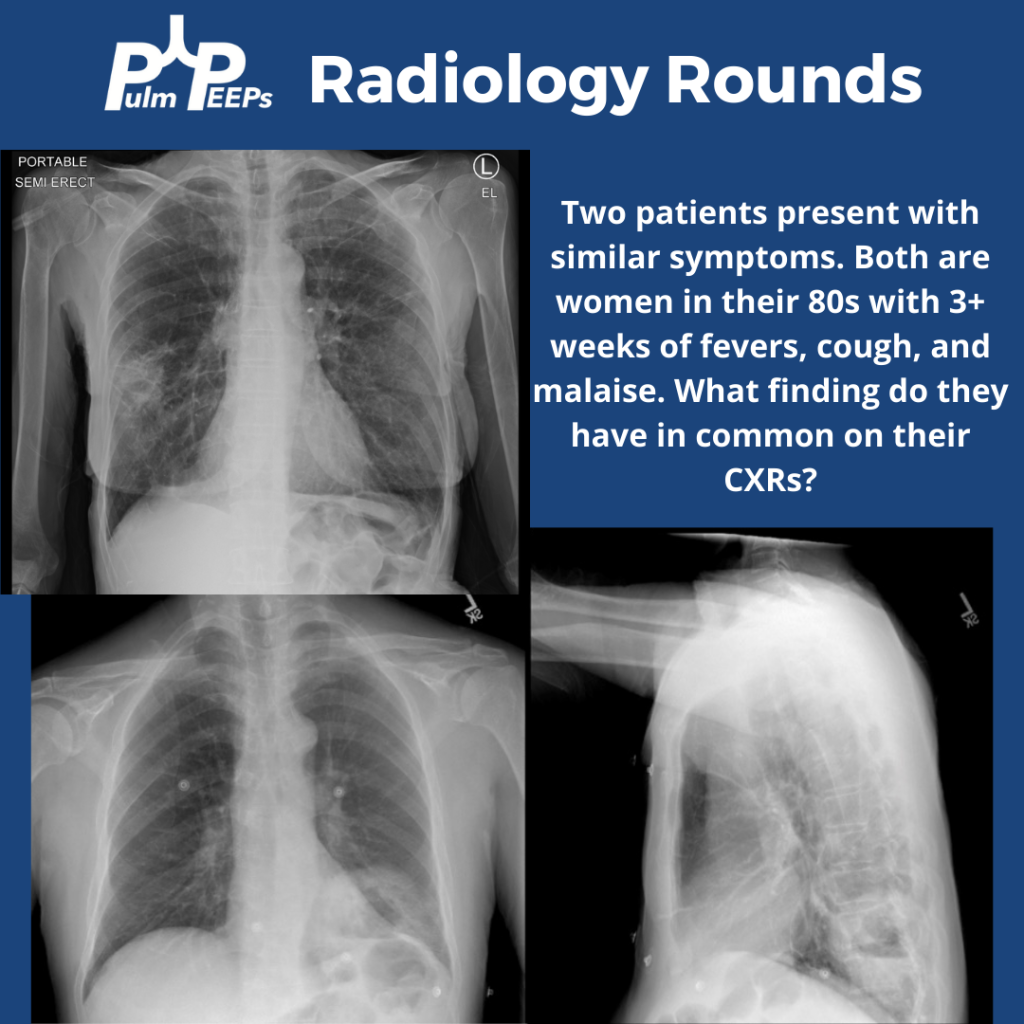
Tuesday is time for another #RadiologyRounds! Time for some CXR reading and a differential diagnosis mnemonic Two women presented to the hospital with similar presentations. They are both in their 80s with multiple weeks of cough, fever, and fatigue. Here are the CXRs
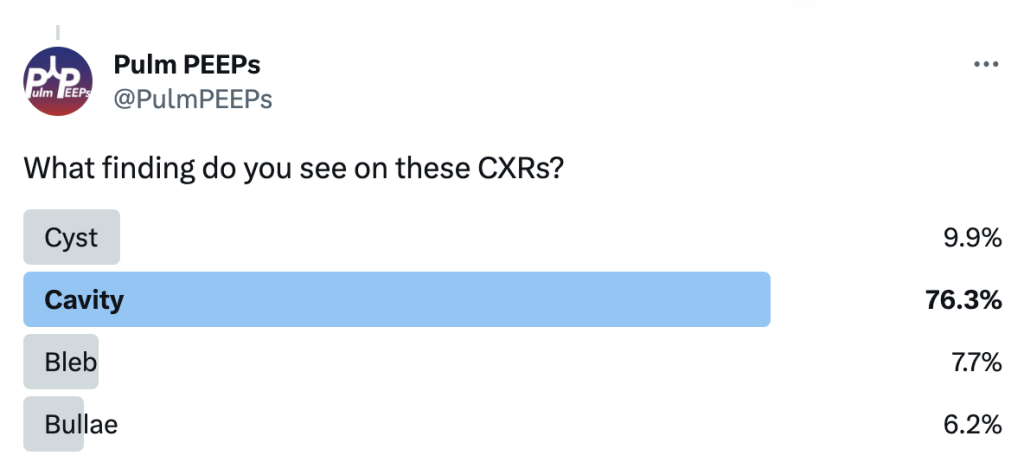
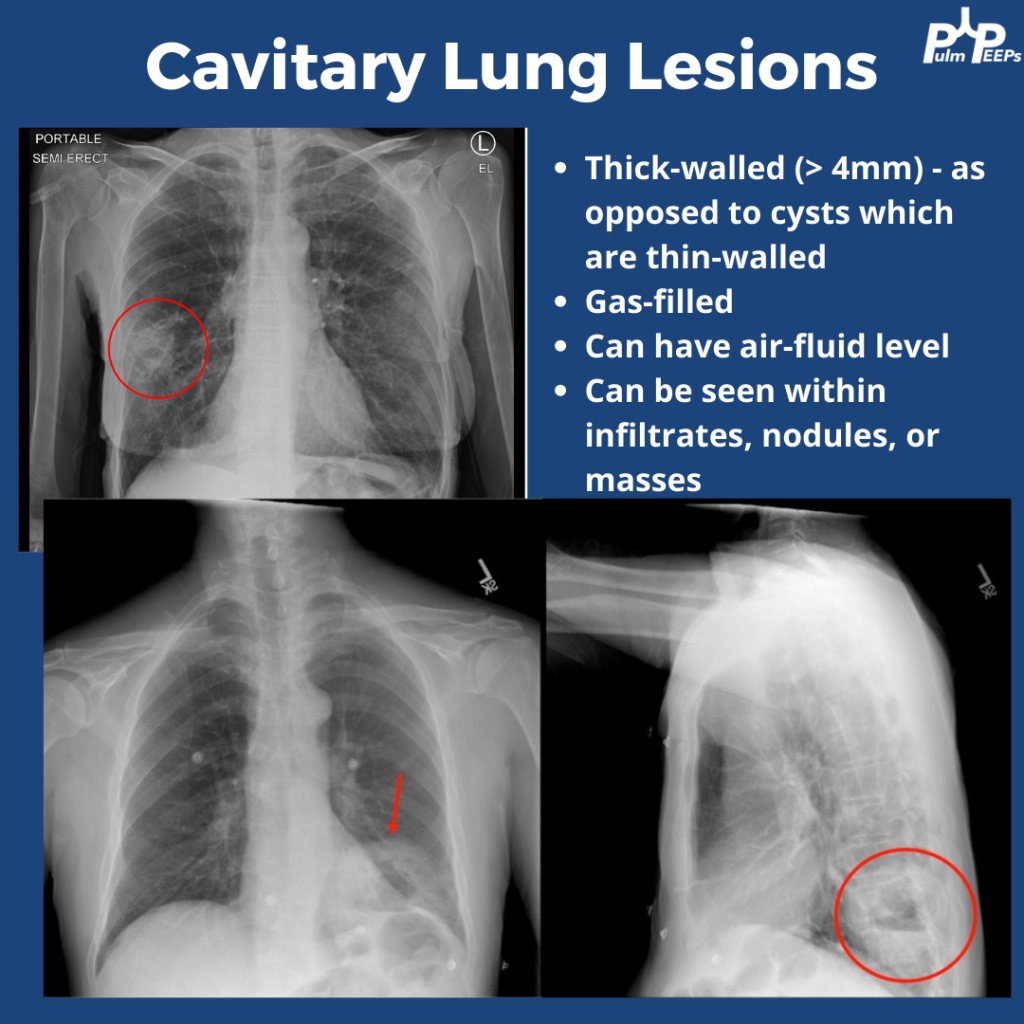
The CXRs both showed cavities. They are thick-walled (>4mm) and gas-filled. Cavitary lung lesions are seen within infiltrates, nodules, or masses. There can