s Day than with a new #RadiologyRounds?! We think it is time for a Lung-centered holiday, but until then enjoy this case.
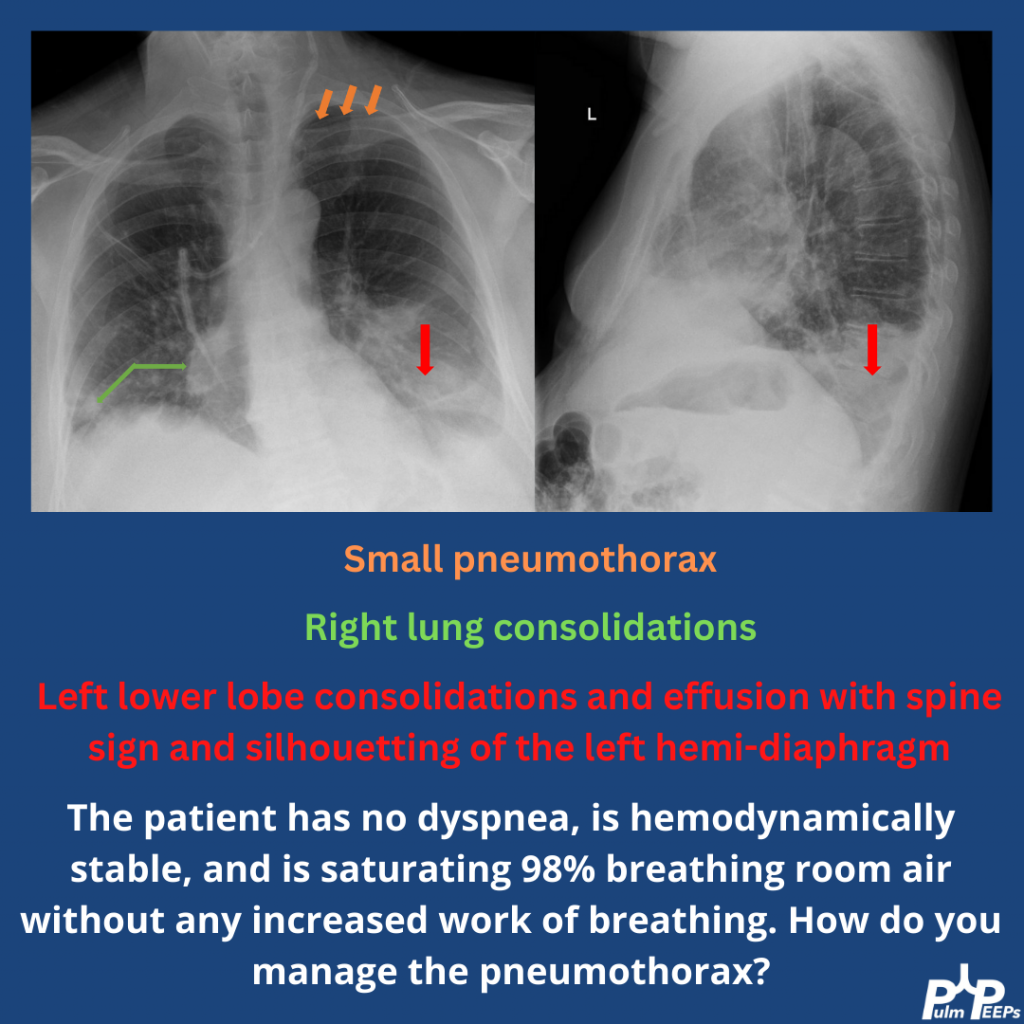
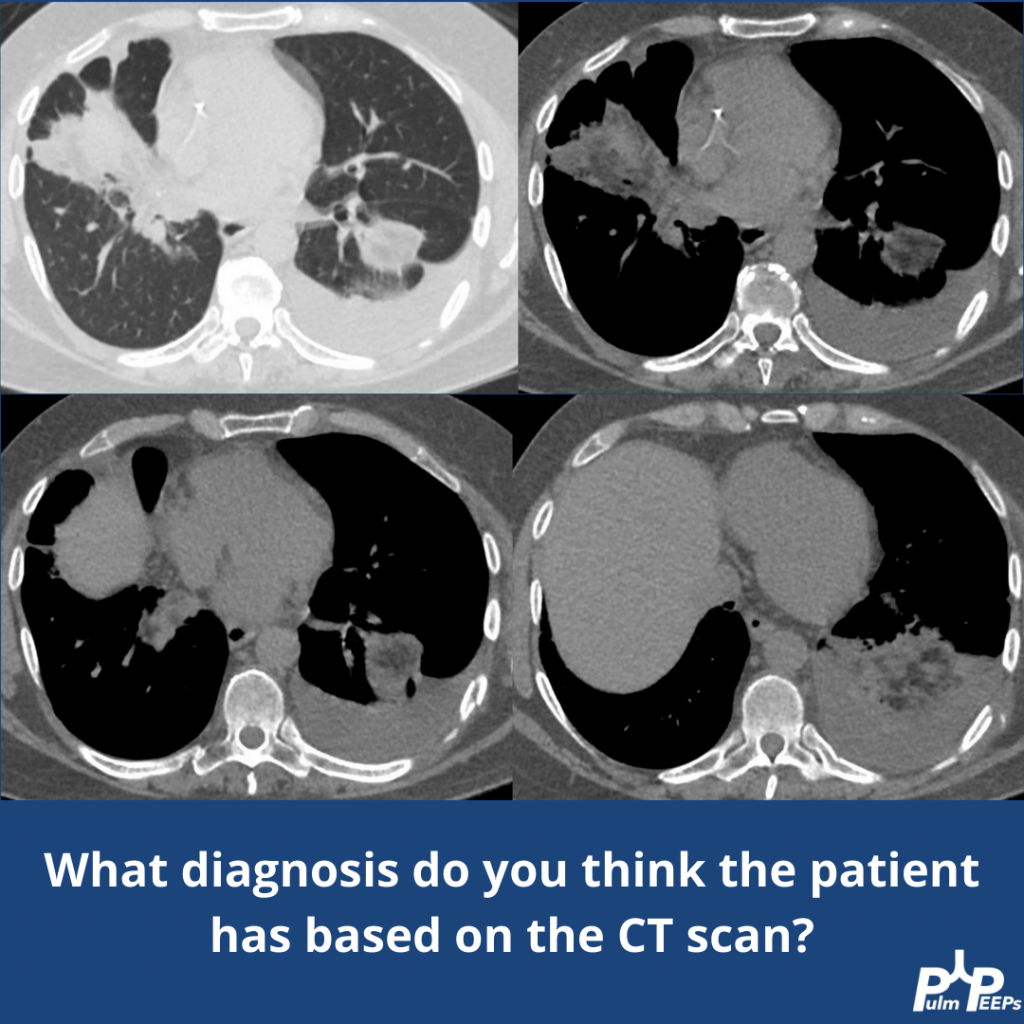
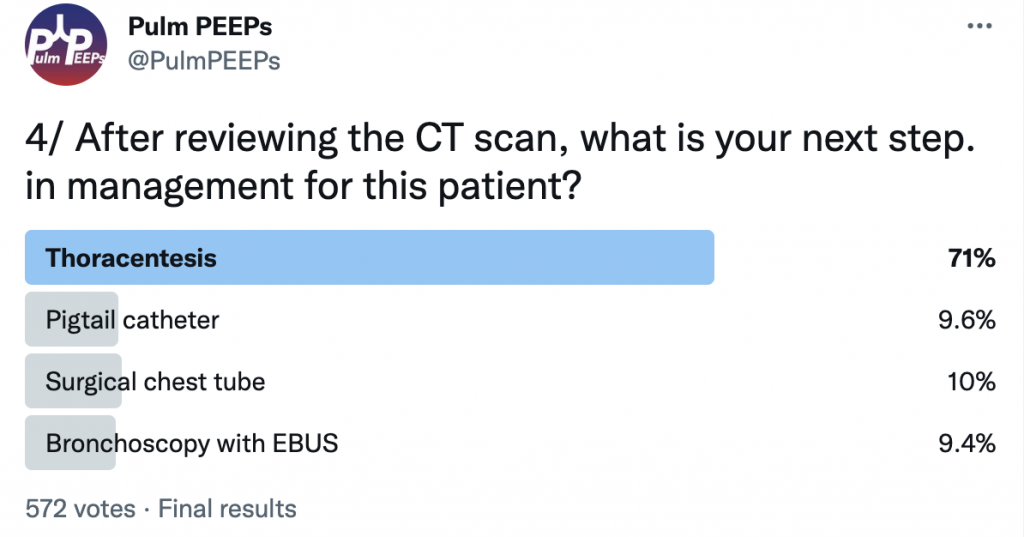
The patient’s pneumothorax was managed conservatively with observation and temporary 100% oxygen via a non-rebreather for nitrogen washout. The consolidations and effusion were concerning, so the patient had a CT chest performed.
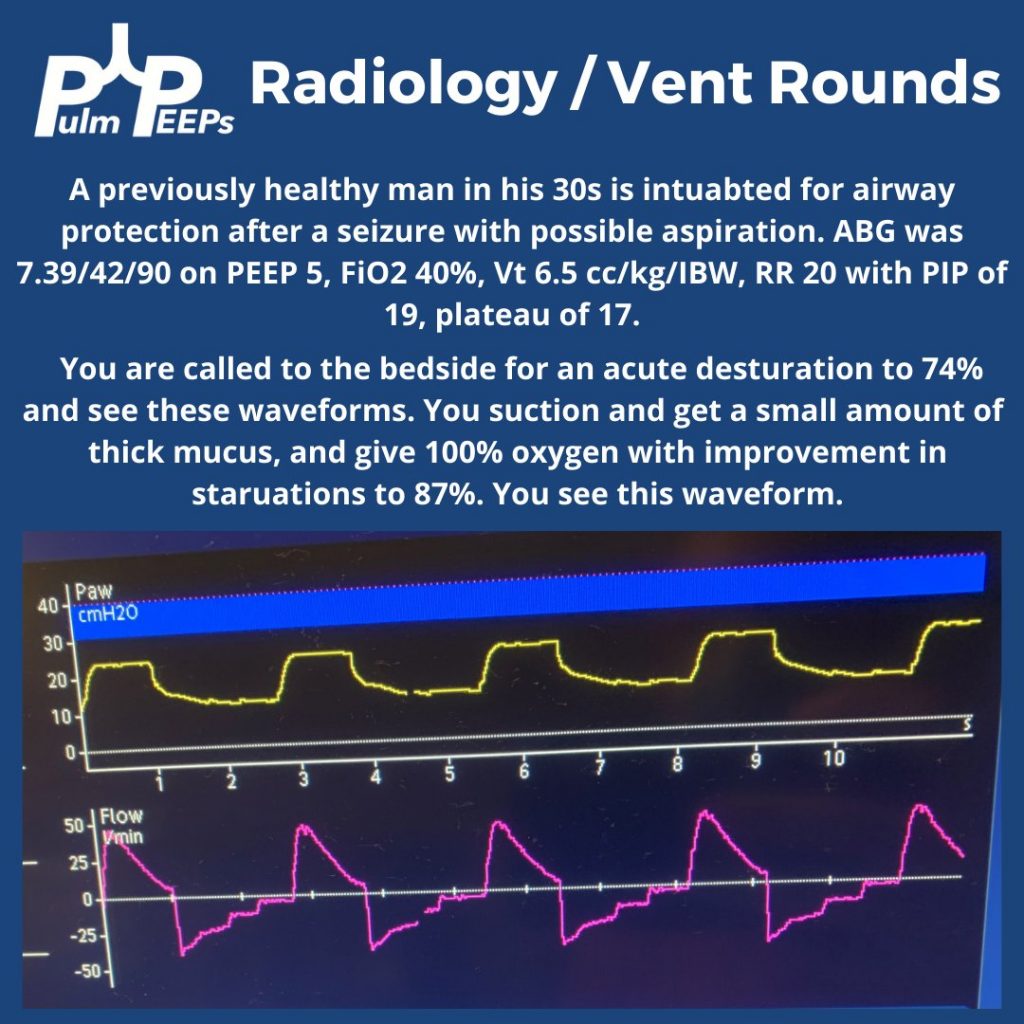
For today’s #RadiologyRounds we have a combined Radiology and Ventilator imaging rounds! You’re in the ICU caring for a young patient on a ventilator when you are called to the bedside for a desaturation.
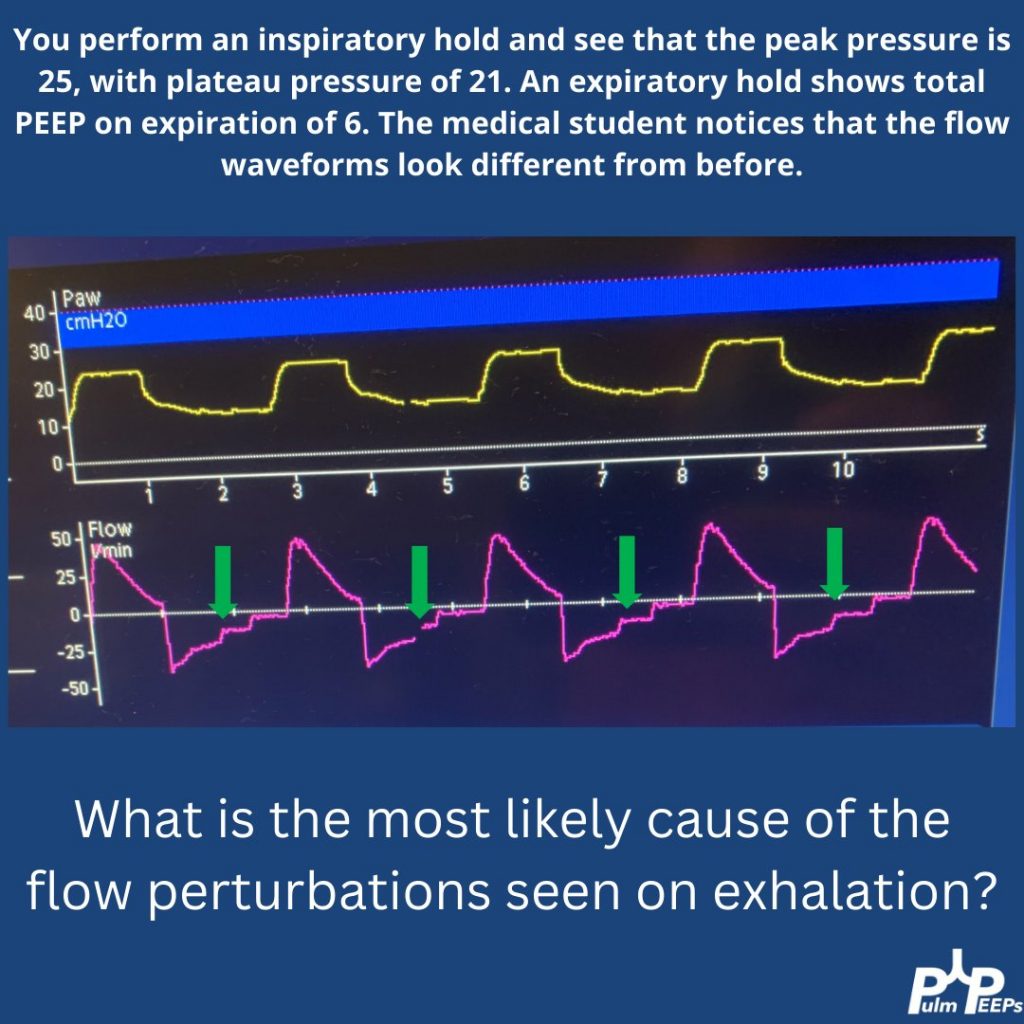
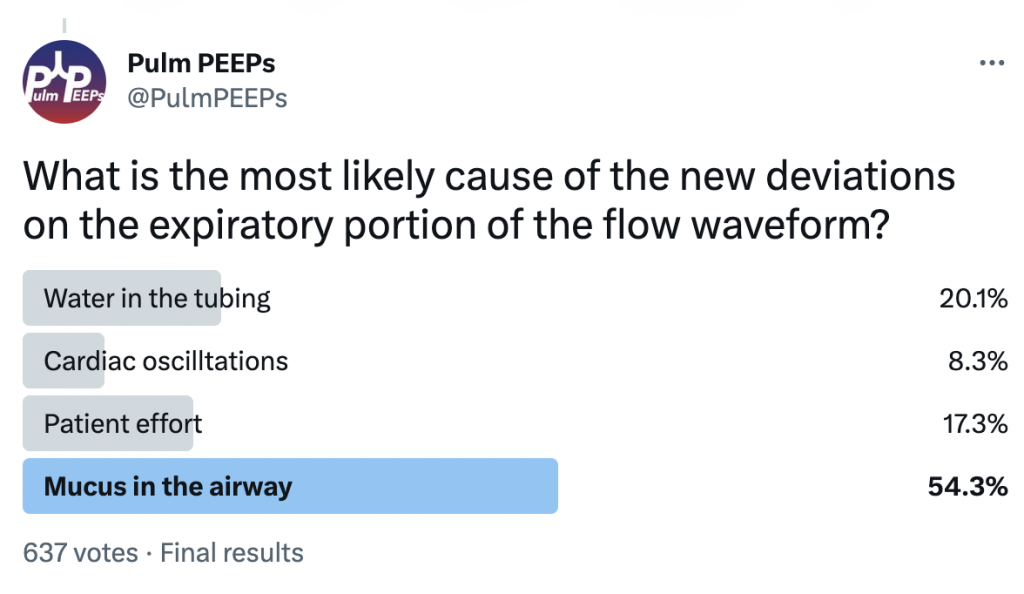
You perform an inspiratory hold and see that the PIP, plateau, and difference between peak and plateau have all increased. On exam you hear bilateral mechanical breath sounds anteriorly. You order a CXR and the student asks a question about the waveforms
There are pressure deviations corresponding to the flow deviations.
There is no clear patient effort The fact that the PIP and plat have changed makes water in the tubing or cardiac oscillations less likely.