be an air-fluid level within the cavity. Cysts have thinner walls. The findings were confirmed on CT scan
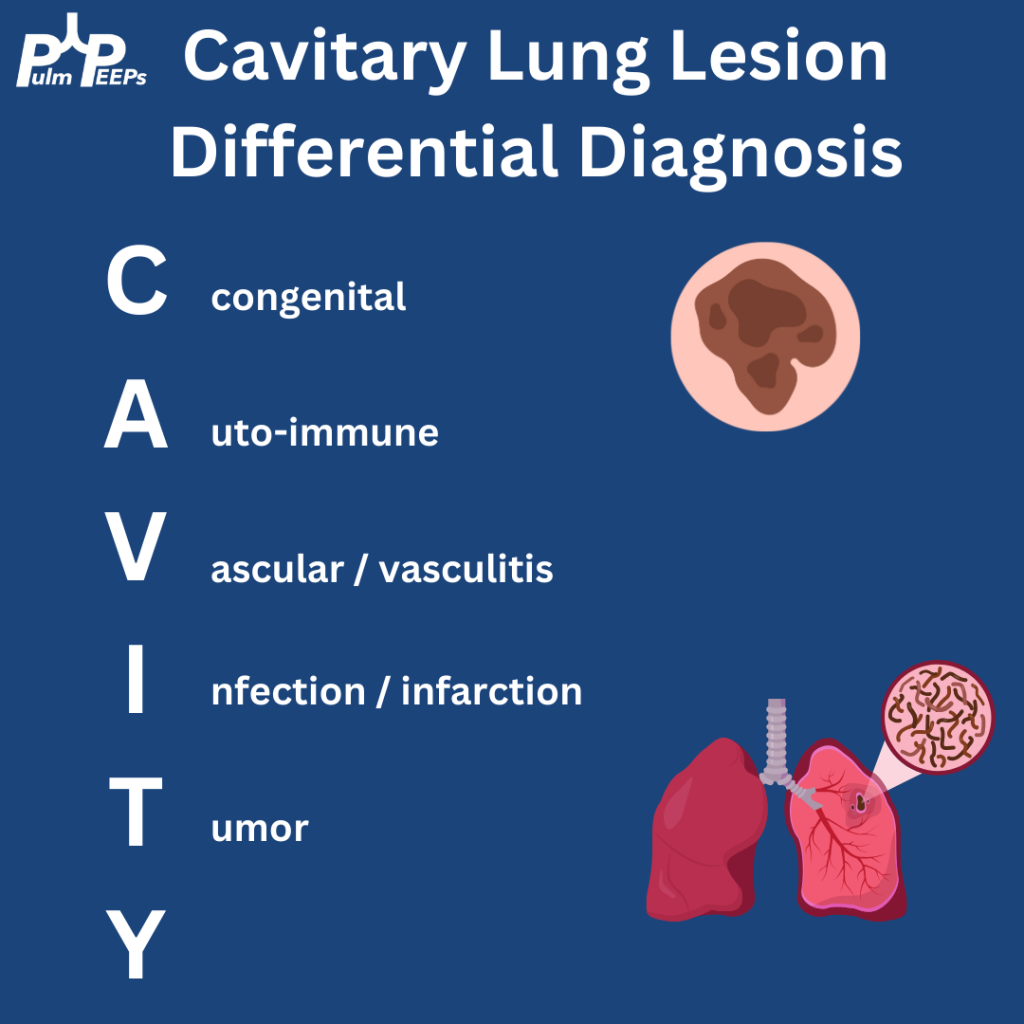
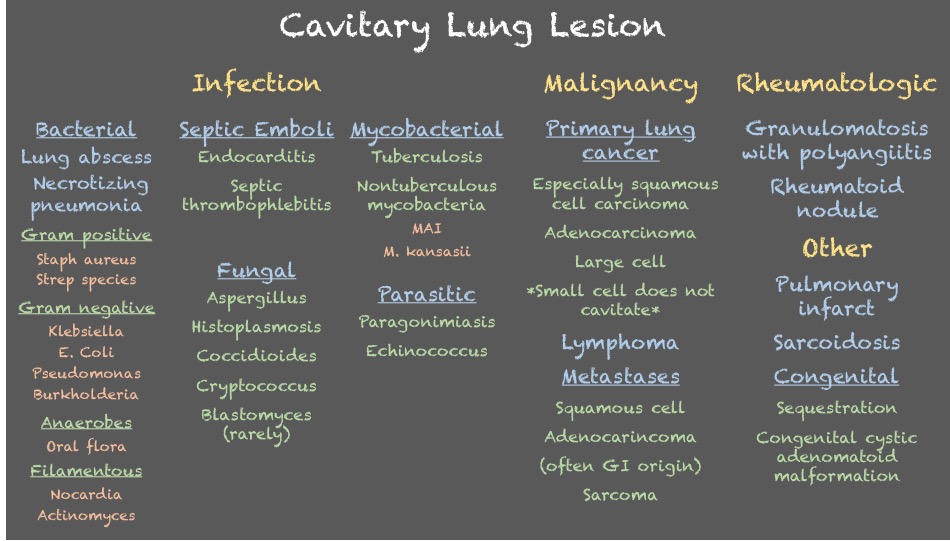
Cavitary lung lesions can have a broad differential so it is helpful to have a systematic approach. To make it easy, when you see this just remember: CAVITY
Bonus points to anyone who can fill in the Y
Both patients were ultimately diagnosed with pulmonary abscesses which improved with prolonged courses of antibiotics with anaerobic and gram-negative coverage.
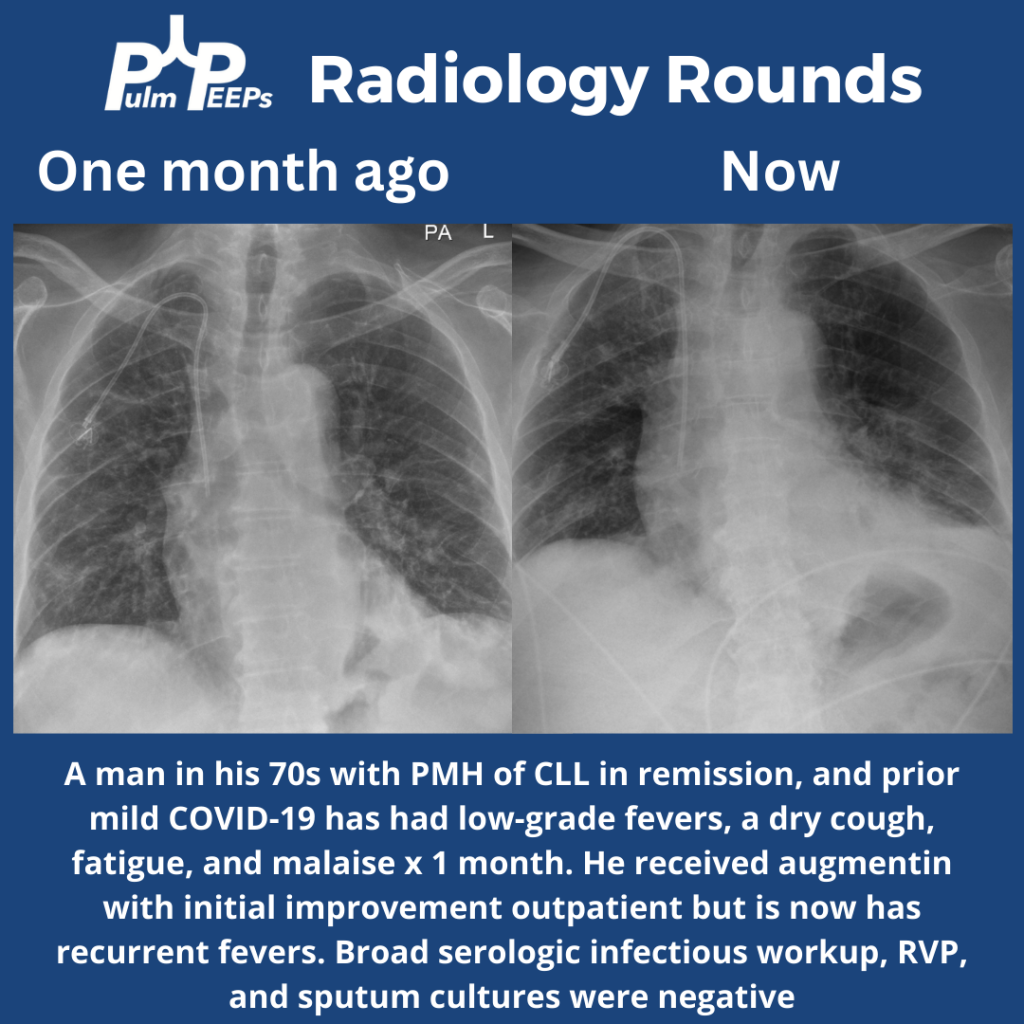
Time for #RadiologyRounds! This week we have a man in his 70s with CLL s/p treatment now in remission. He had fevers, a dry cough, and malaise that initially improved outpatient with antibiotics but have now recurred.
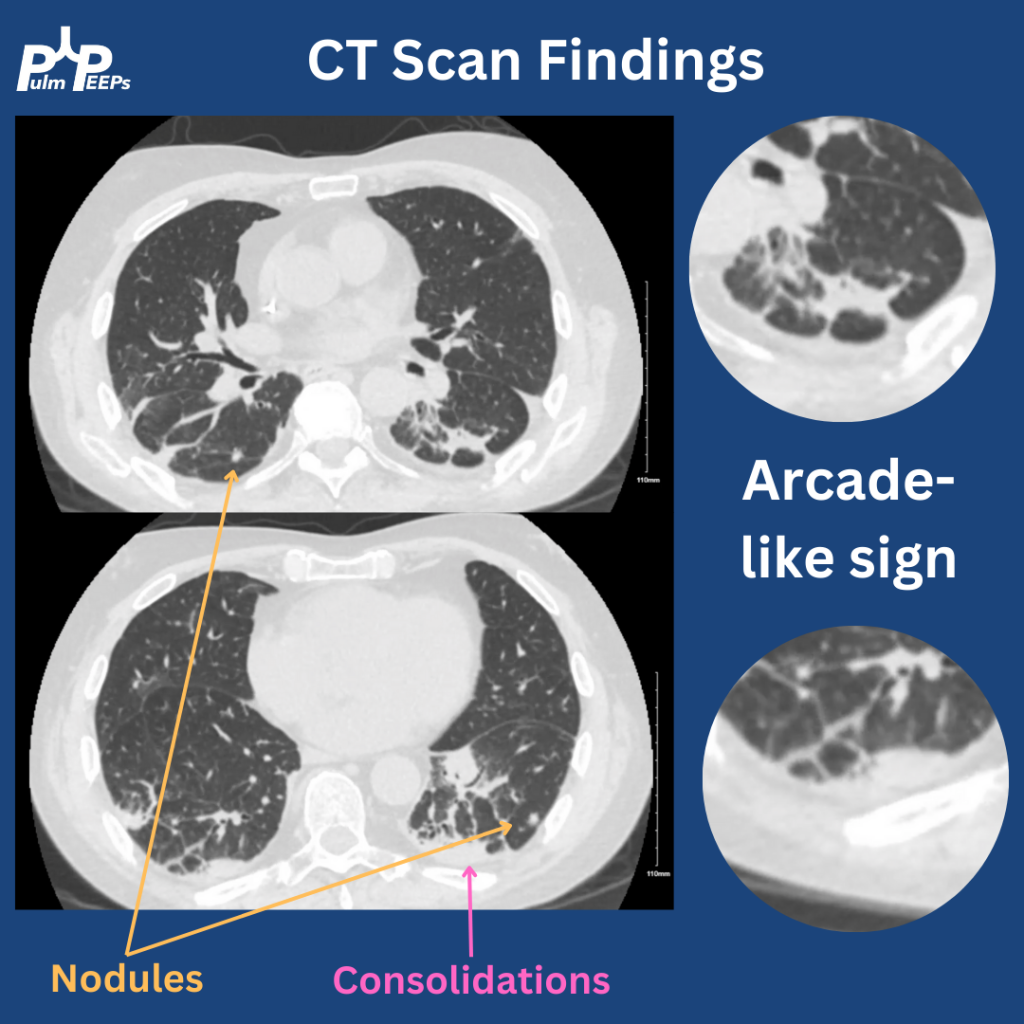
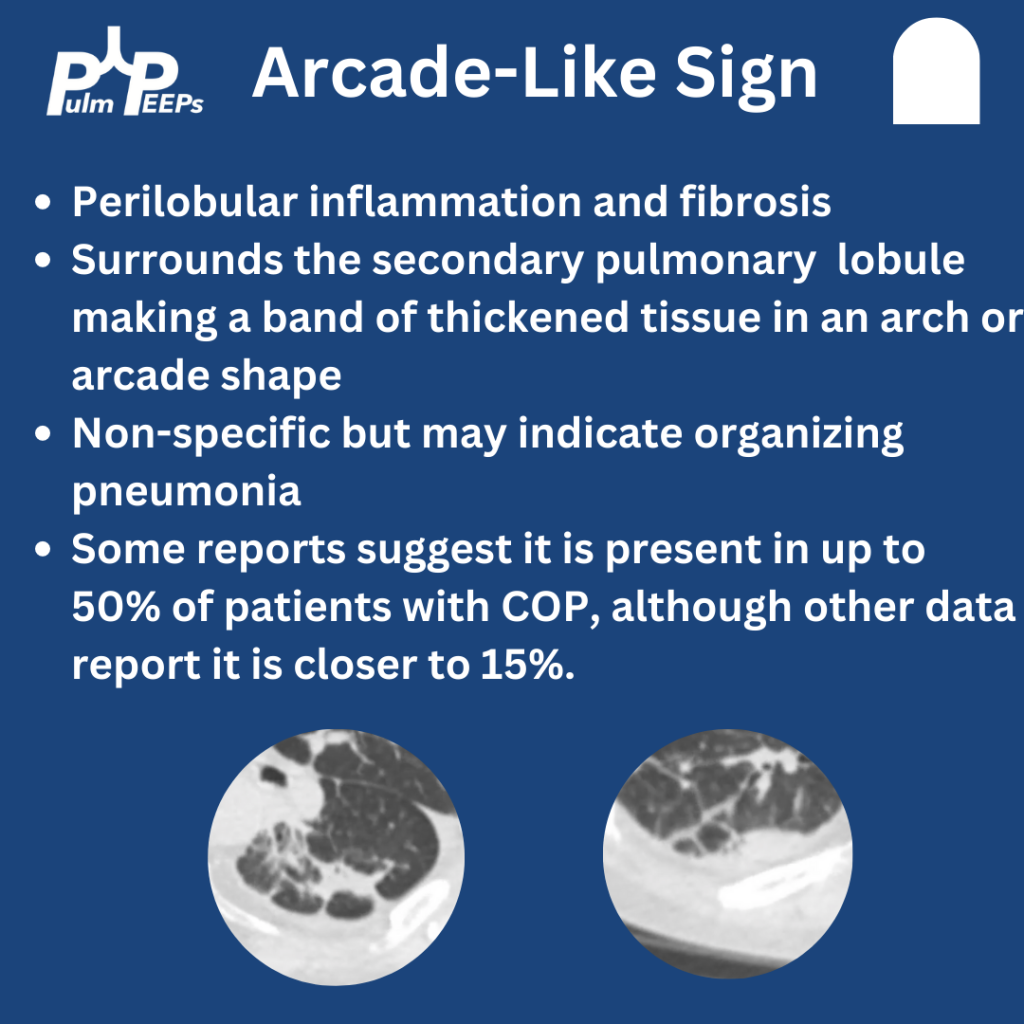
The CT had multiple findings including small nodules, consolidations, and bands of fibrosis around the secondary pulmonary nodules. This is known as Arcade-Like Sign and has classically been described with COP. While it can make you think COP, it has a low sensitivity