You think this is mucus, with a plug ball-valving in a bronchus
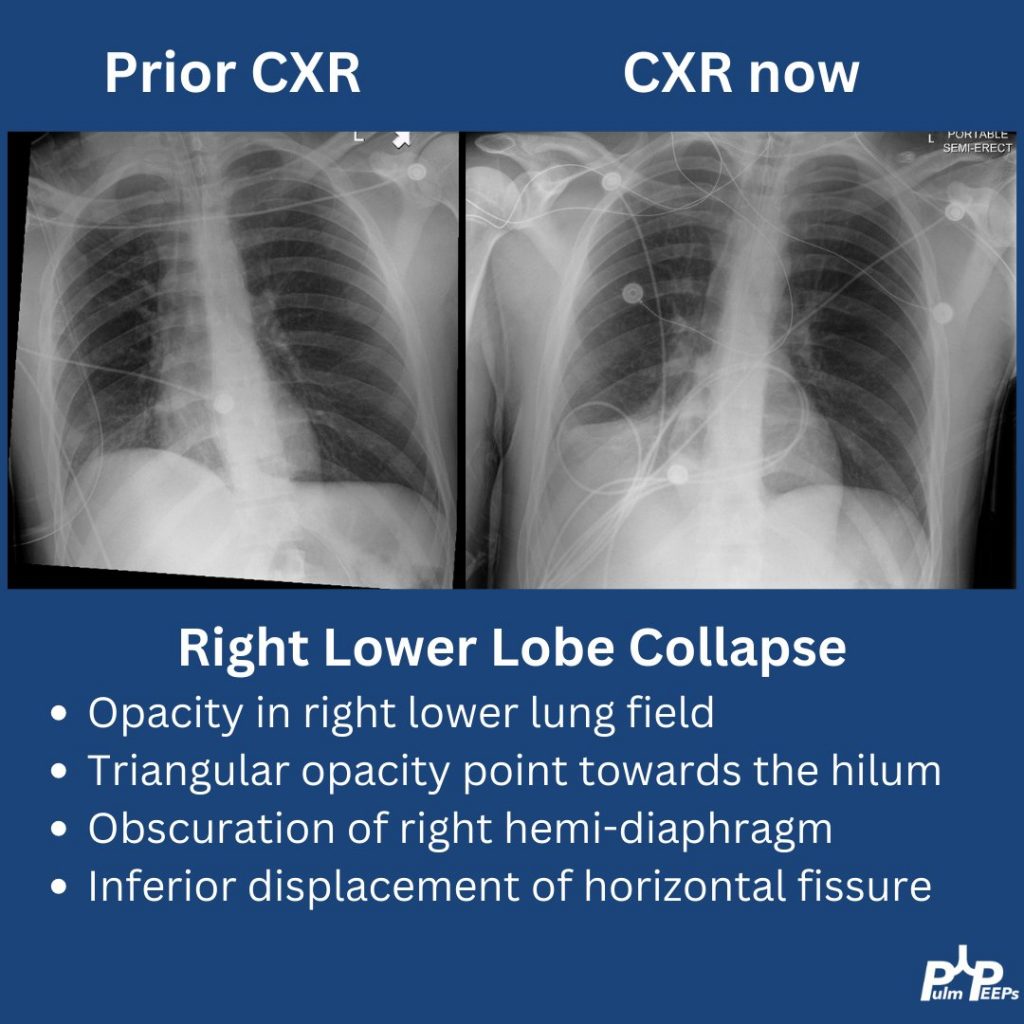
The CXR arrives and shows right lower lobe collapse.
A bedside bronchoscopy is performed with large mucus plugs suctioned out of the RLL and RML. Afterward, the patient’s oxygenation is improved, the flow deviations resolve, and the plateau pressure drops to 19
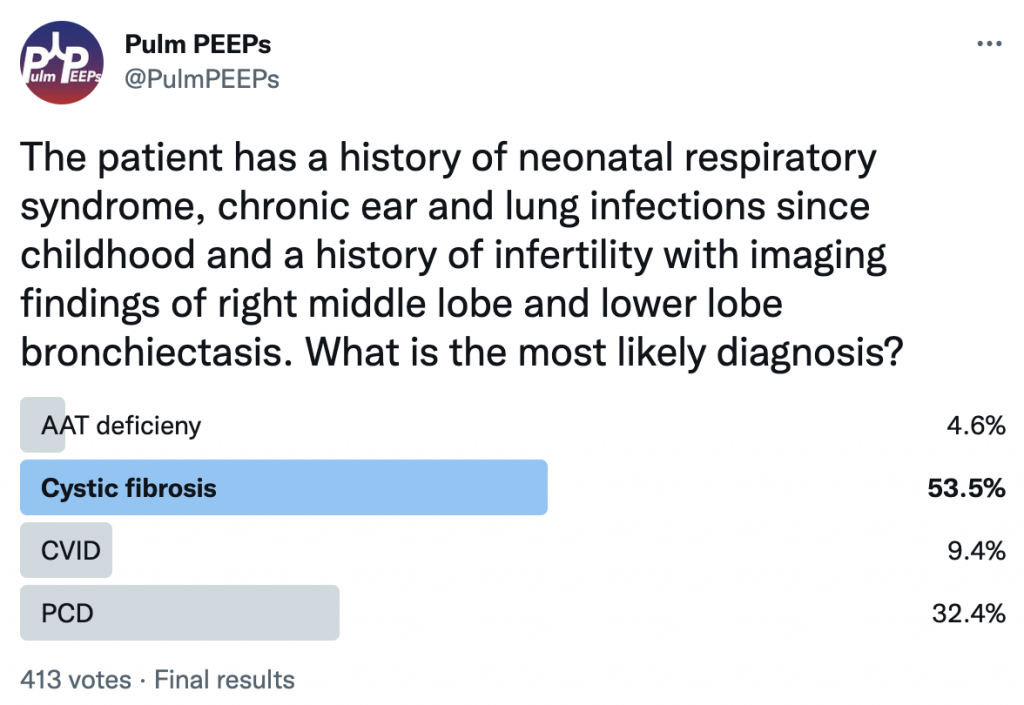
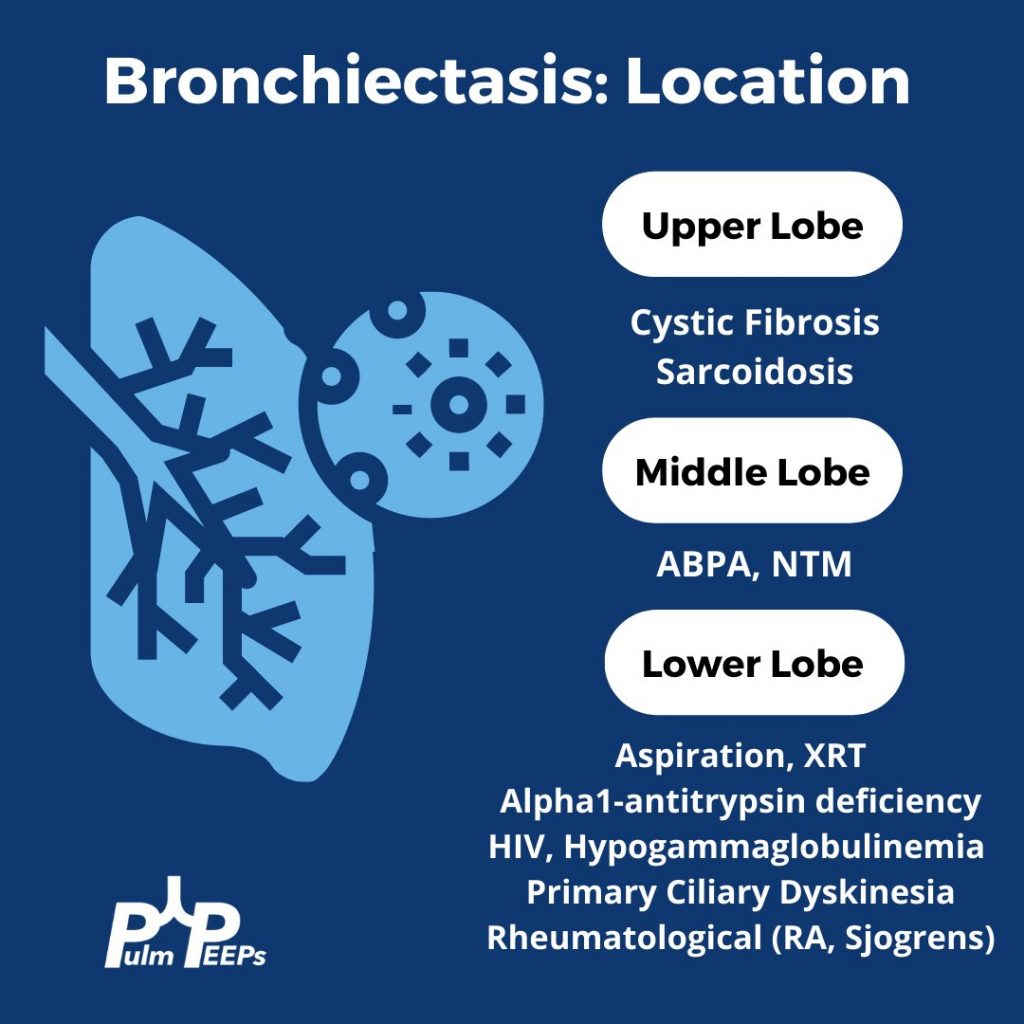
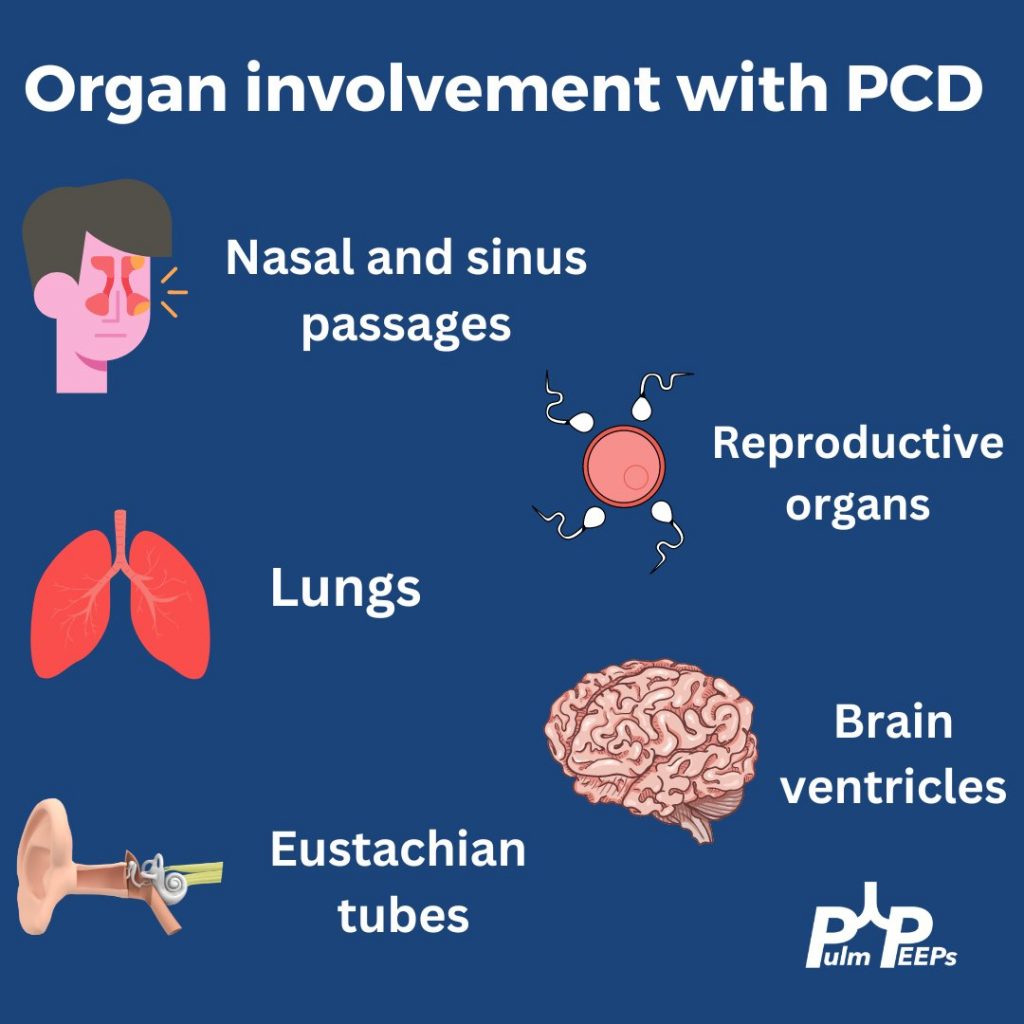
While chronic lung infections and infertility are overlapping symptoms for CF and Primary Ciliary Dyskinesia, the history of neonatal respiratory syndrome, ear infections and lower lobe bronchiectasis are most consistent with PCD
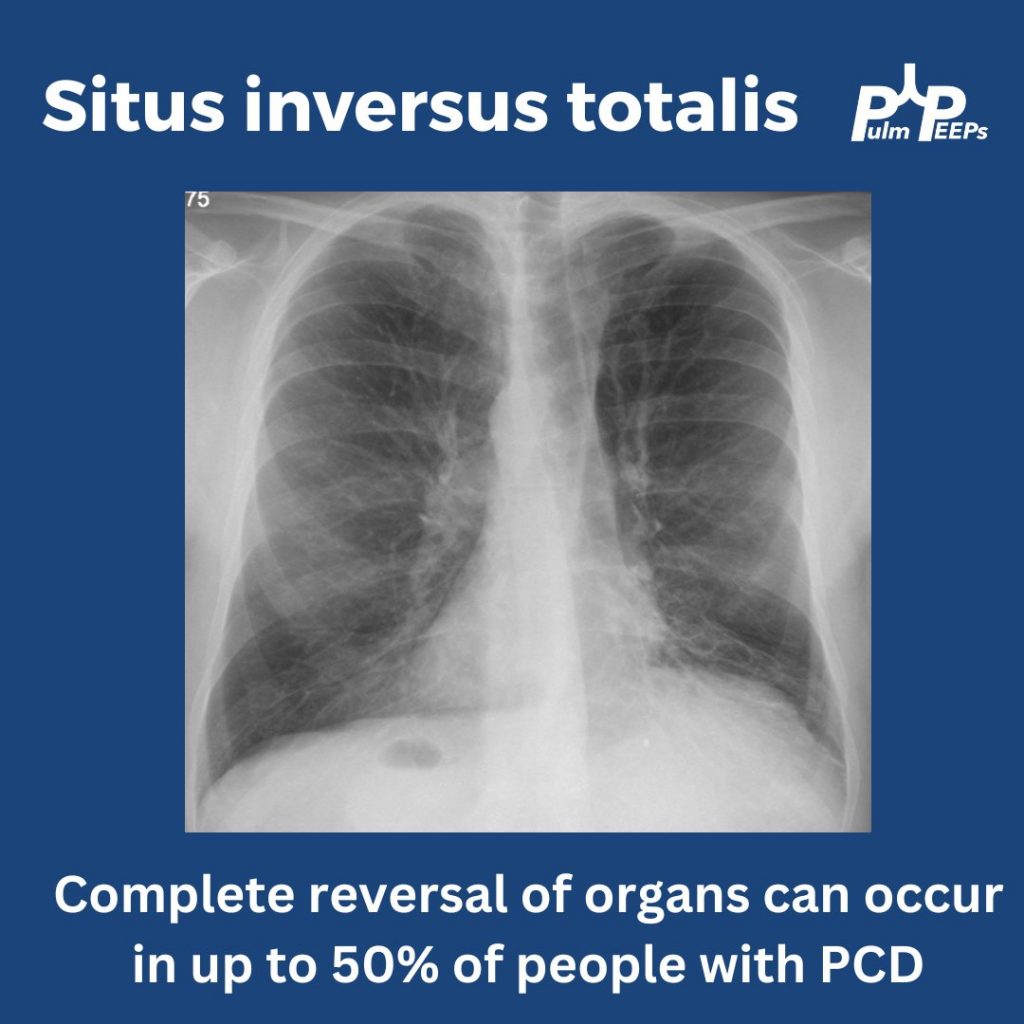
In up to 50% of people with PCD, you can get complete reversal of thoracic and abdominal organs. In this film you can see the heart in the right hemithorax, the gastric bubble on the right with the liver on the left resulting in elevation of the left hemidiaphragm
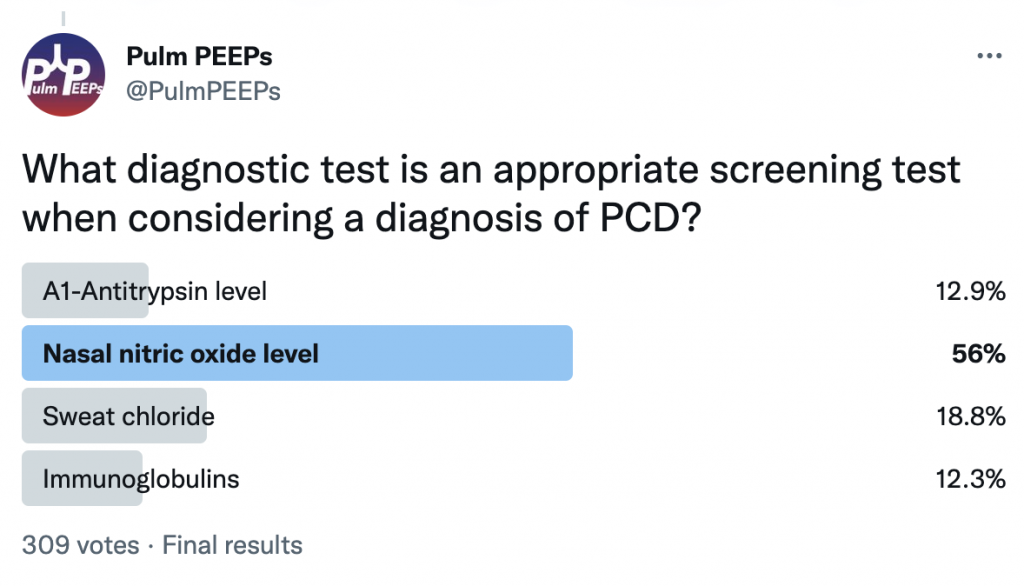
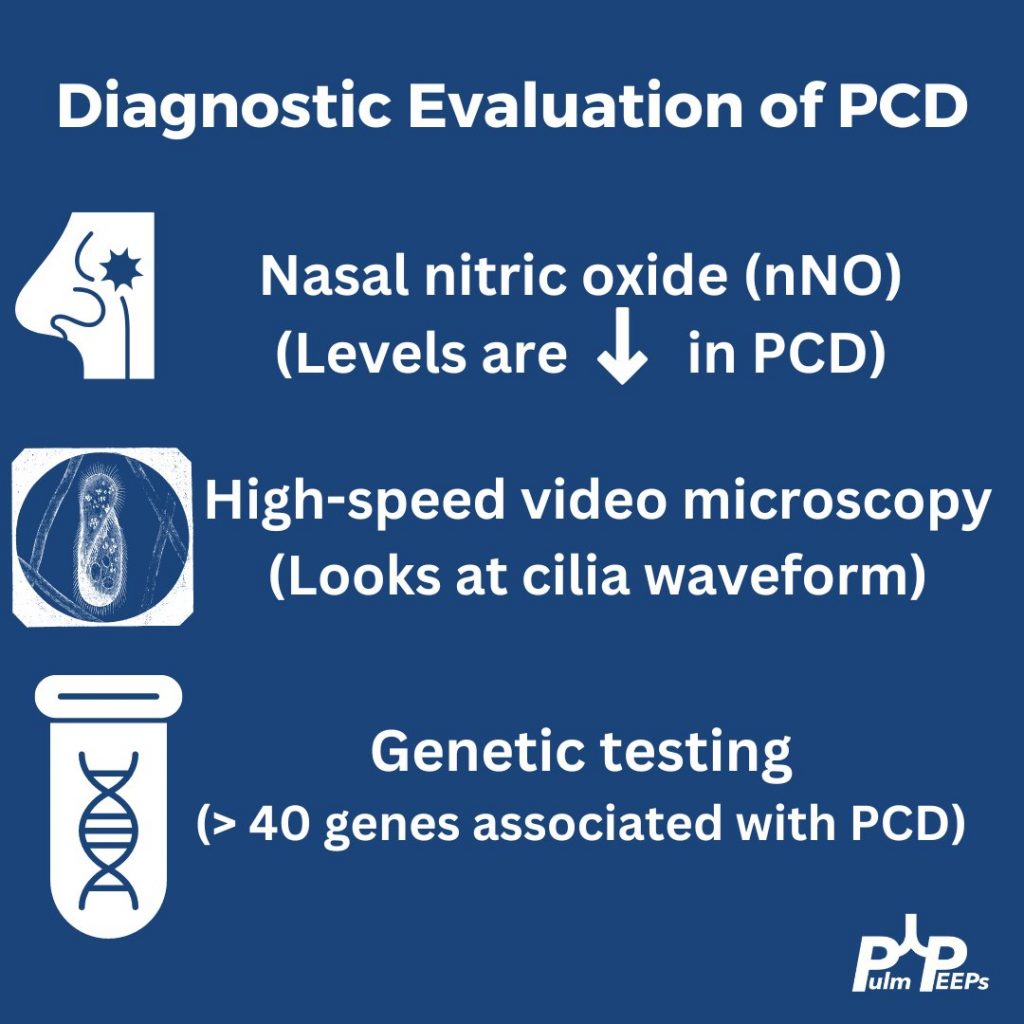