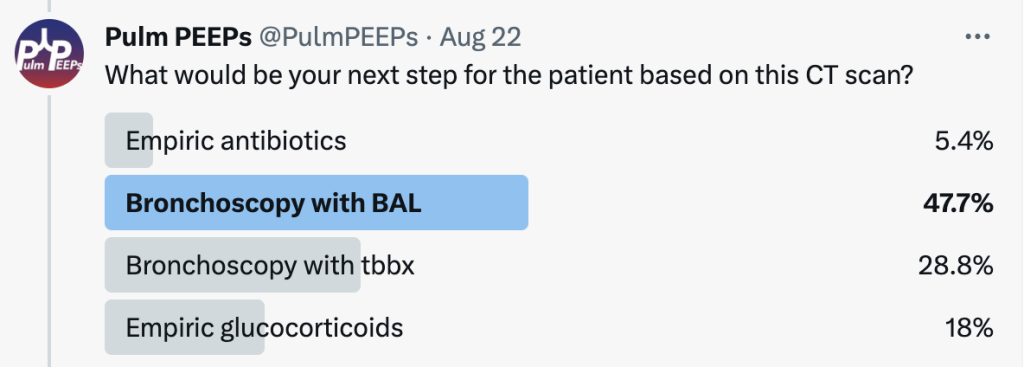
The patient underwent bronchoscopy with Tbbx given the suspicion for OP. The BAL was negative for bacterial, viral, fungal, or mycobacterial infection. The histopathology revealed organizing pneumonia. The patient was started on glucocorticoids and all symptoms improved
Time for another Radiology Round by our Associate Editor Tess Litchman!
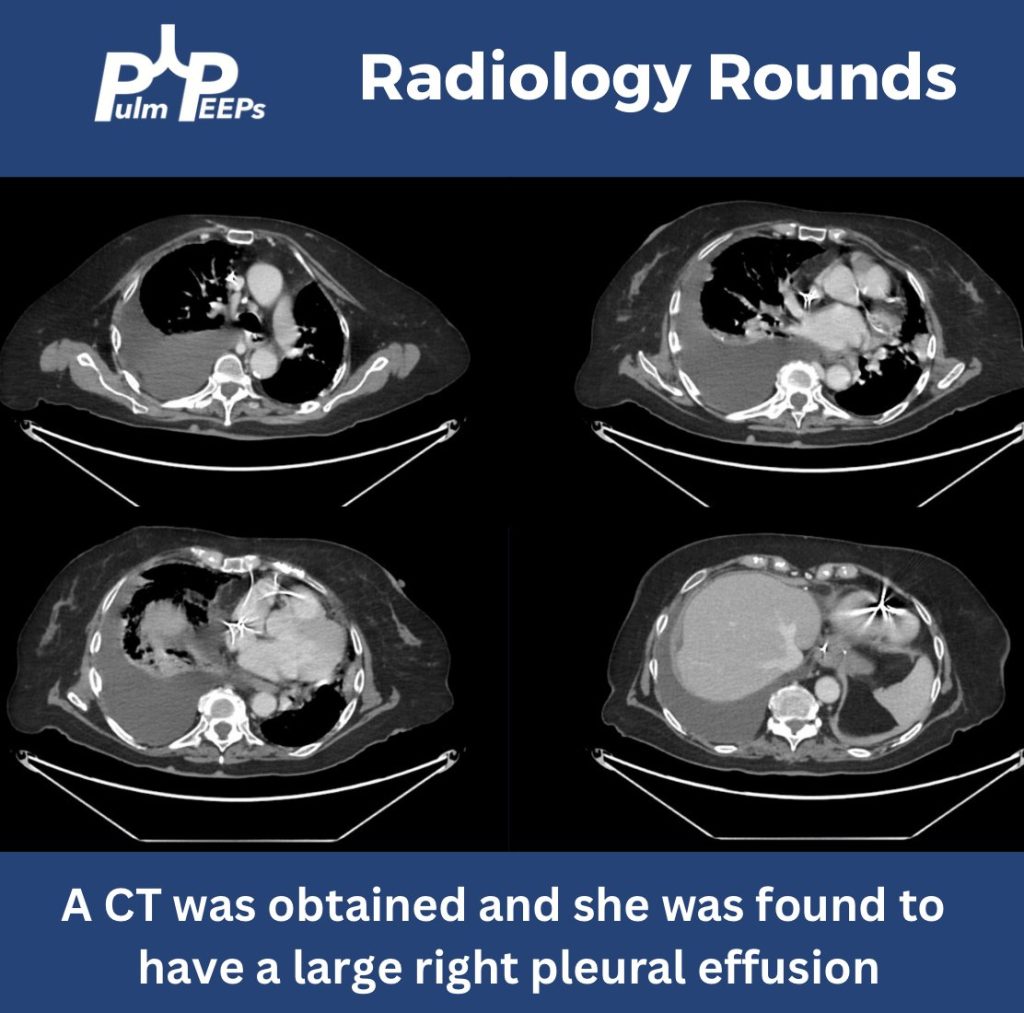
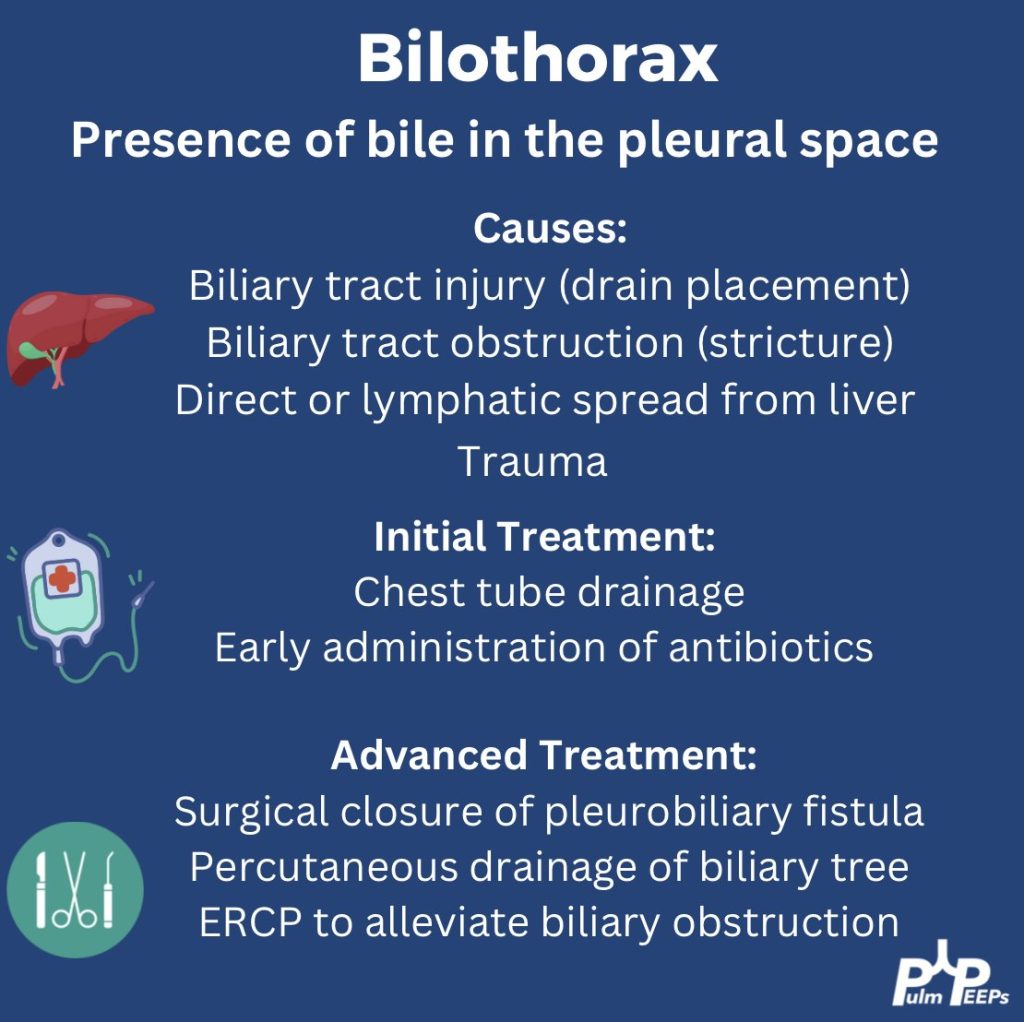
We have an older-aged woman found to have gastric and duodenal ulcers requiring multiple abdominal surgeries and transhepatic biliary drainage presenting with respiratory distress
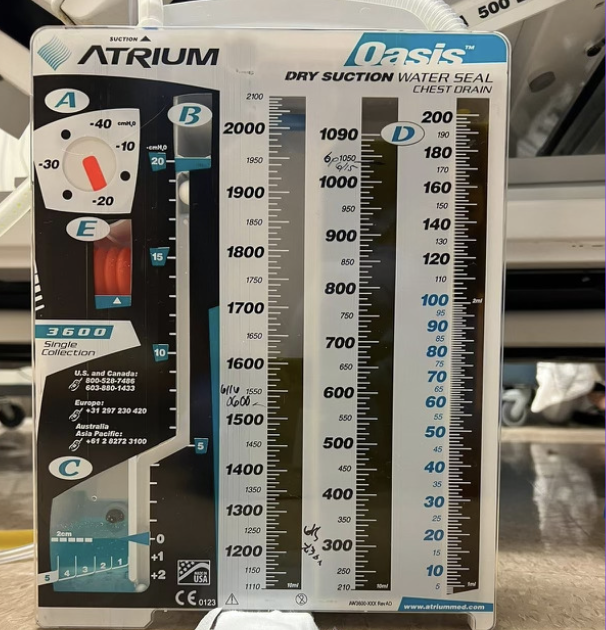
She underwent pleural fluid drainage with the following pleural fluid studies
She ultimately had a right chest tube placed with 1.6 liters of green pleural fluid was drained
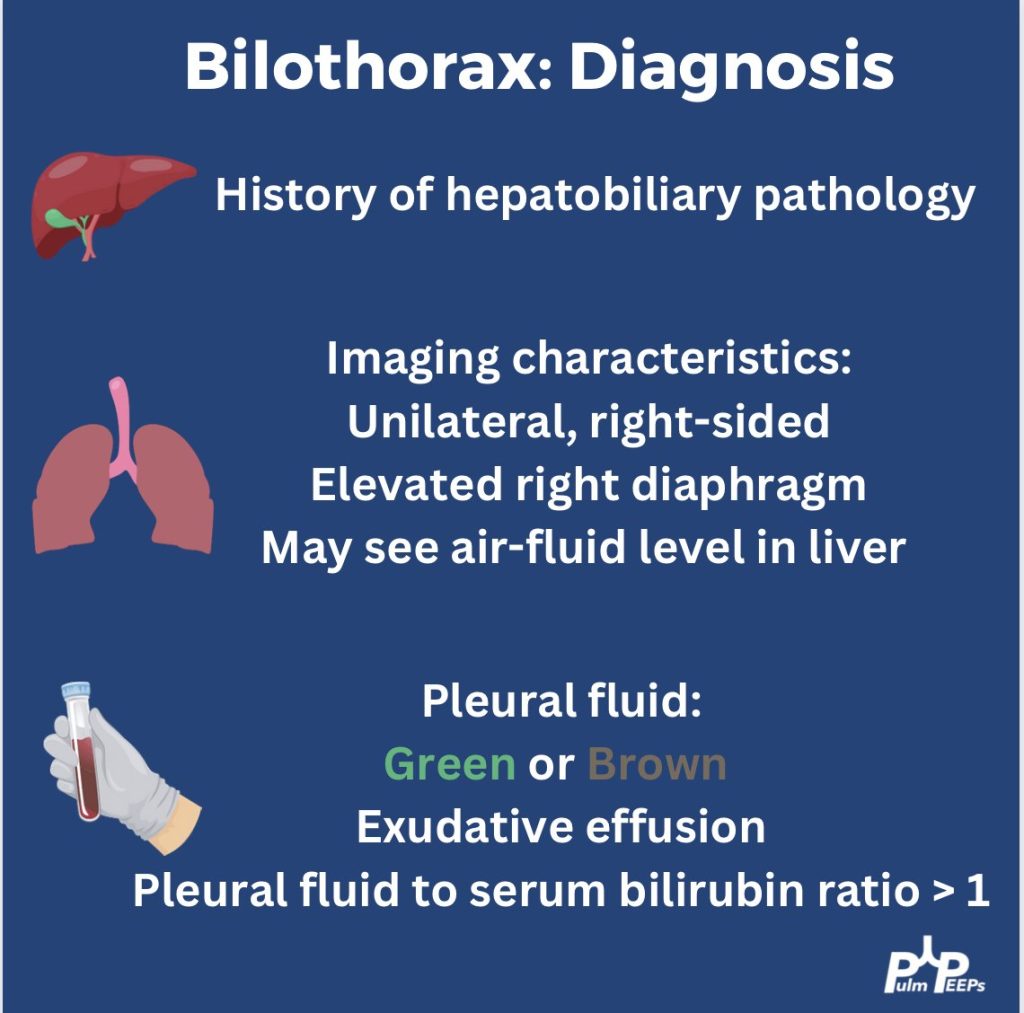
Given concern for a bilothorax, a pleural and serum bilirubin test were added. Her pleural bilirubin level was 17.2 and her serum bilirubin level was 0.5. Her chest tube was maintained, IV antibiotics were started and multi-disciplinary meetings occurred to determine next steps.