In patients with clinical symptoms and two decreased levels of nasal nitric oxide these findings suggest a PCD diagnosis but evaluation of the cilia structure and function as well as genetic testing are other diagnostic evaluations to confirm a diagnosis of PCD
Primary ciliary dyskinesia is a autosomal recessive disorder that results in motile ciliary dysfunction and clinical manifestations can vary depending on which organs are involved
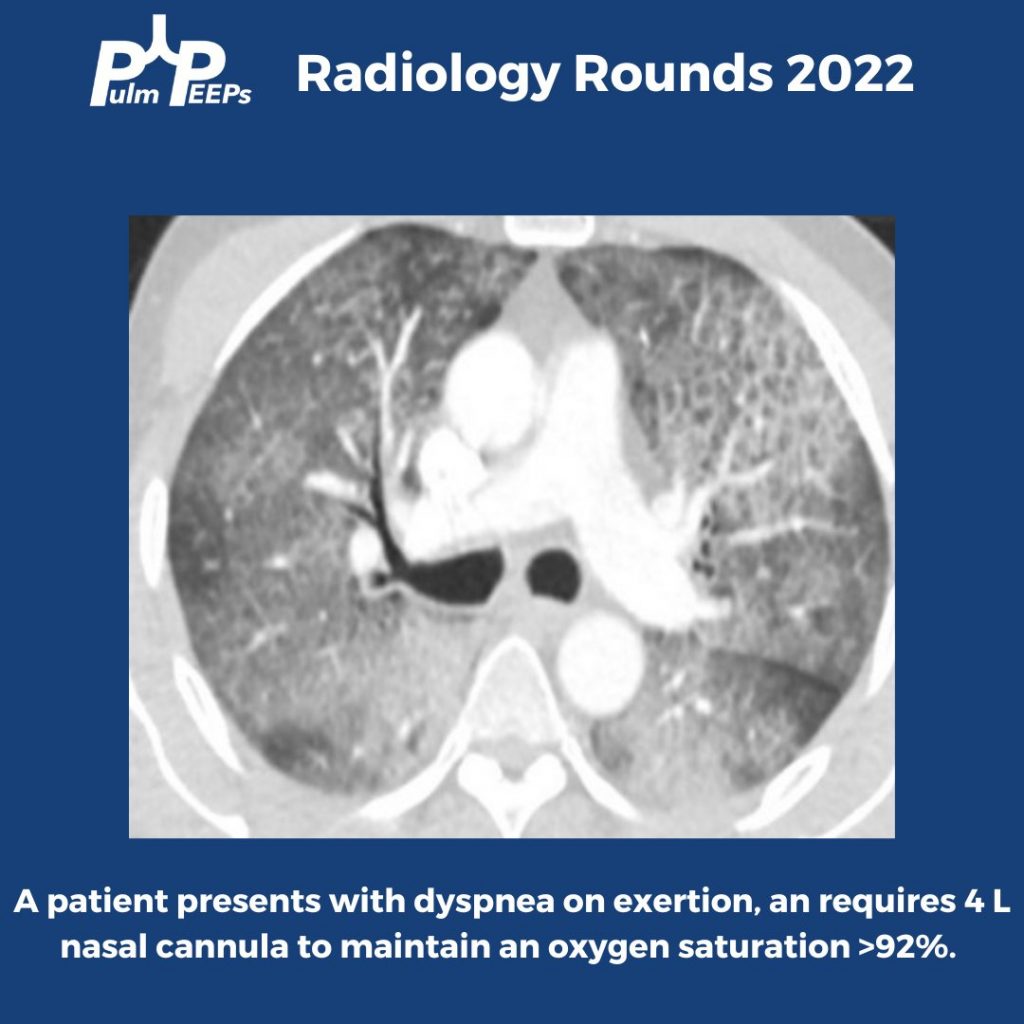
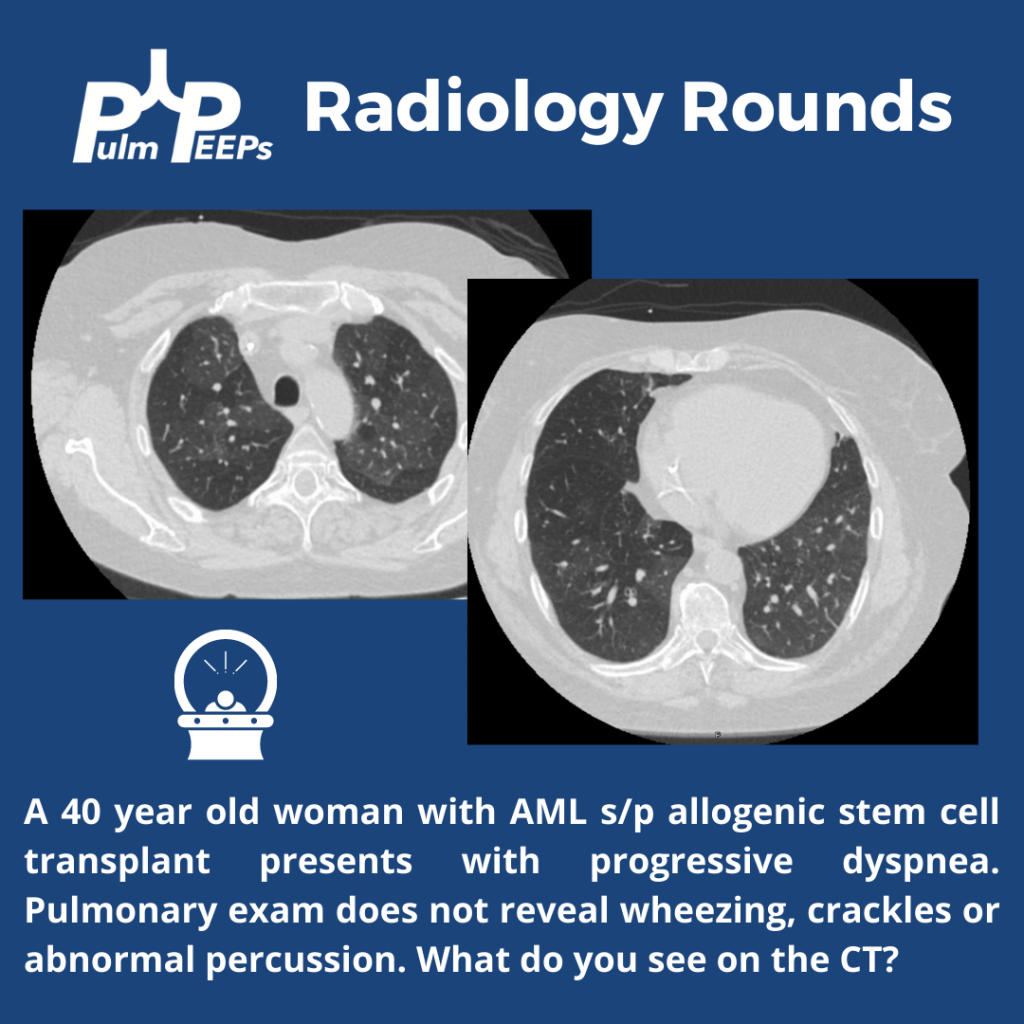
A 40-year-old patient s/p allogeneic stem cell transplant for AML 6 months prior presents with progressive dyspnea. The exam is unrevealing and imaging is obtained.
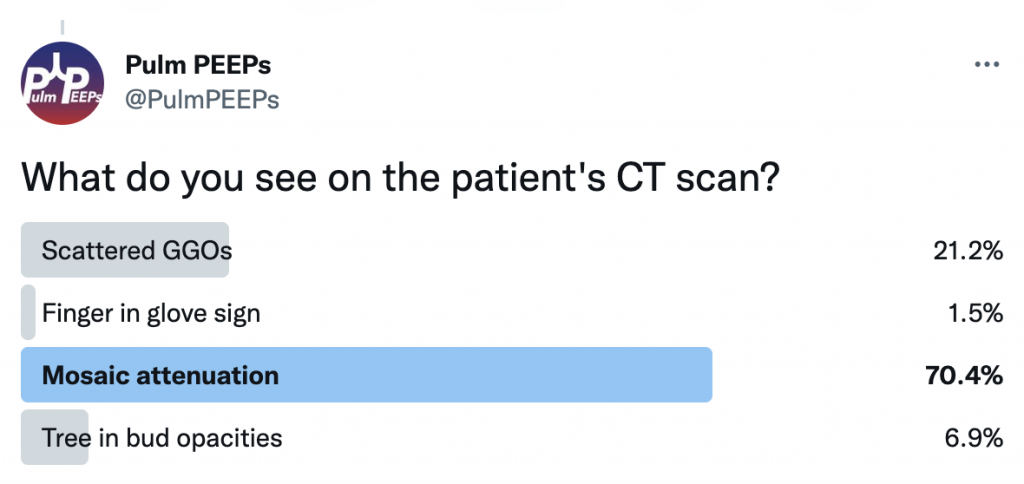
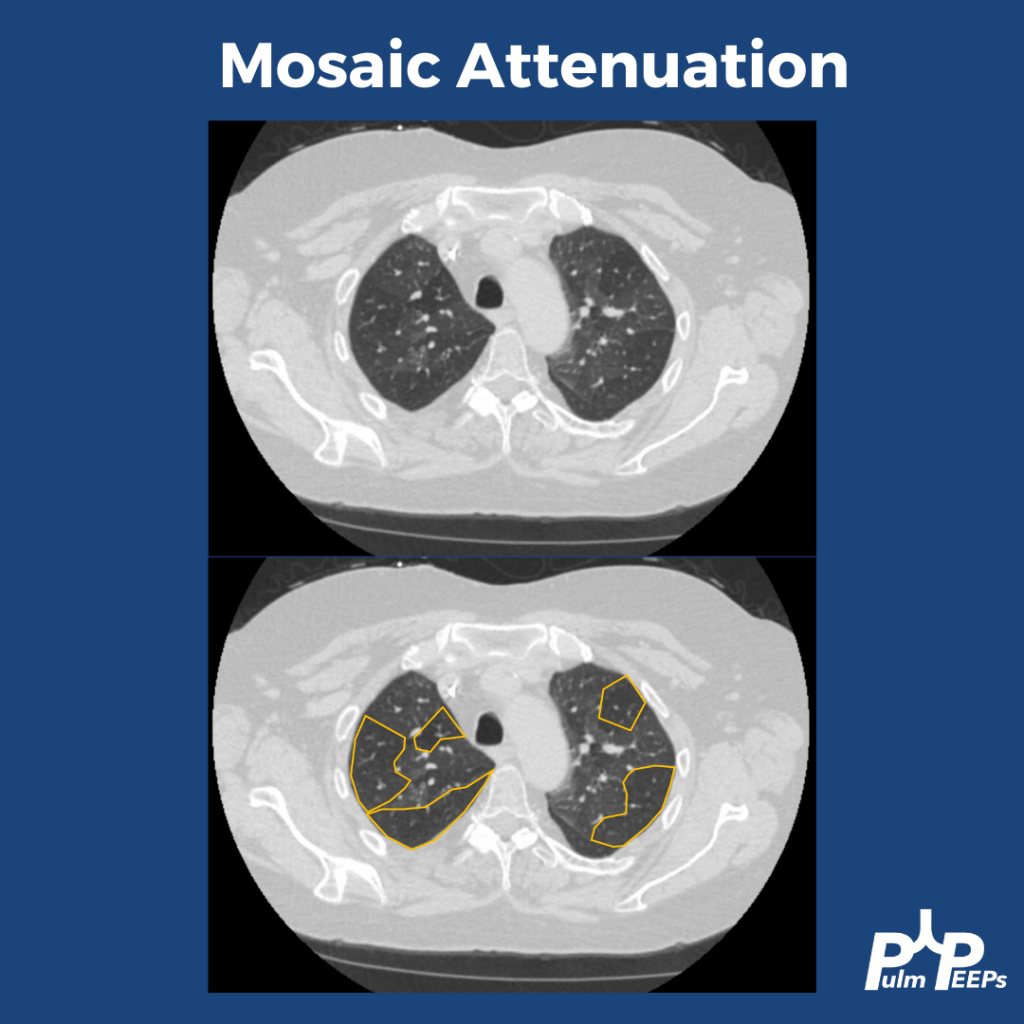
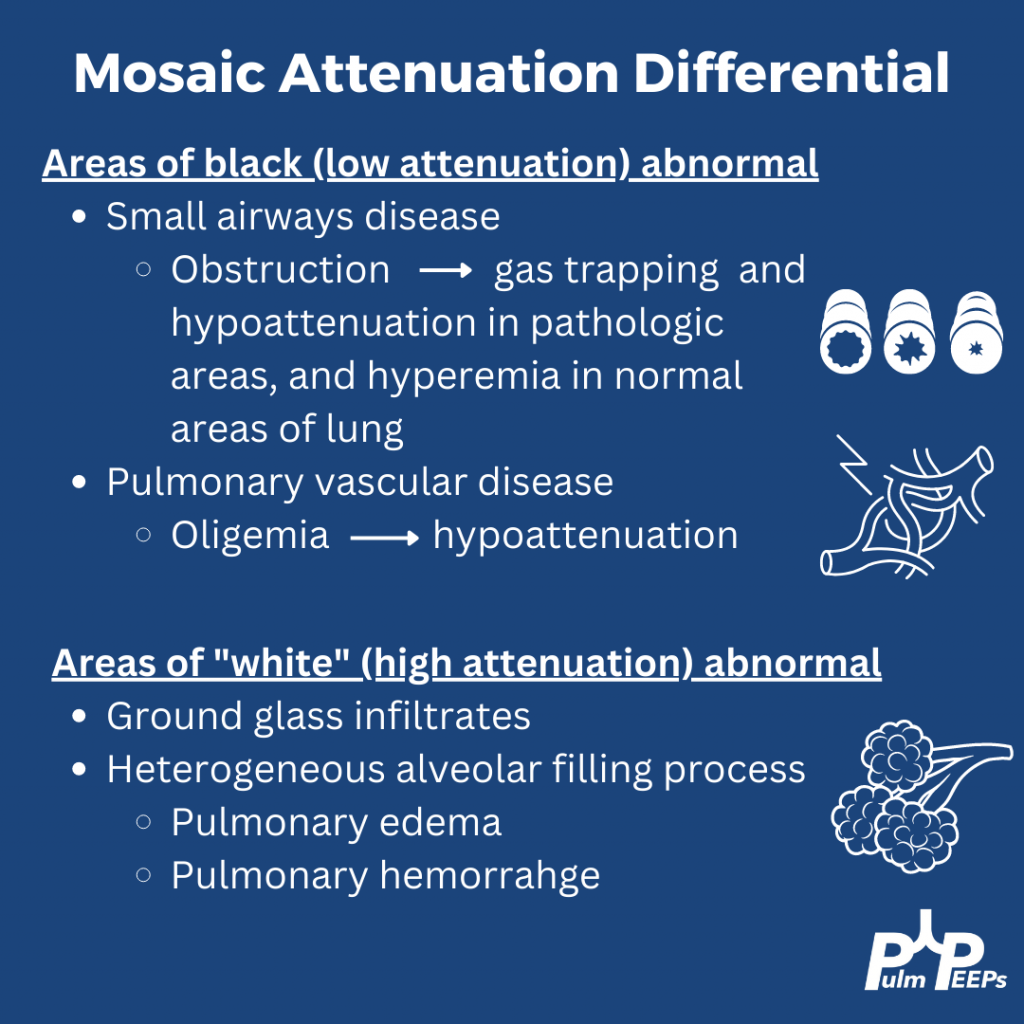
The patient’s CT reveals mosaic attenuation. Mosiac attenuation is a pattern of scattered regions of the lung with differing densities. The abnormal portions can be those that appear white or black.
Tip: Inspiratory and expiratory films can help identify the cause!