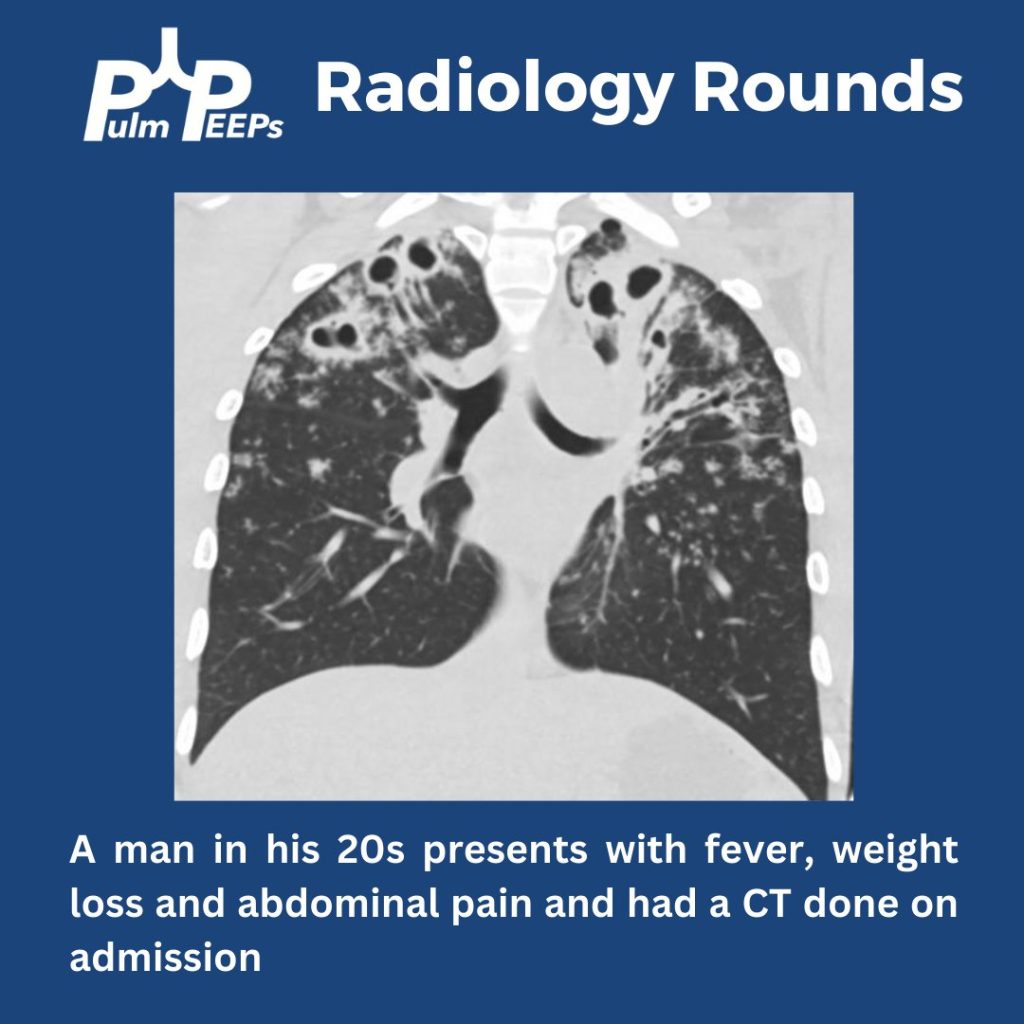
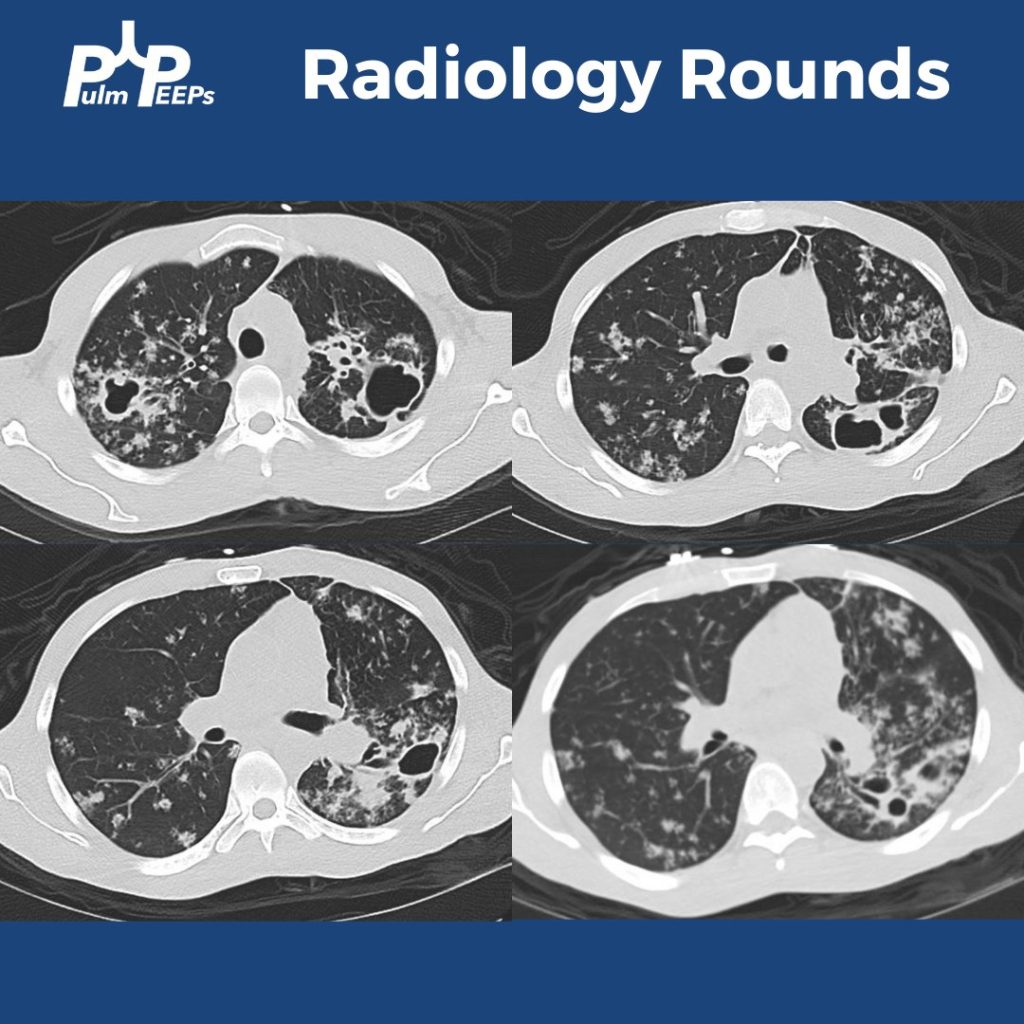
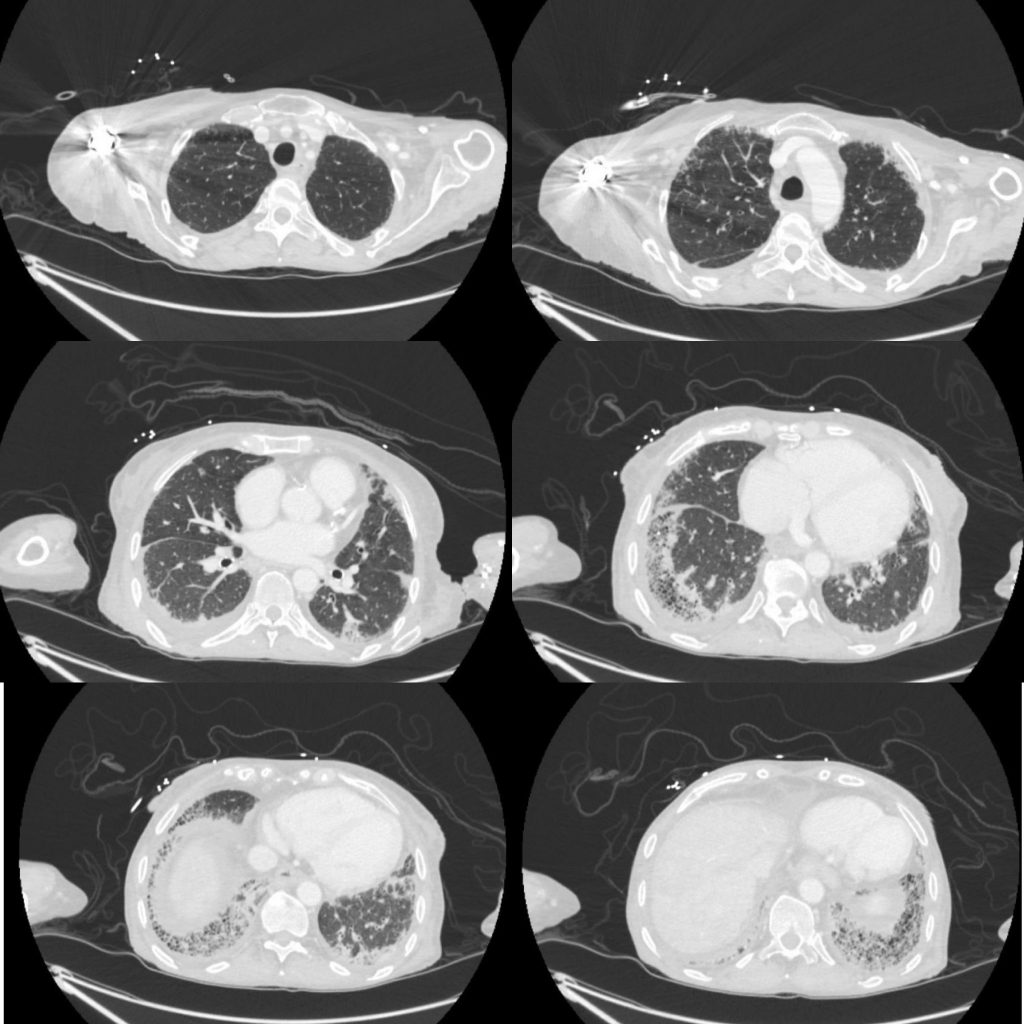
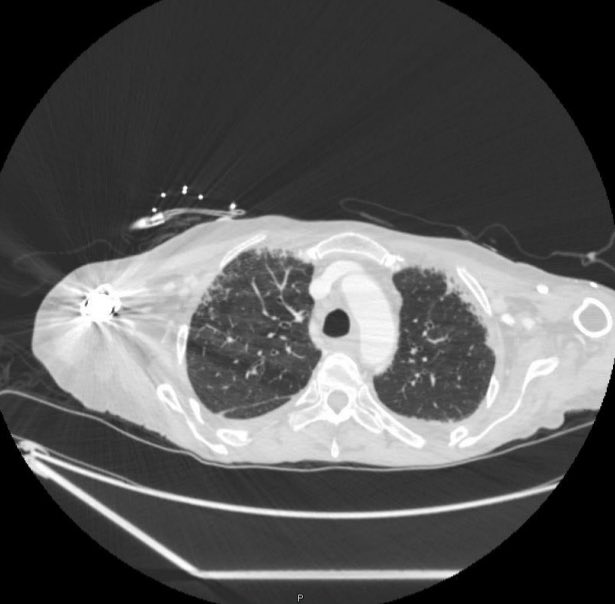
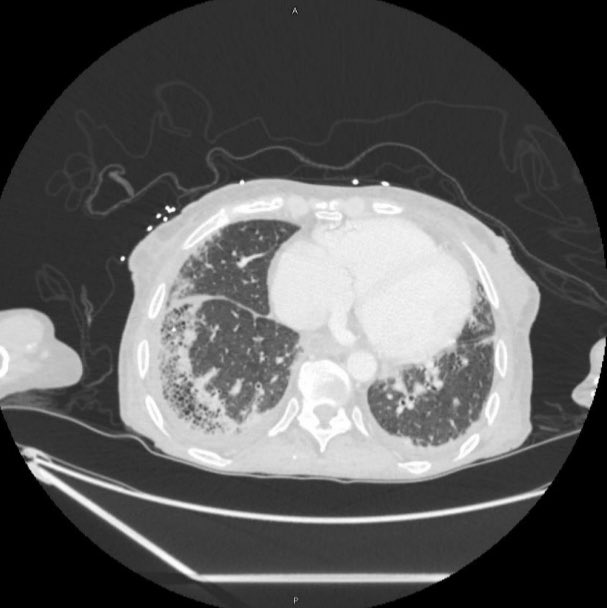