The patient had PFTs that showed severe obstruction, and significant change from PFTs prior to the stem cell transplant. Inspiratory and expiratory CT confirmed significant areas of gas trapping. She was diagnosed with bronchiolitis obliterans secondary to chronic GVHD
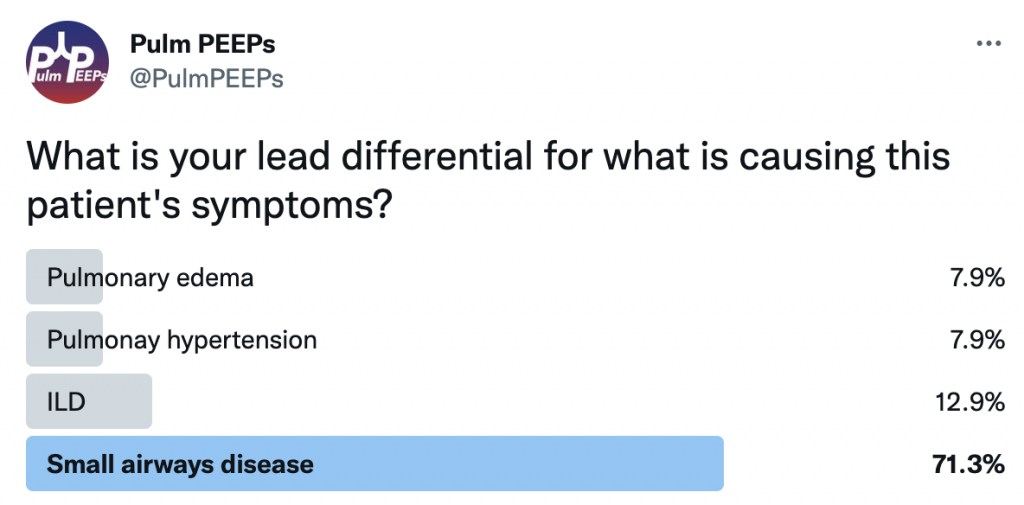
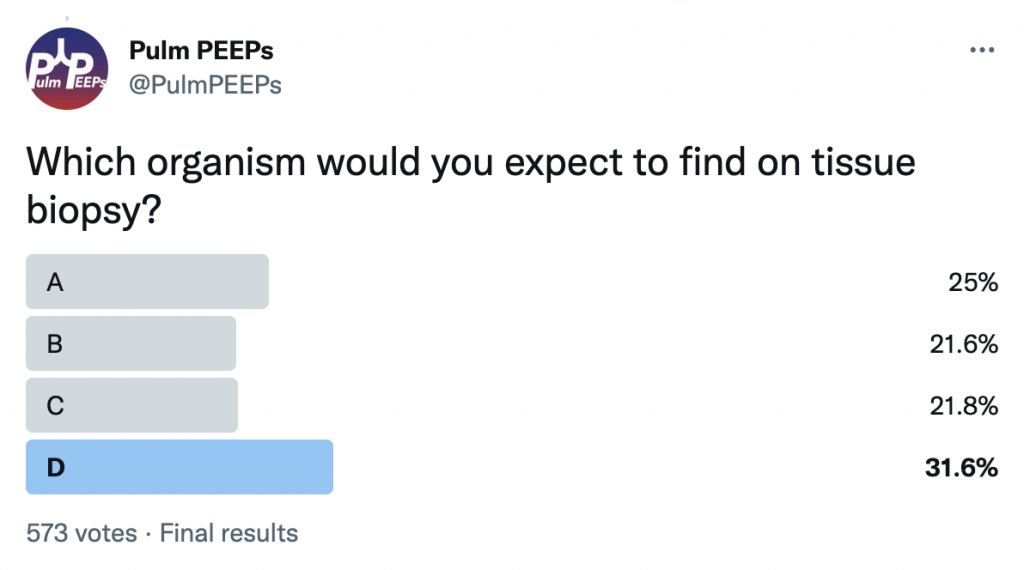
A middle-aged male presents with sub-acute fatigue, fevers and dyspnea on exertion. His admission labs are notable for severe neutropenia (ANC < 500)
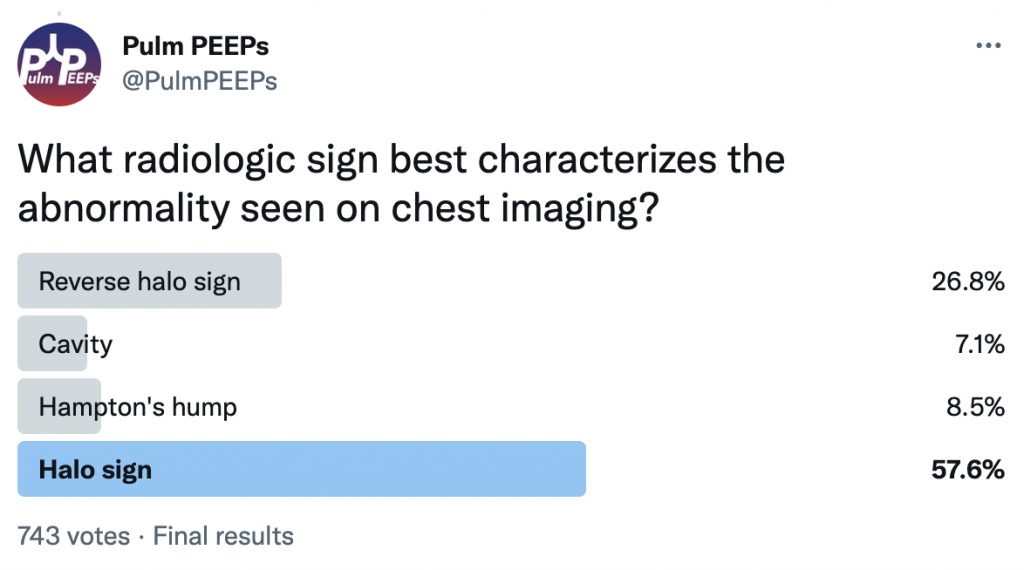
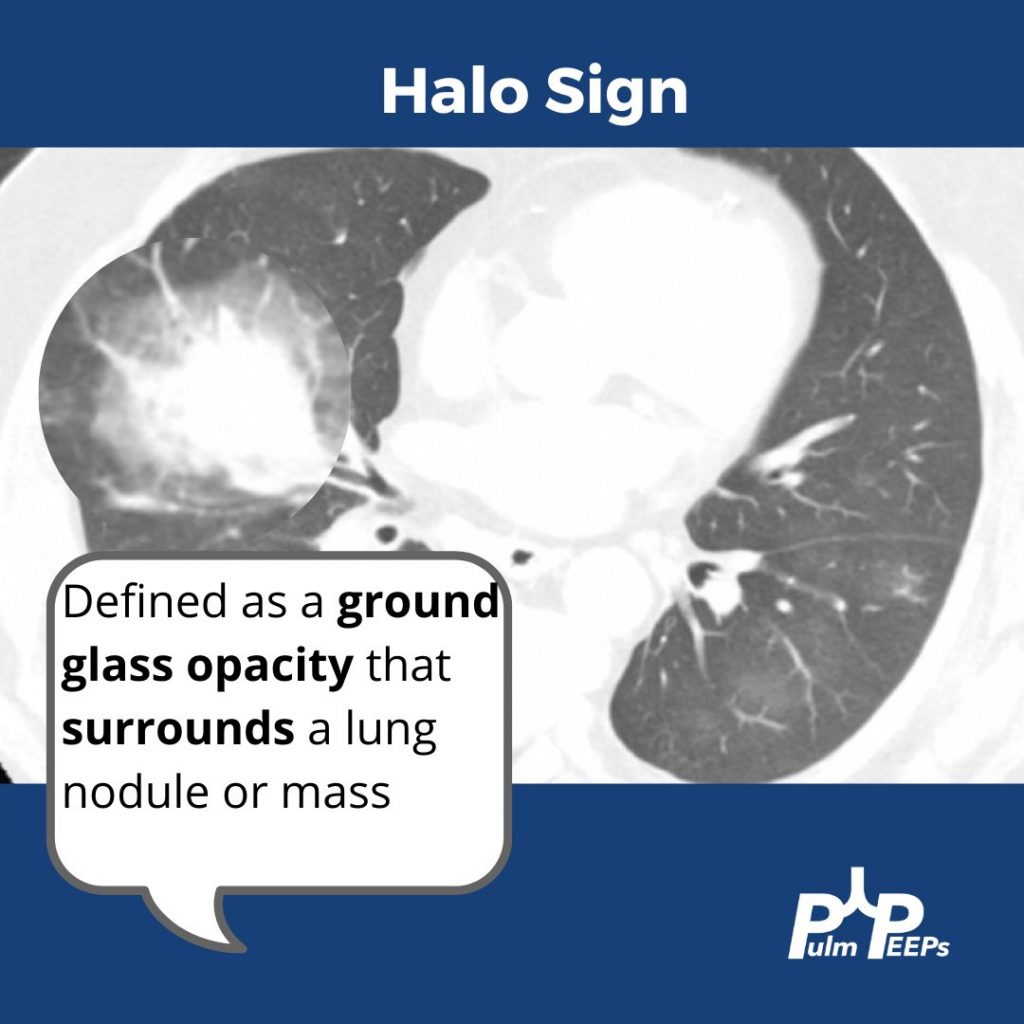
This patient has evidence of a halo sign which represents local vessel invasion or hemorrhage
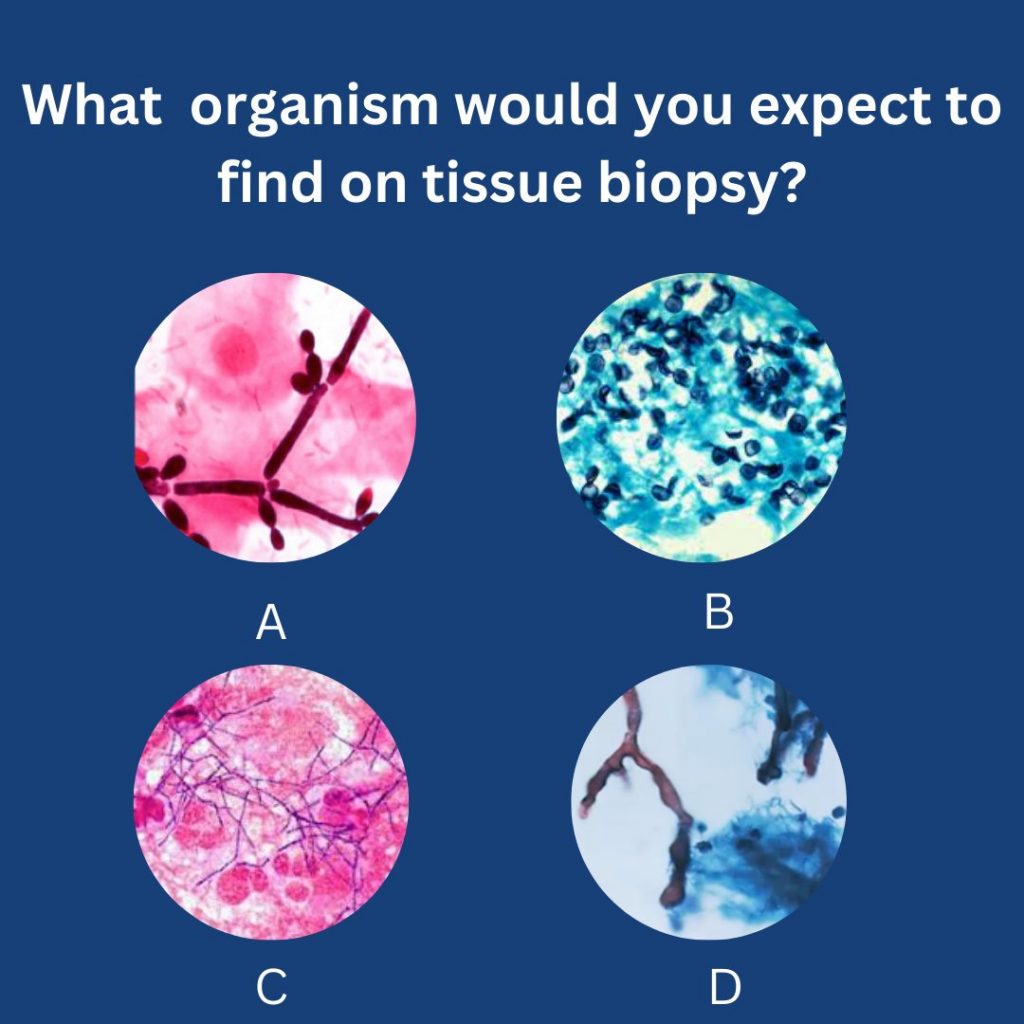
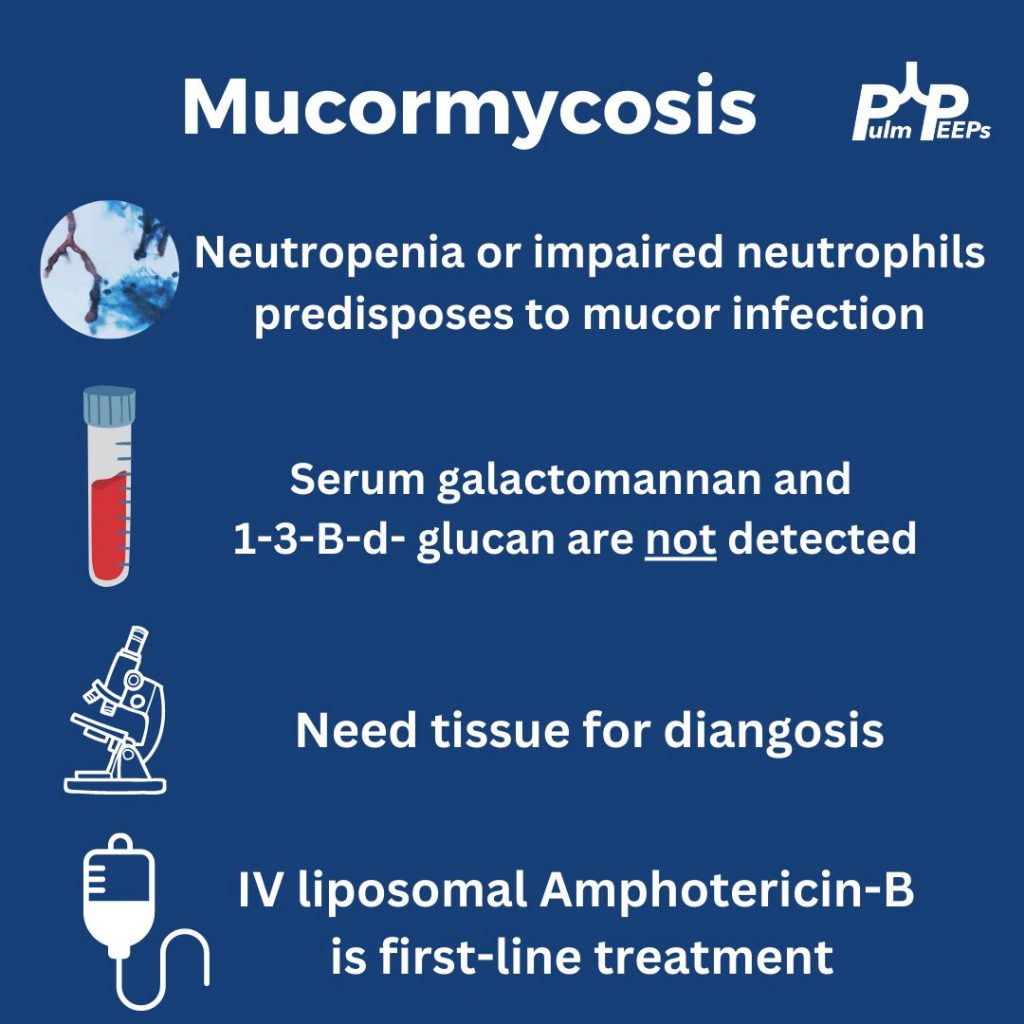
The patient undergoes evaluation. RVP, sputum culture and serum galactomannan and 1-3-B-d-glucan are negative. A BAL with transbronchial biopsies are obtained.
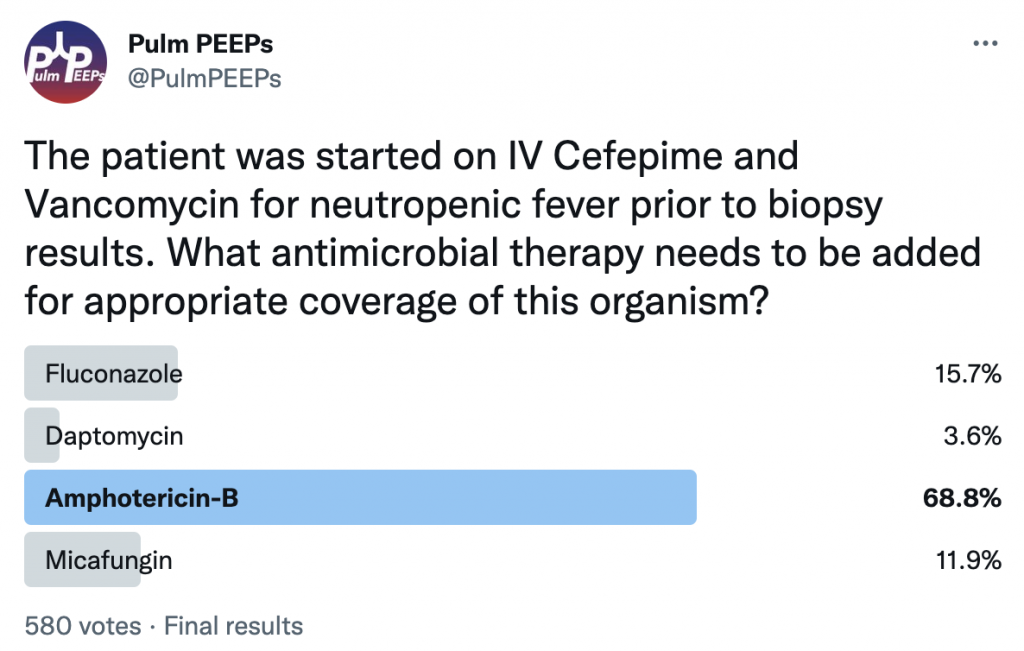
The patient was found to have pulmonary mucormycosis and was started on IV liposomal amphotericin-B.
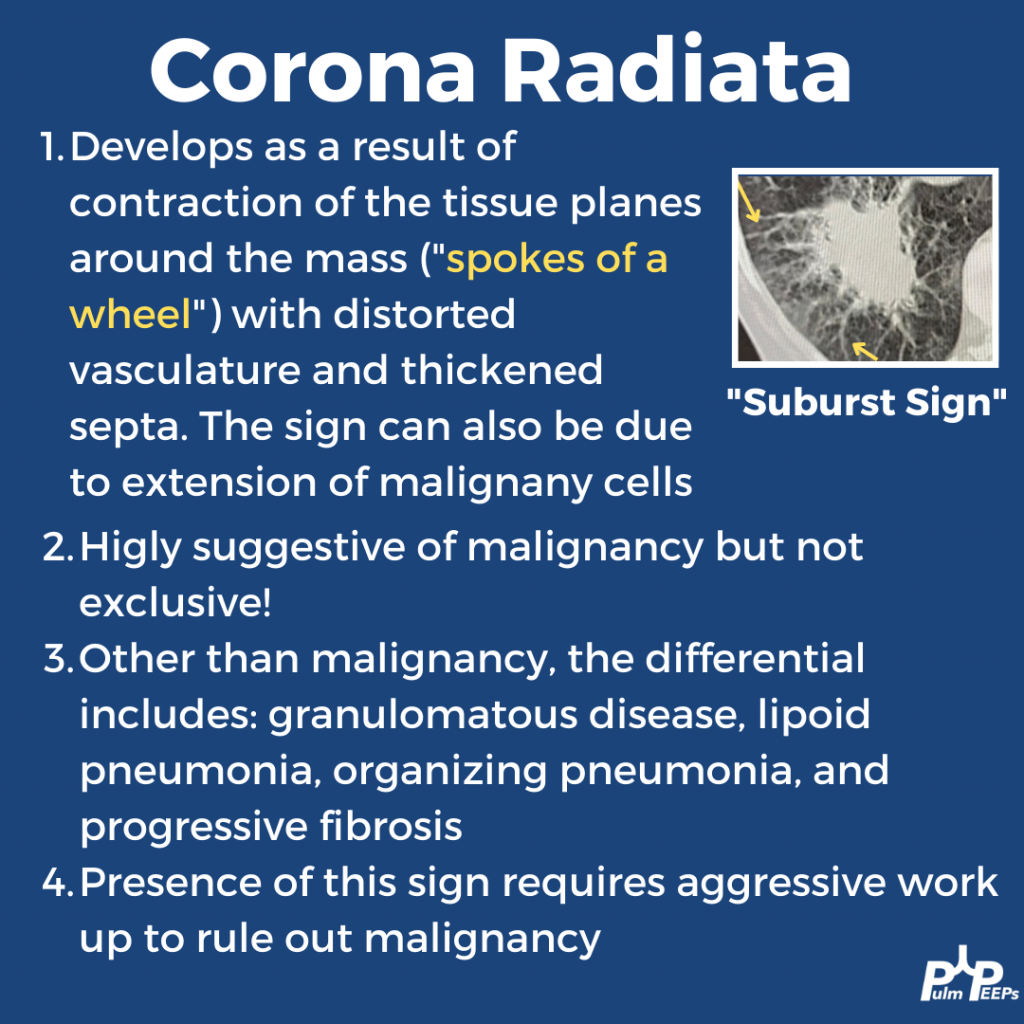
This week’s #RadiologyRounds is brought to you by our newest contributor, Nick Ghionni! We’ll dive into a classic Radiology Sign and talk about what it represents, and how it helps inform your differential.
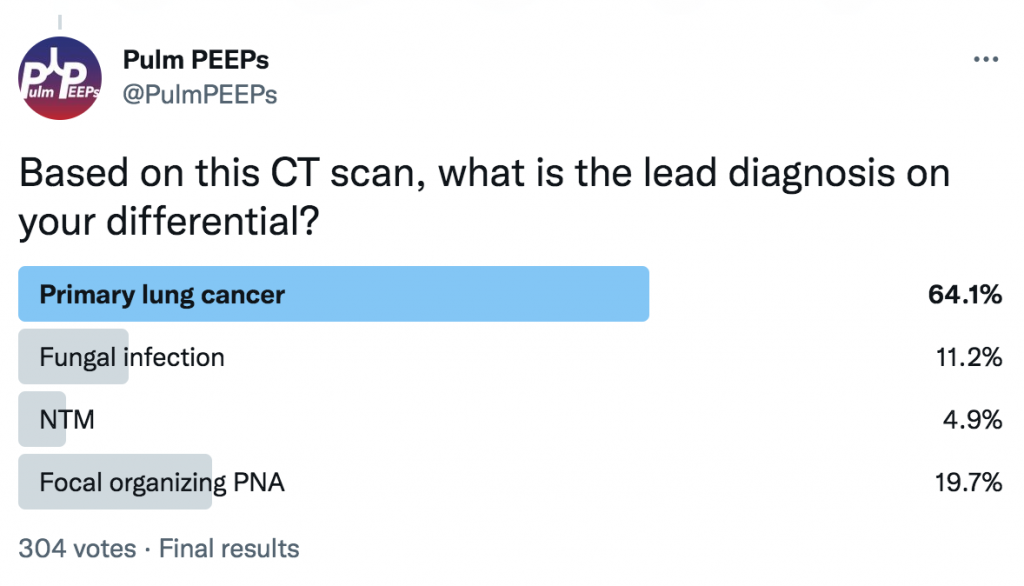
In this case, the patient underwent a biopsy that showed no malignancy but grew NTM! Given that NTM can be superimposed on malignancy, repeated biopsies were done that corroborated. She is being treated with close monitoring.
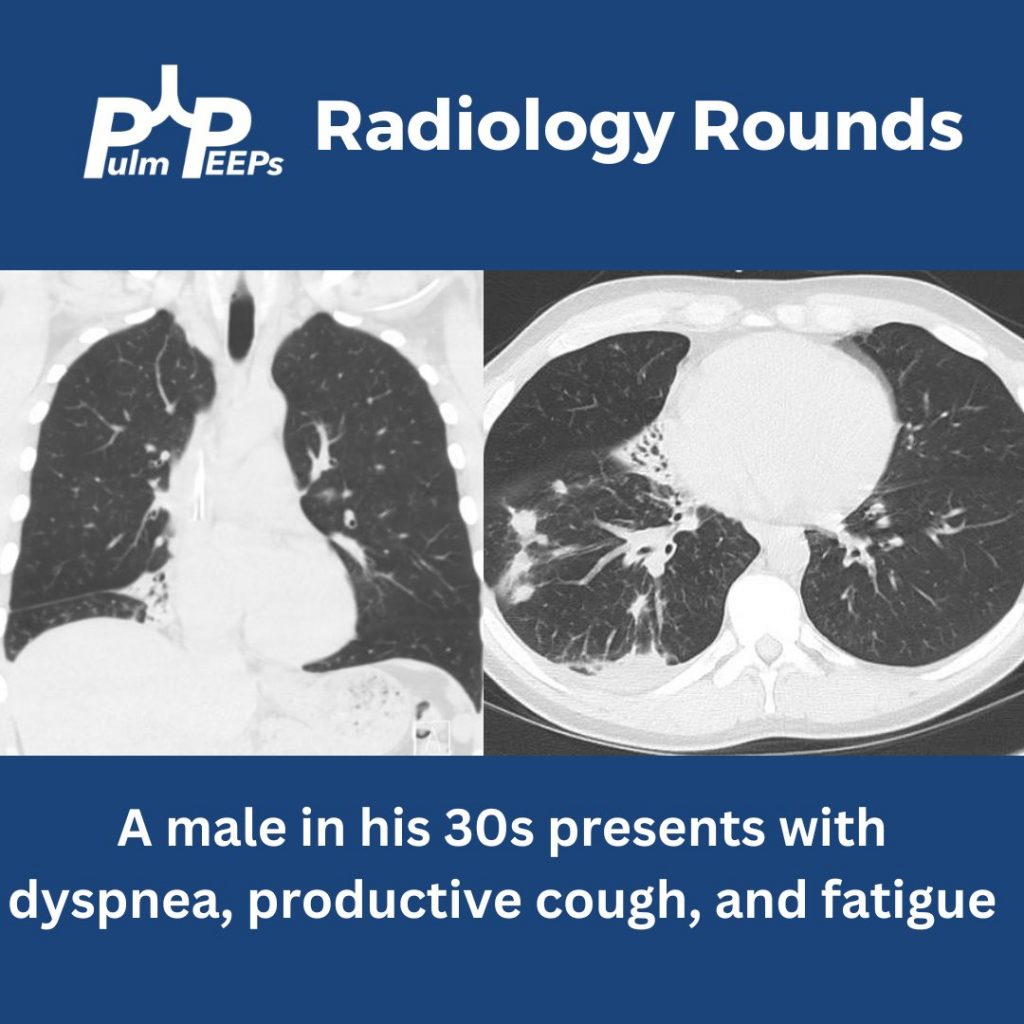
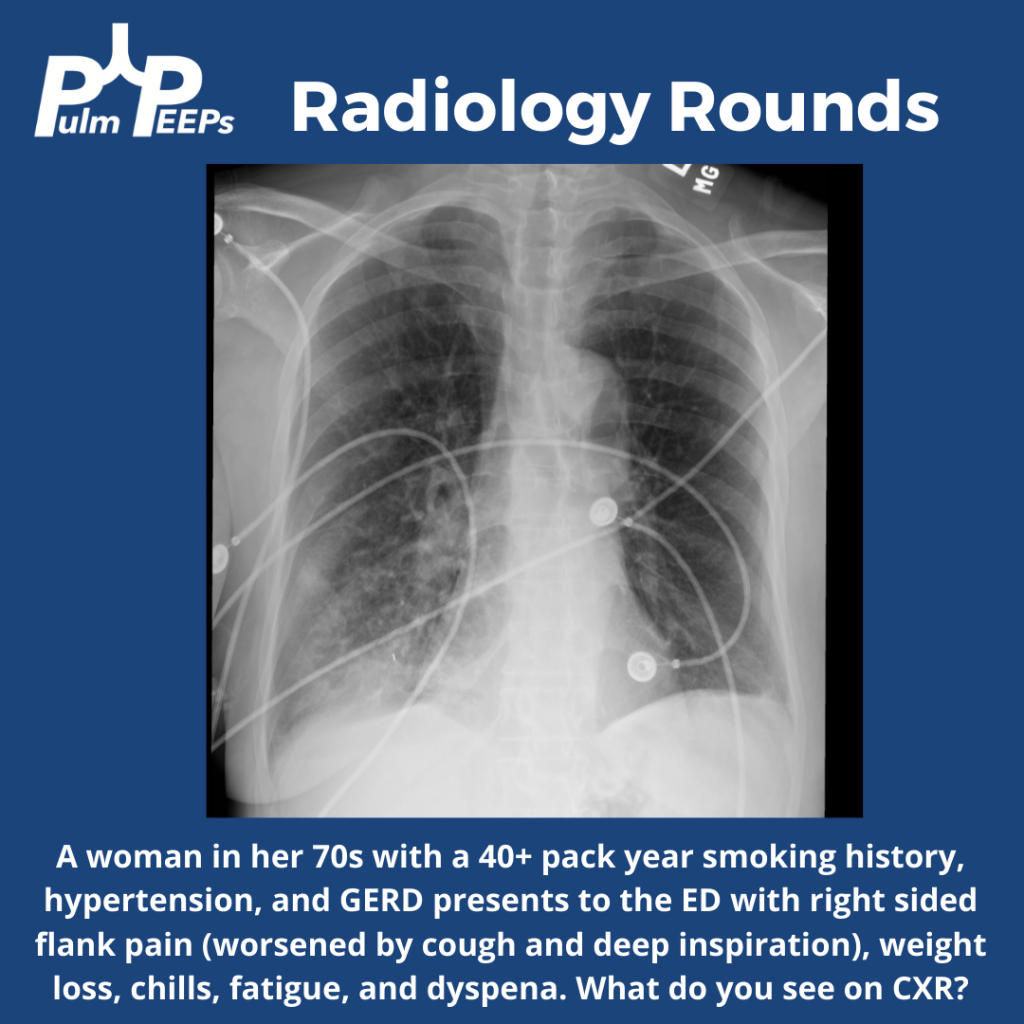
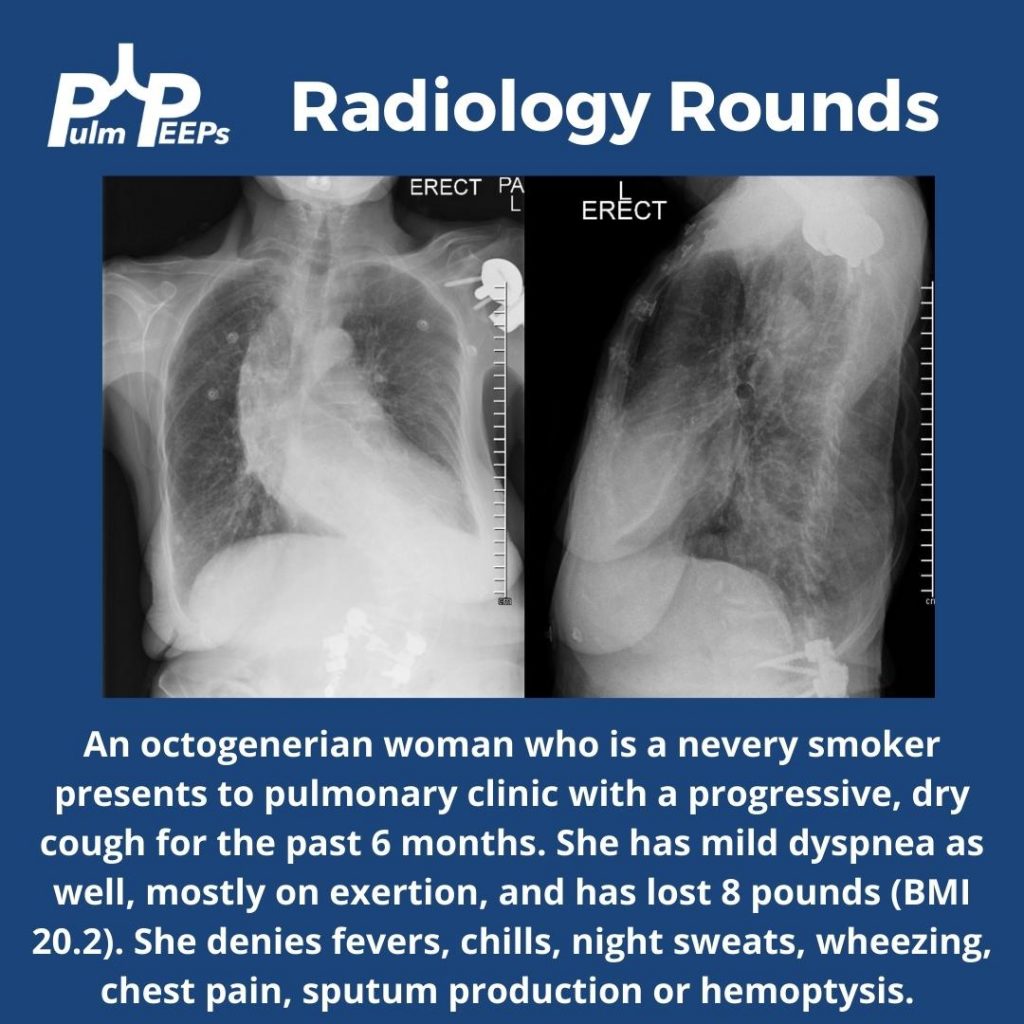
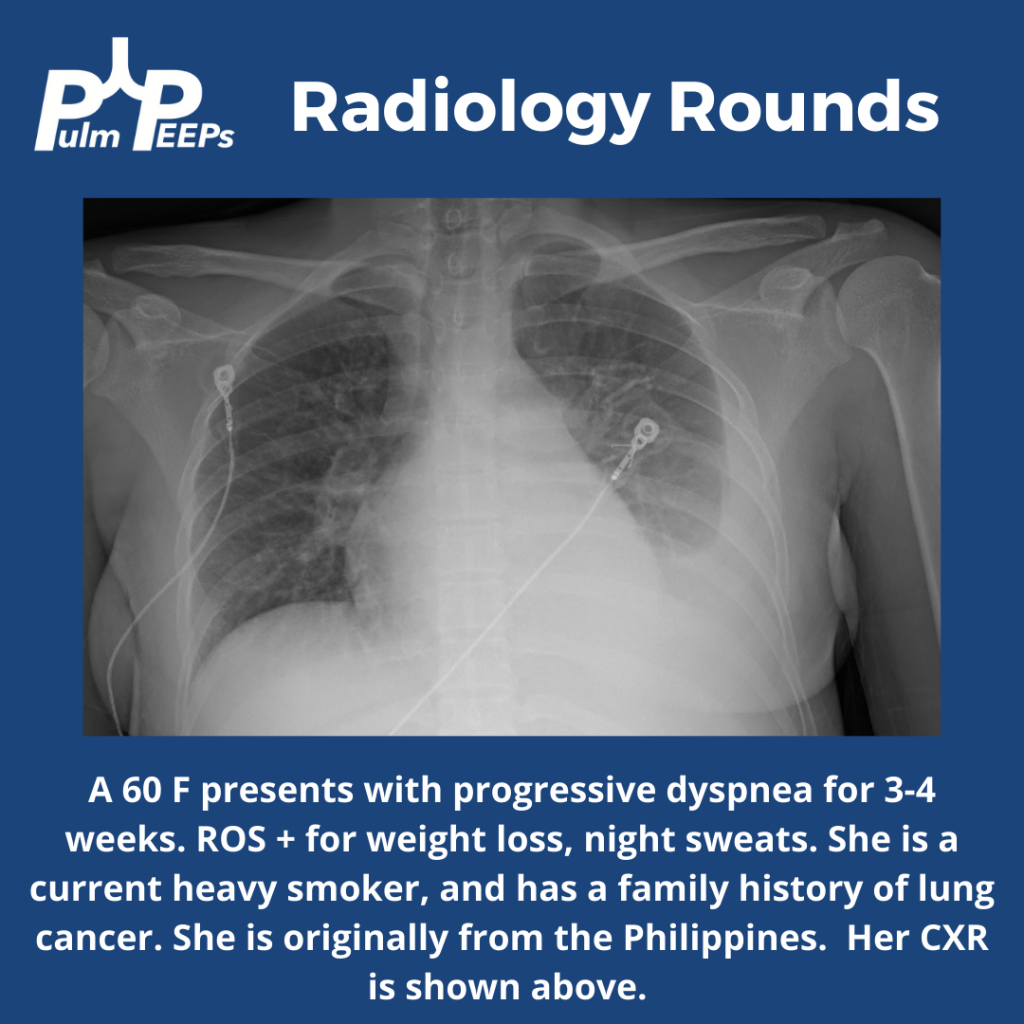
This week’s #RadiologyRounds is coming from the pulmonary clinic. Follow us on Twitter to see the case and answer our polls live!