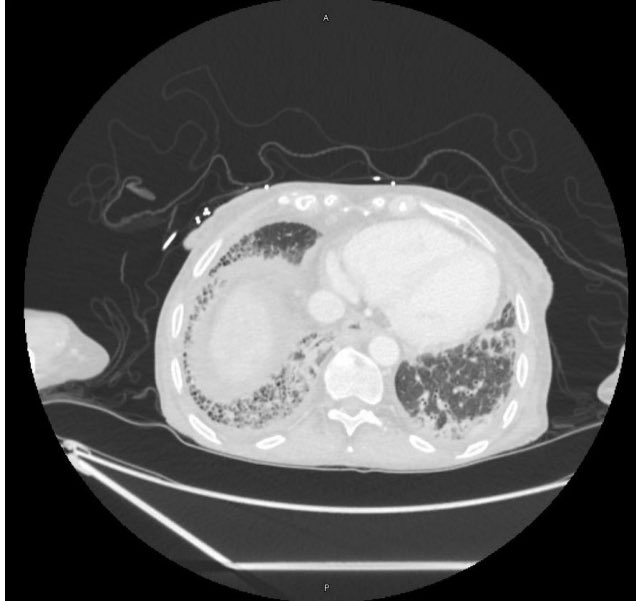
We are back with our first #RadiologyRounds of the new academic year. We have a young, immunocompetent man presenting with fever, weight loss, and abdominal pain.