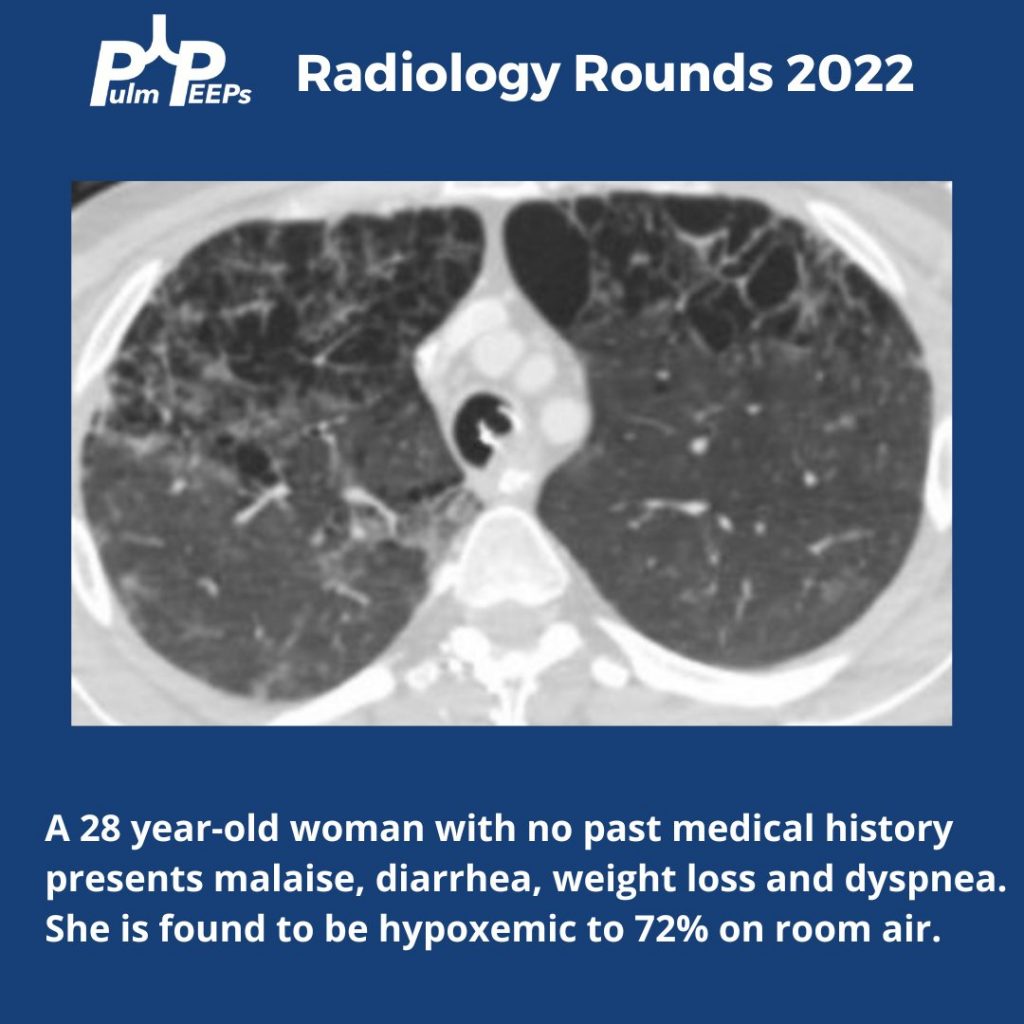
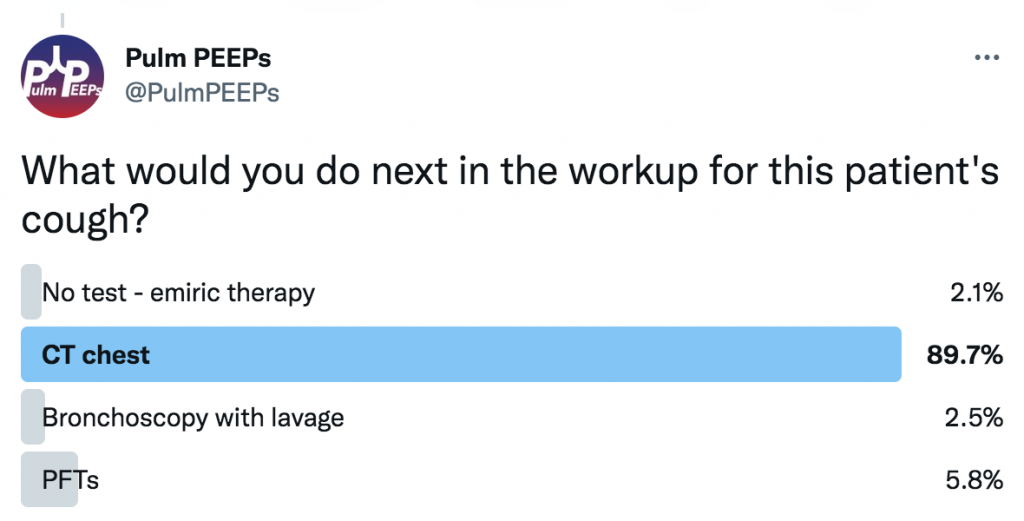
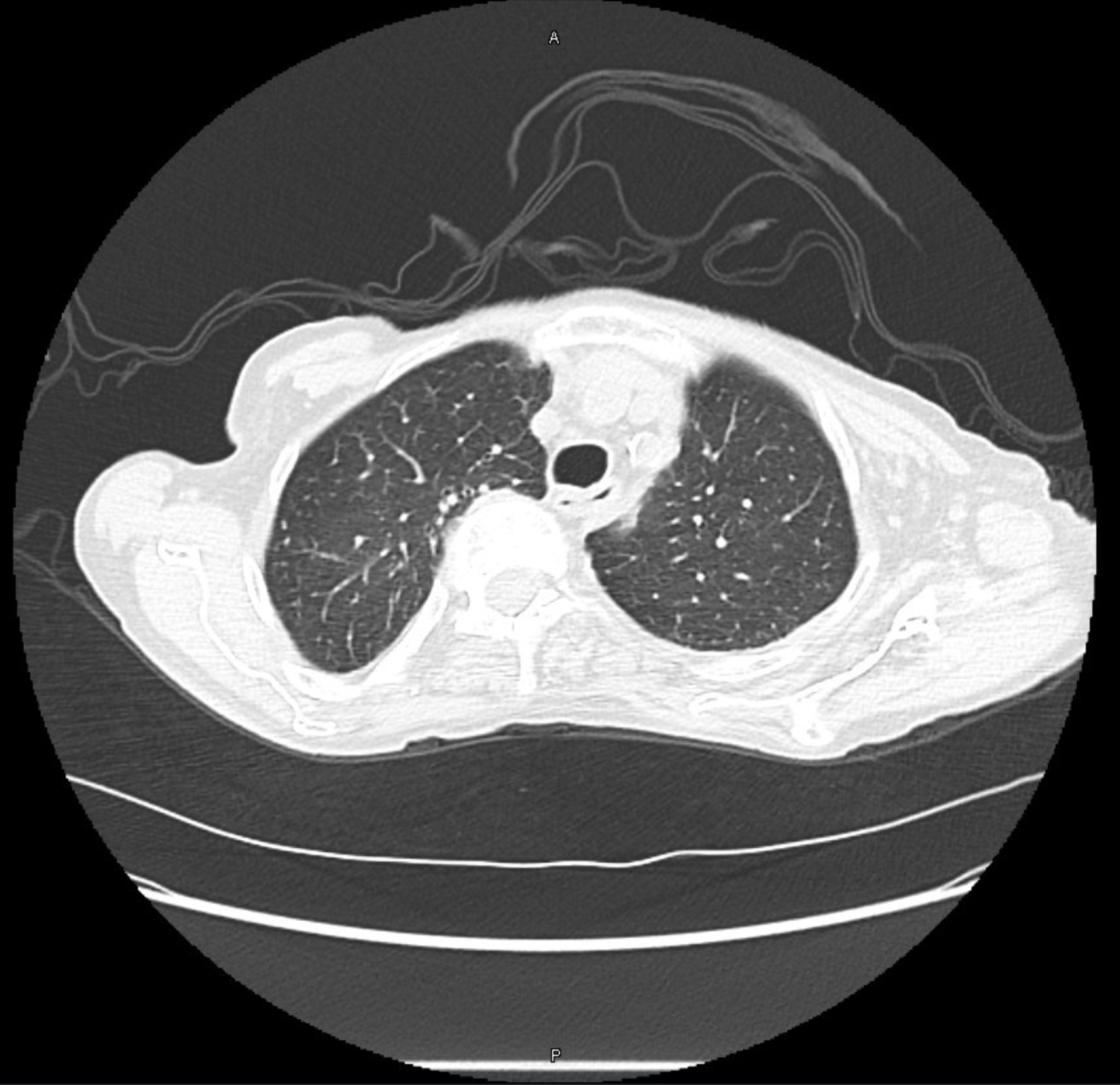
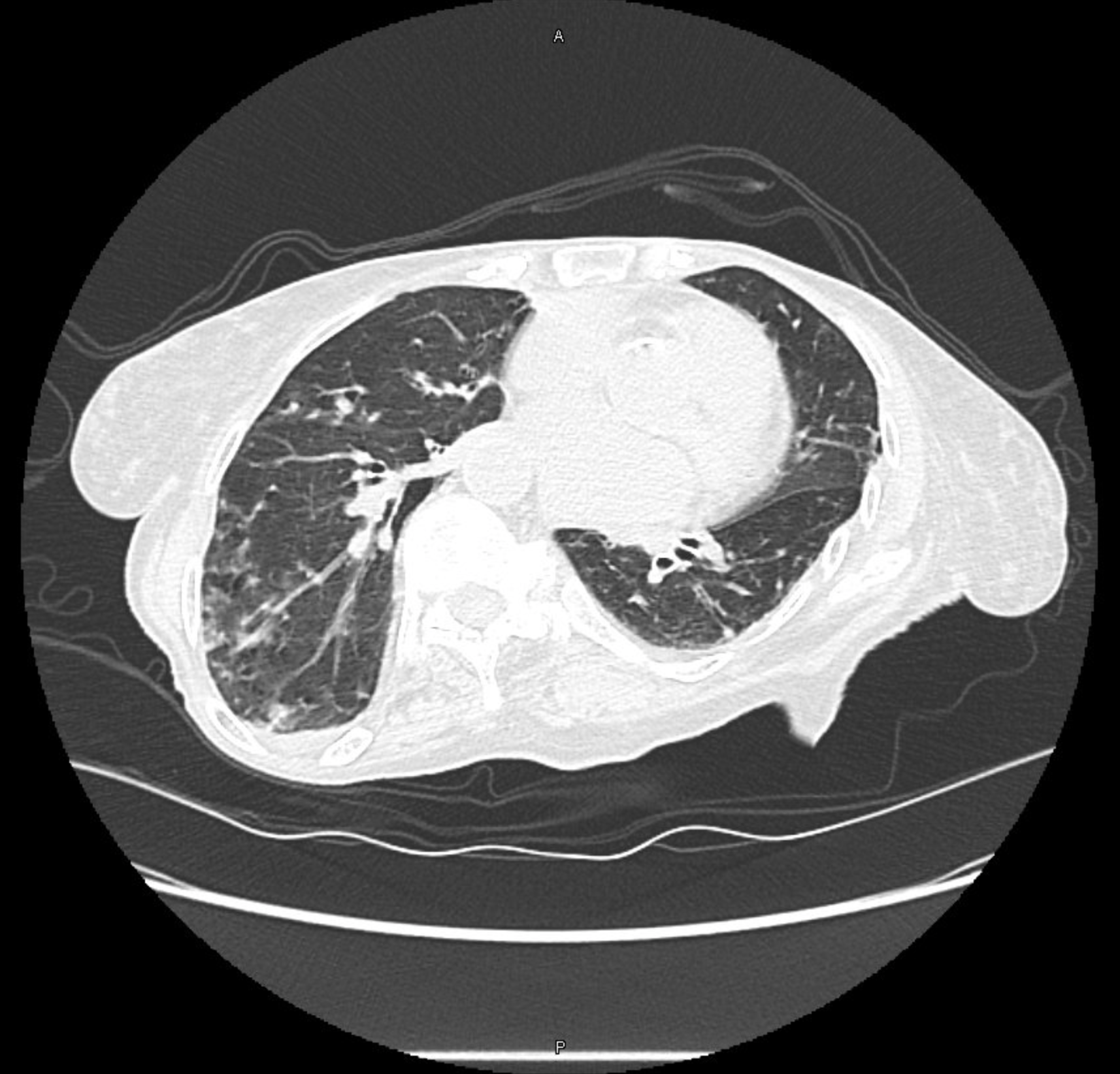
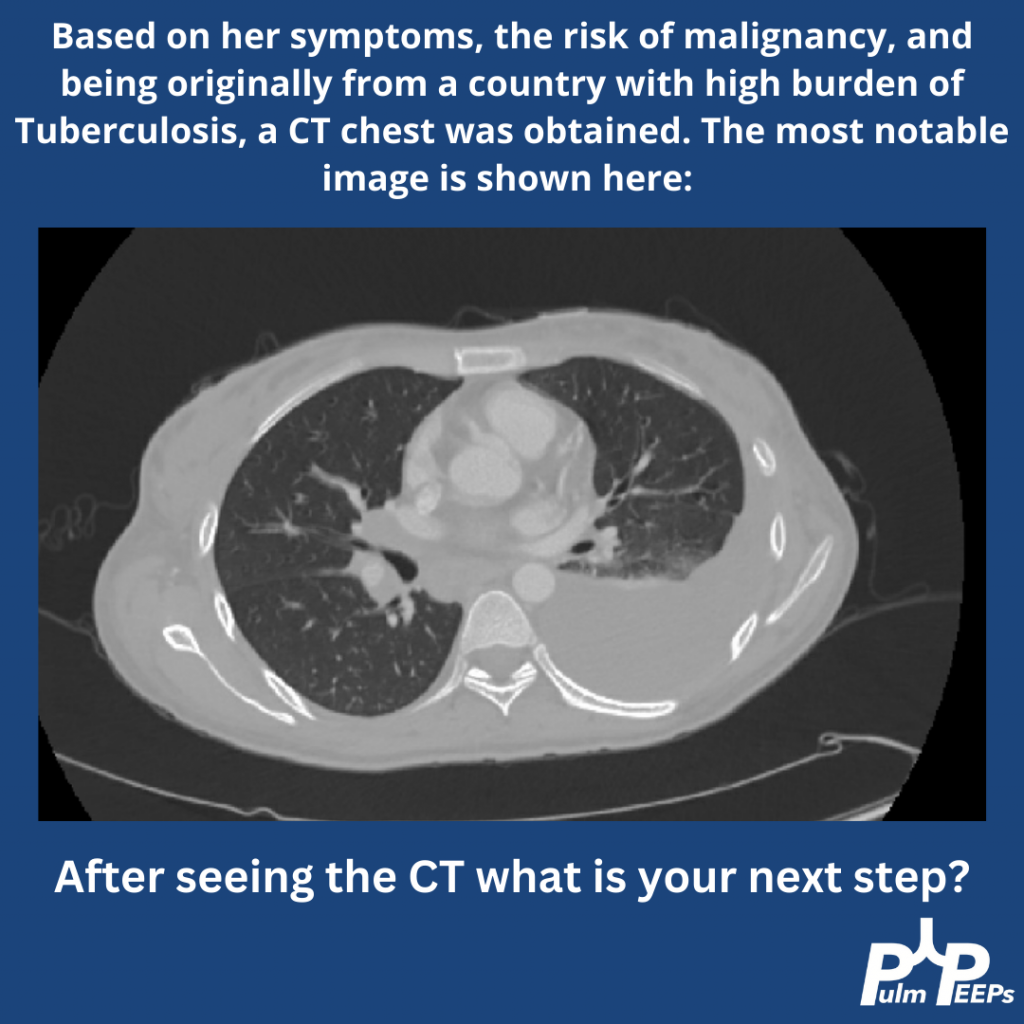
Given the patient’s weight loss and persistent symptoms despite trying some empiric therapies, a chest CT was obtained. PFTs were also ordered 🙂
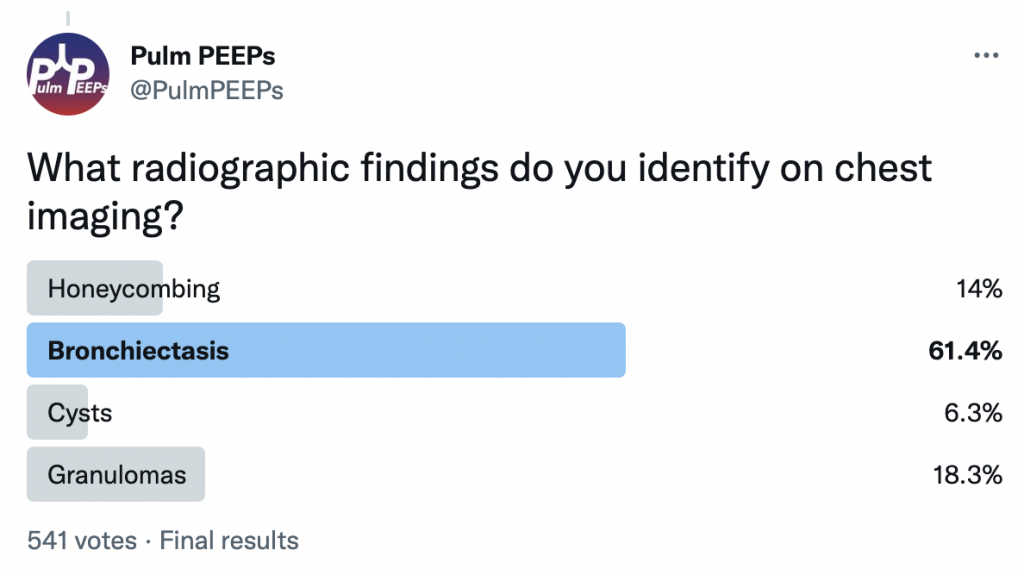
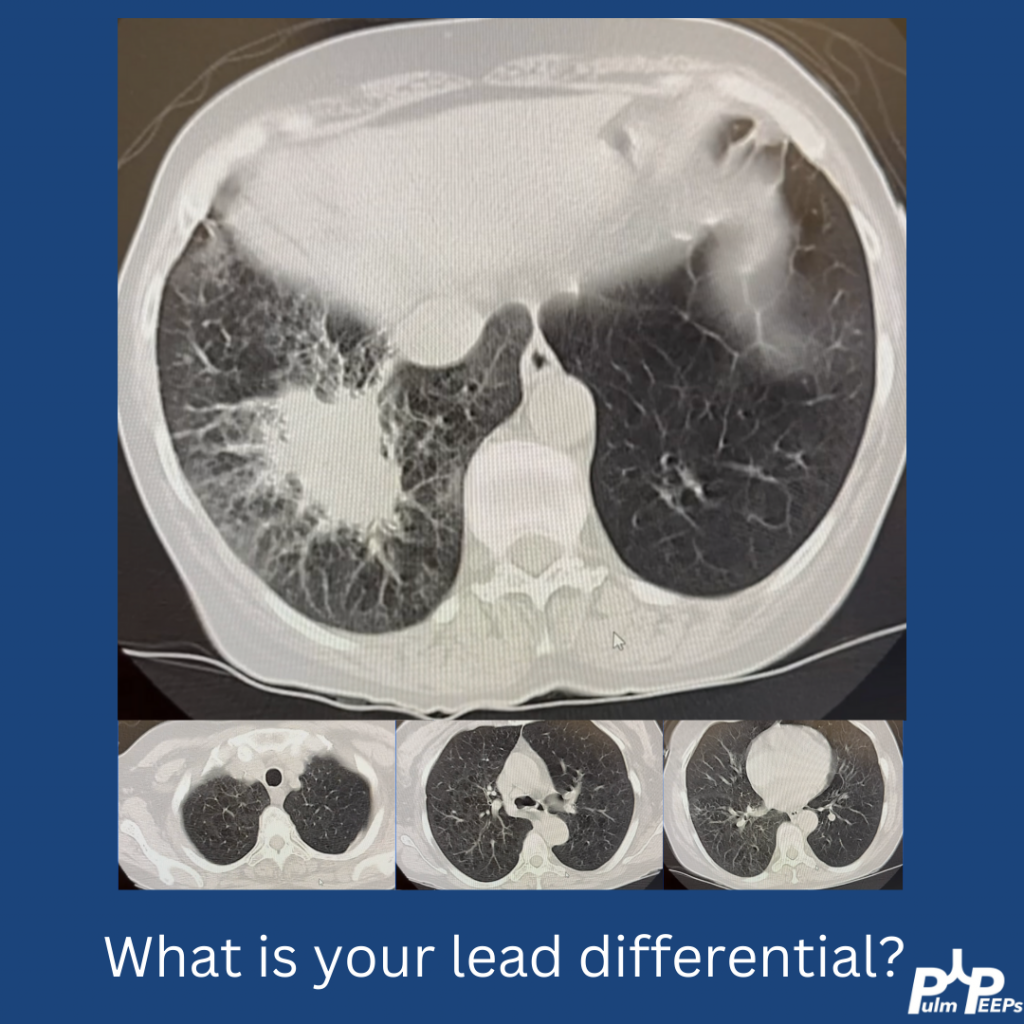
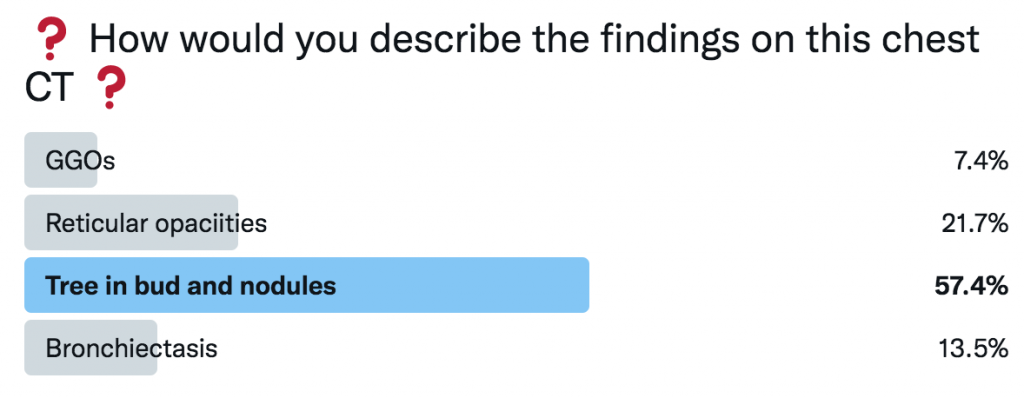
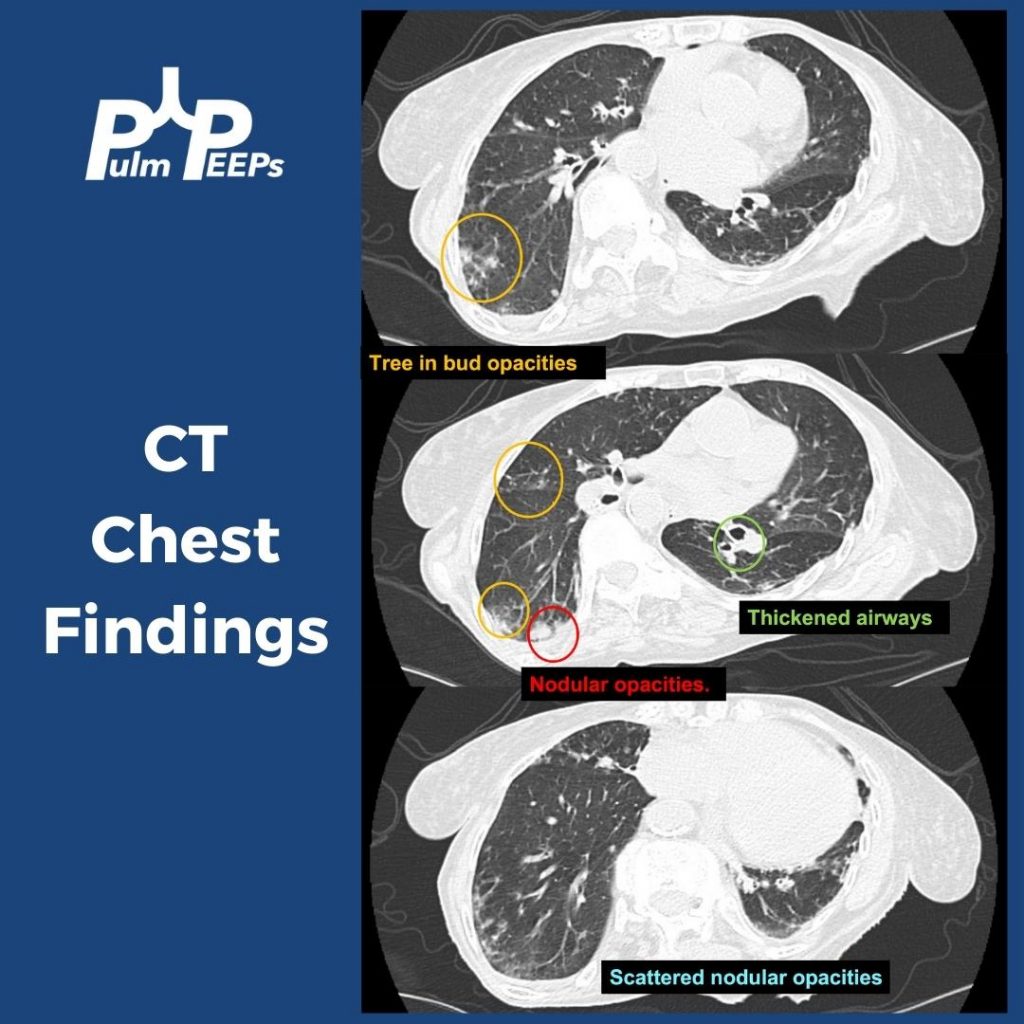
The patient’s CT had tree-in-bud opacities, nodular consolidations, scattered micronodular opacities, and airway thickening.
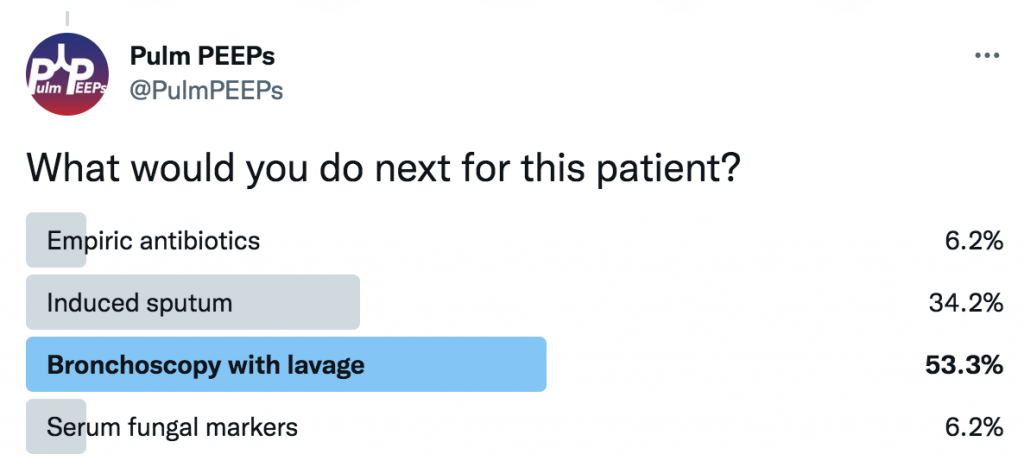
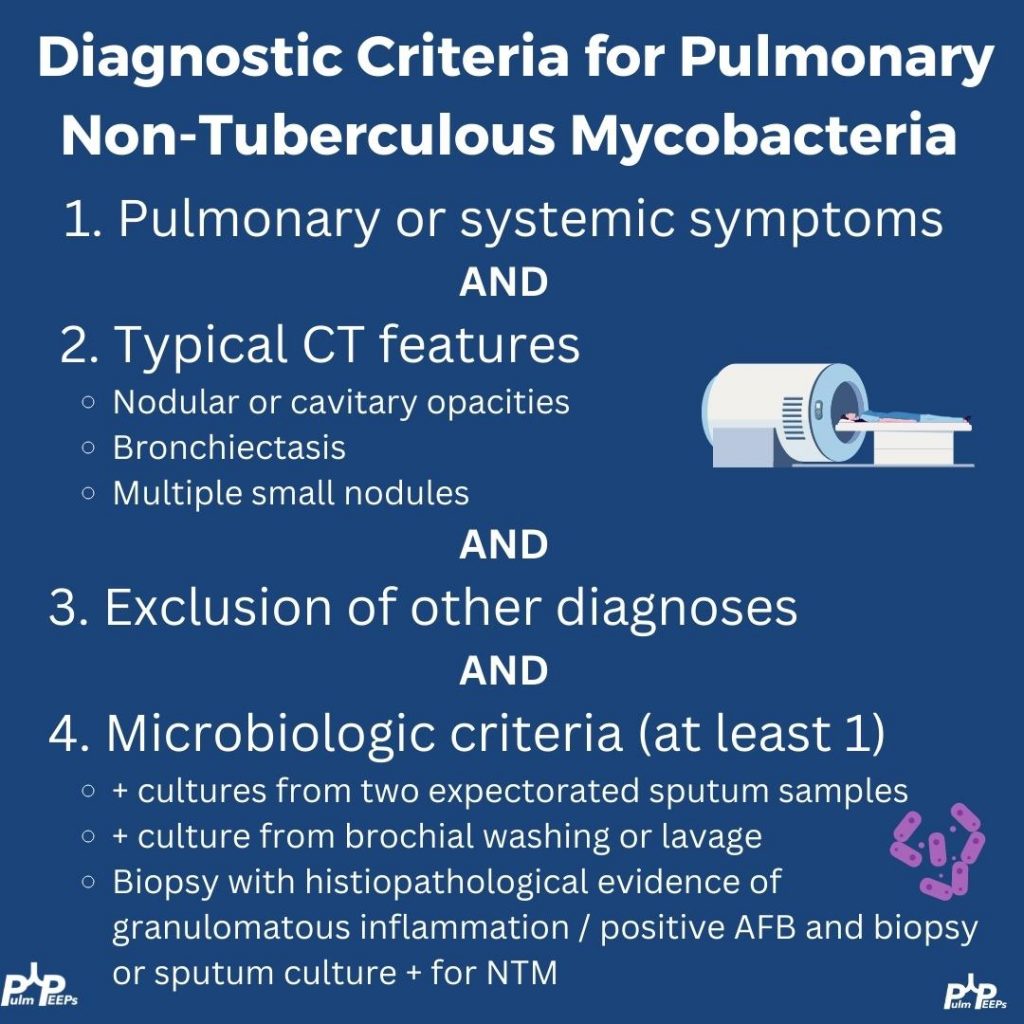
The pt had an induced sputum but could not produce a sample. She underwent bronchoscopy + lavage and her AFB smear was positive with negative TB NAAT. The culture ended up growing M. chimaera! Does that explain her symptoms? Here are the diagnostic criteria for pulmonary NTM:
All other testing was negative and the patient was diagnosed with pulmonary NTM. After a long discussion about treatment (an interesting topic for another day!!) she was started on triple antibiotic therapy and after 9 months her cough had resolved and she was gaining weight.
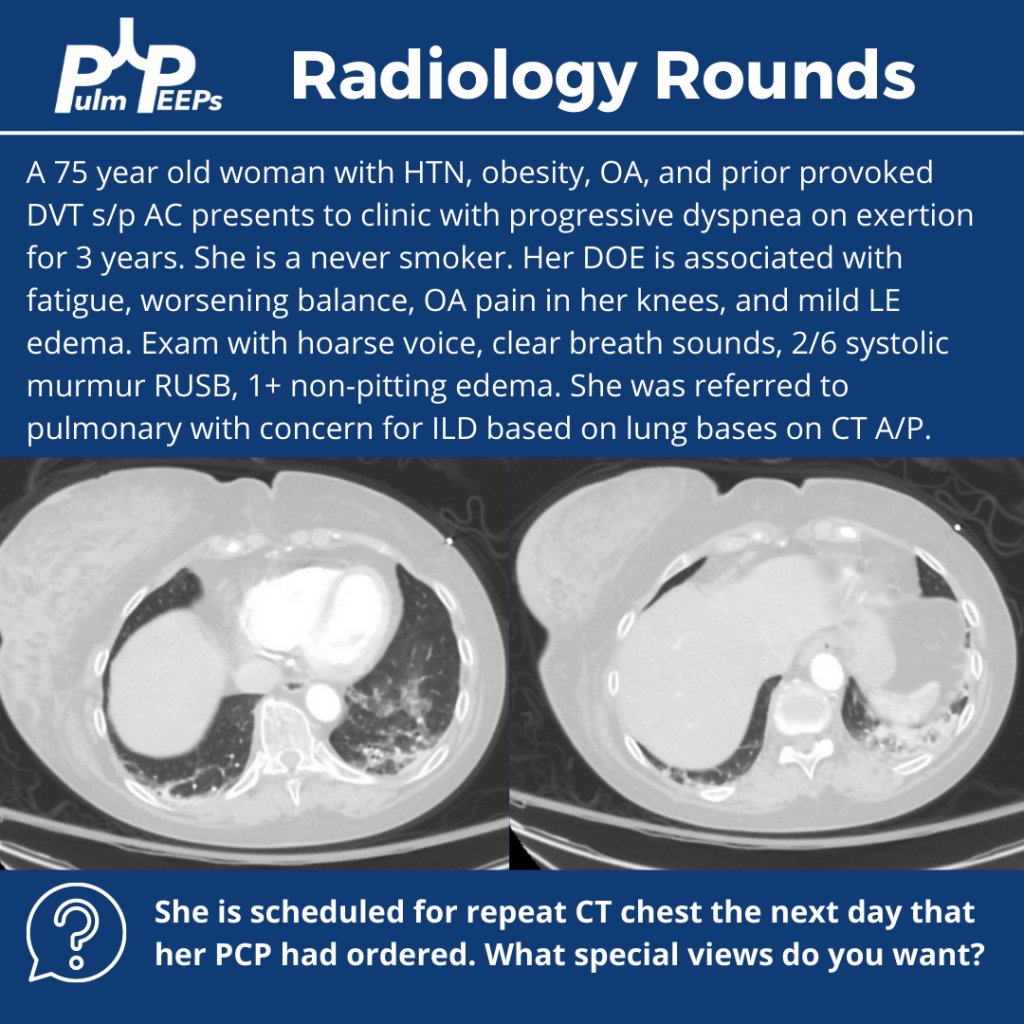
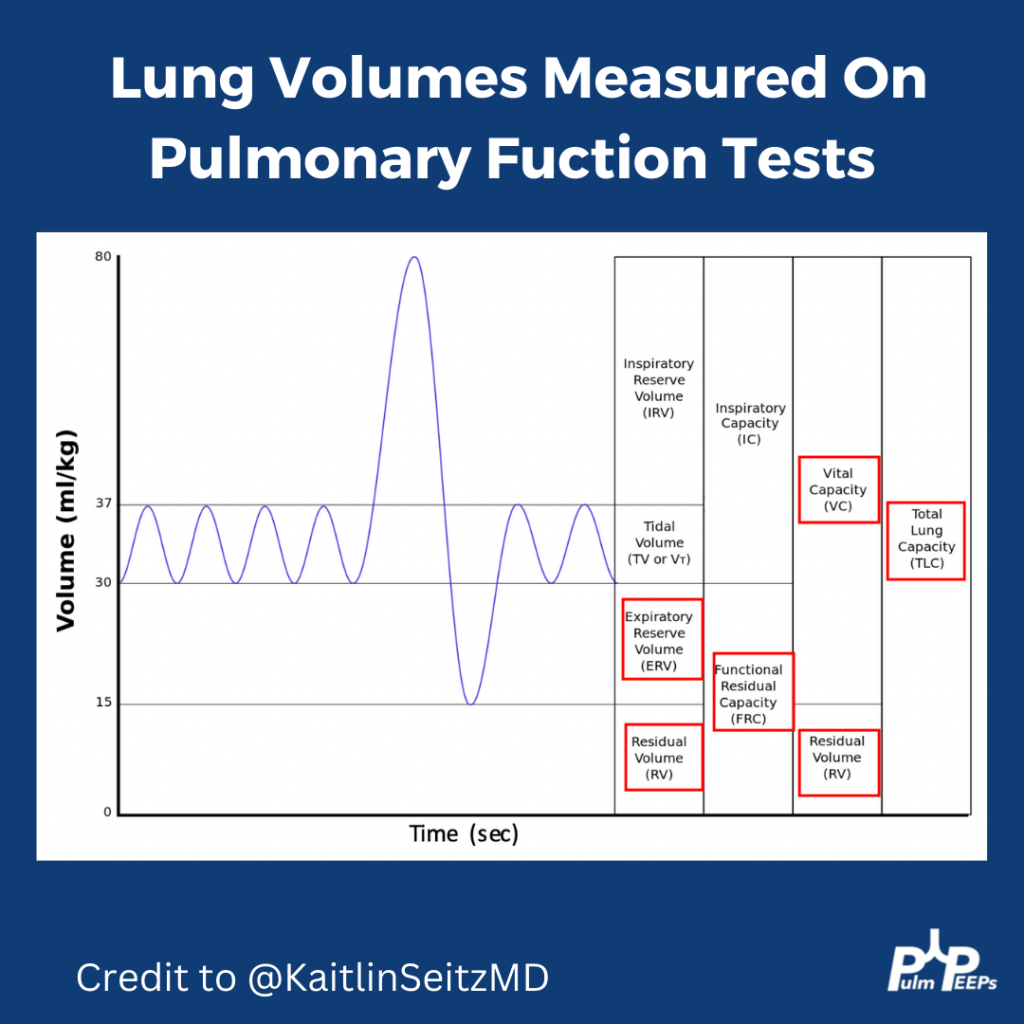
For #RadiologyRounds this week we have a mystery case from the pulmonary clinic complete with imaging and exploration of PFTs. Follow along for some great clinical pearls and teaching points about lung function tests. Graphics made with the help of outstanding educator Kaitlin Seitz.
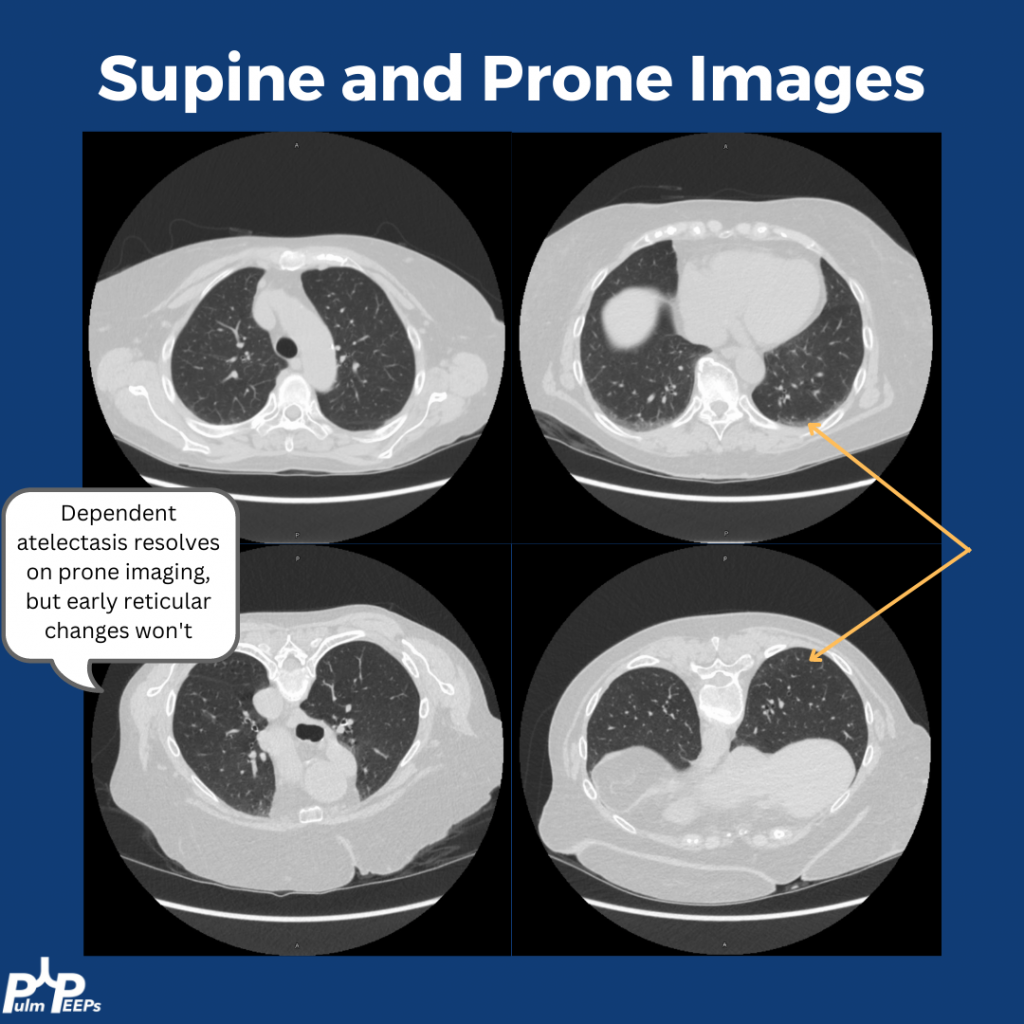
What imaging views would you get next?
A) Supine and prone
B) Inspiratory and expiratory
C) High resolution
D) With contrast
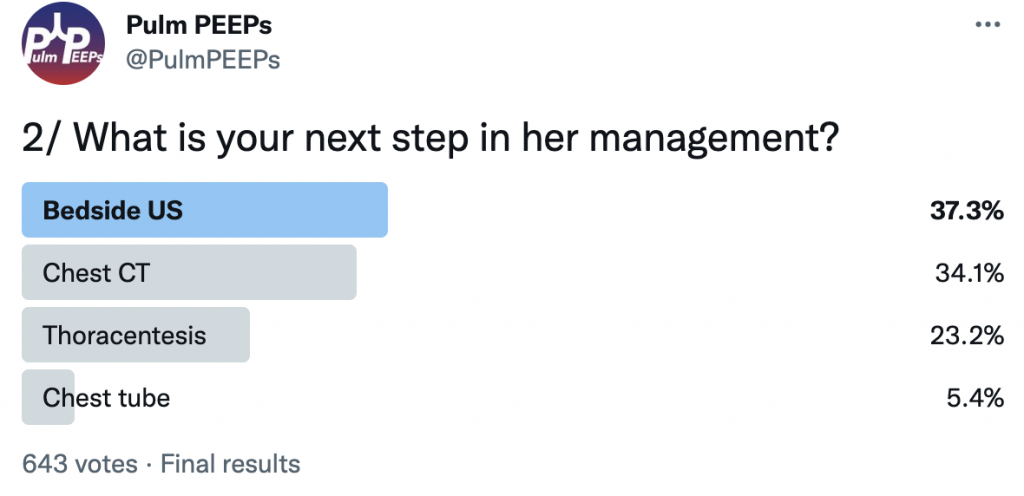
What test would you get next?
A) Bronchoscopy
B) ECHO
C) PFTs
D) Lung US
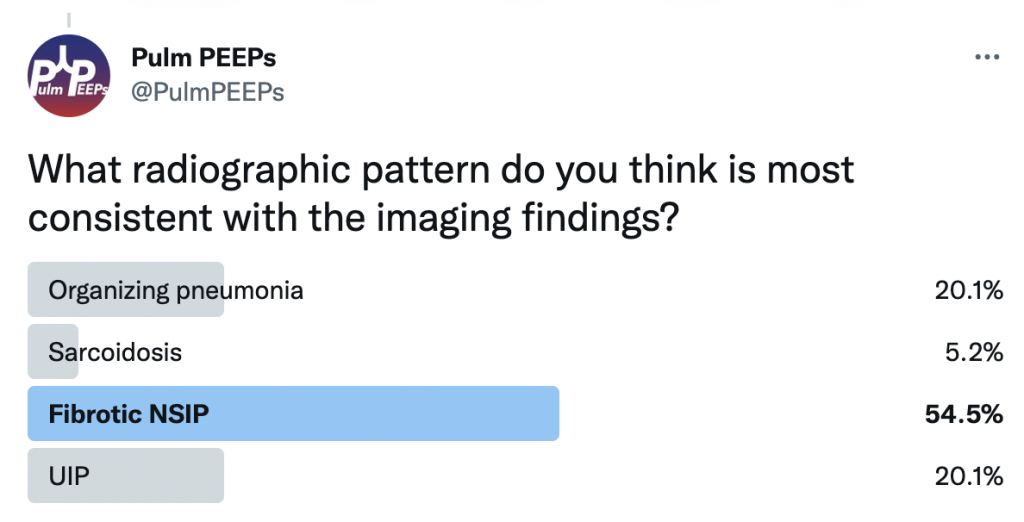
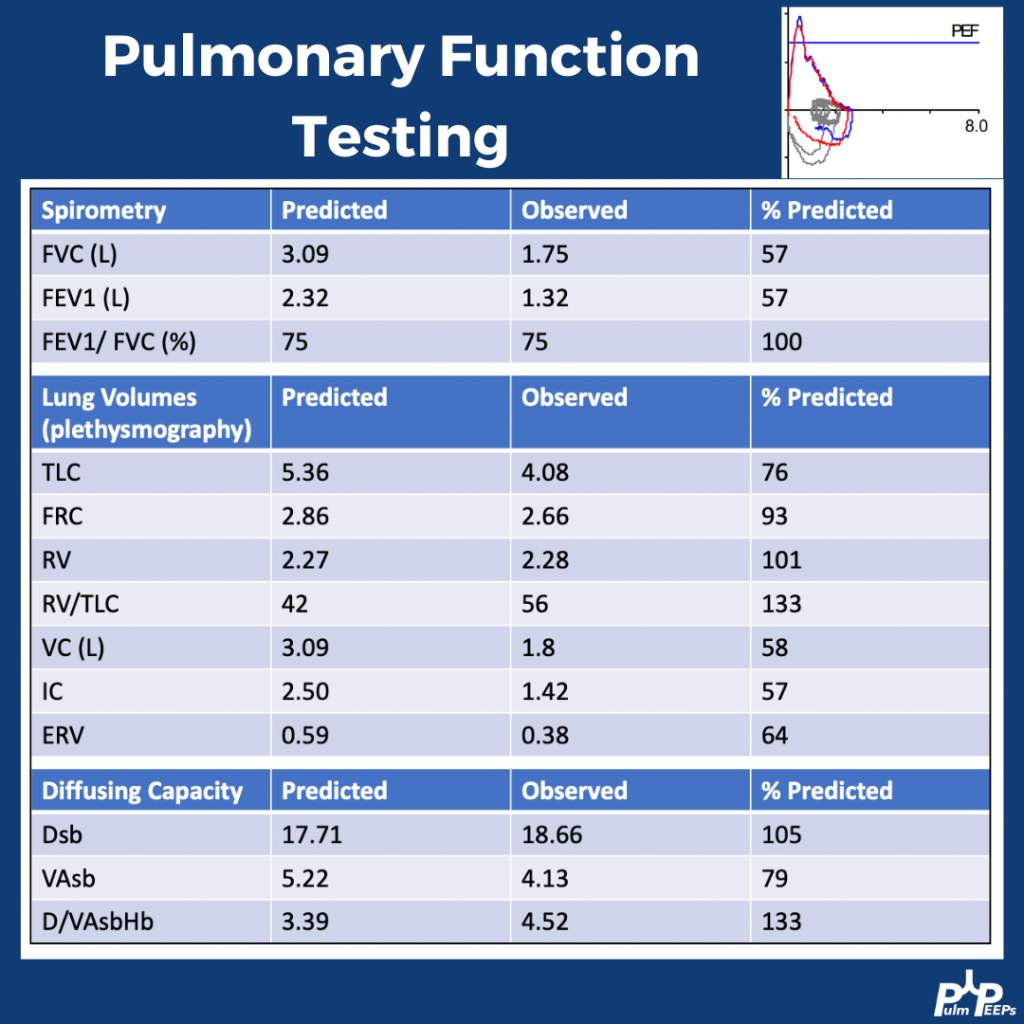
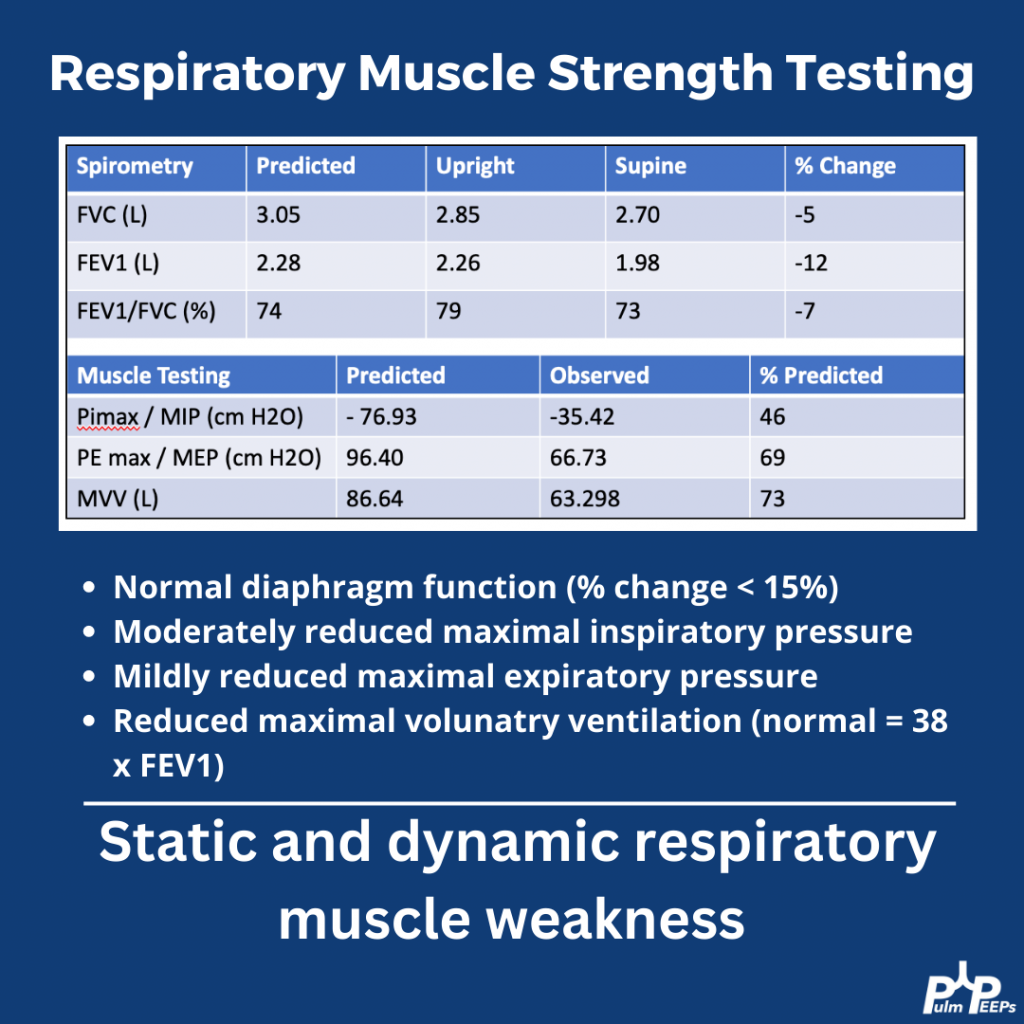
What do these PFTs show?
A) Restriction concerning for ILD
B) Restriction concerning for obesity
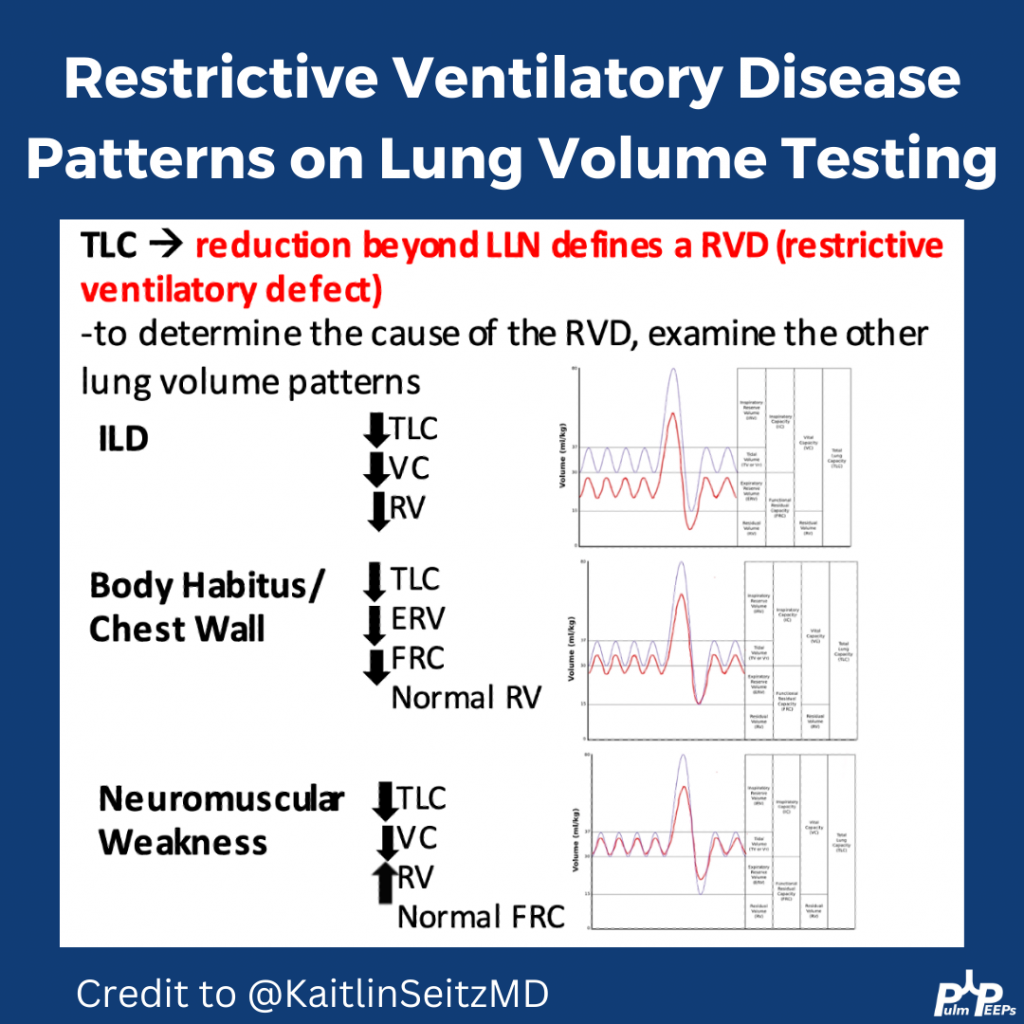
C) Restriction concerning for weakness
D) Mixed obstruction and restriction
The patient was referred to neurology and ultimately diagnosed with severe mixed sensory and motor chronic axonal polyneuropathy.
This week’s #RadiologyRounds and tutorial is authored by Huzaifah Salat, our newest PulmPEEPs contributor! See if you can figure out the case and check out our high-yield points at the end. Follow us on Twitter to answer live polls about the case.