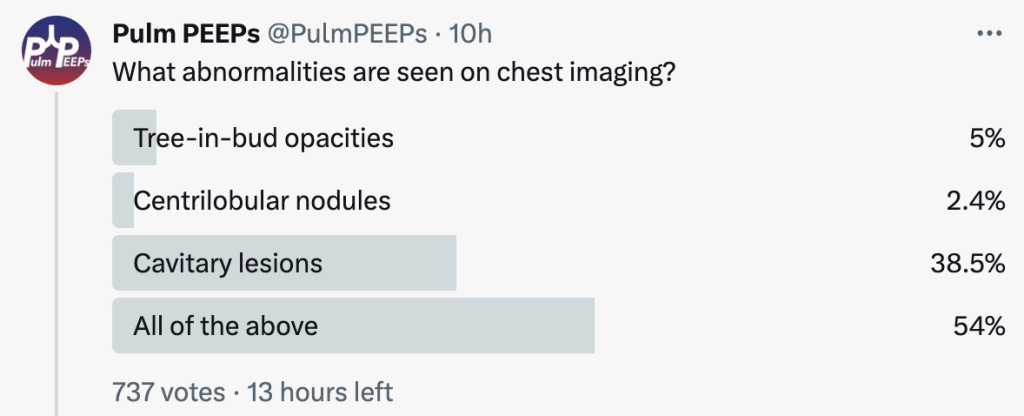
What abnormalities are seen on his chest imaging?
He was found to have bilateral apical cavitary disease, centrilobular nodules, and tree-in-bud opacities. He developed a productive cough with blood-tinged sputum as well as diarrhea.
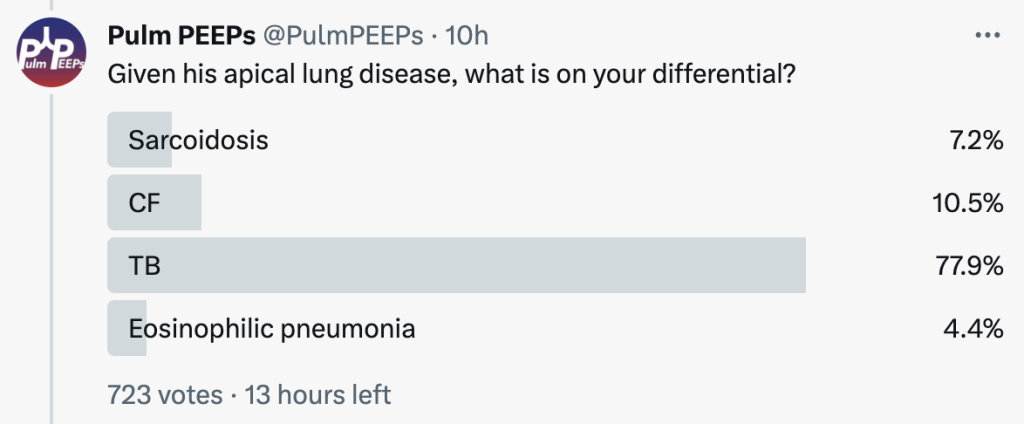
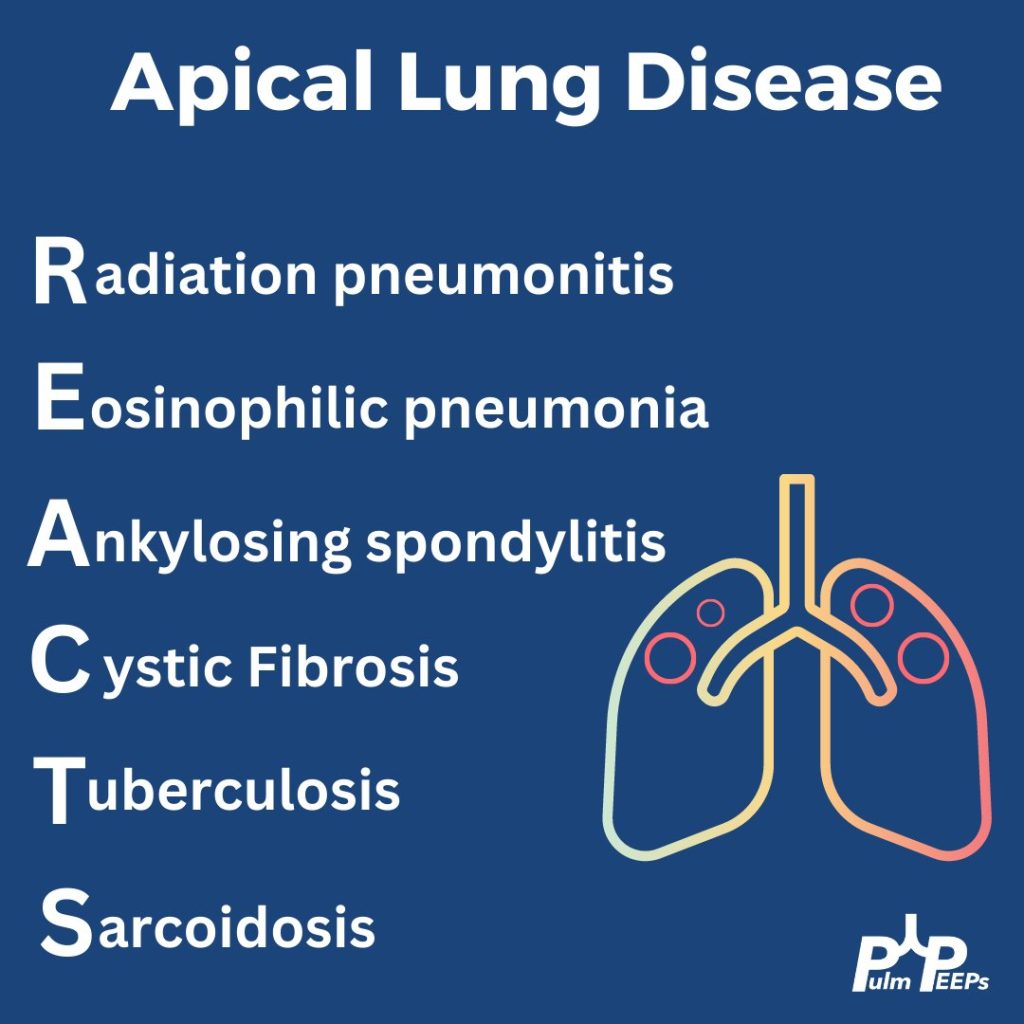
Given his apical lung disease, what is on your differential?
When thinking about apical lung disease, remember the mnemonic REACTS to help with your differential.
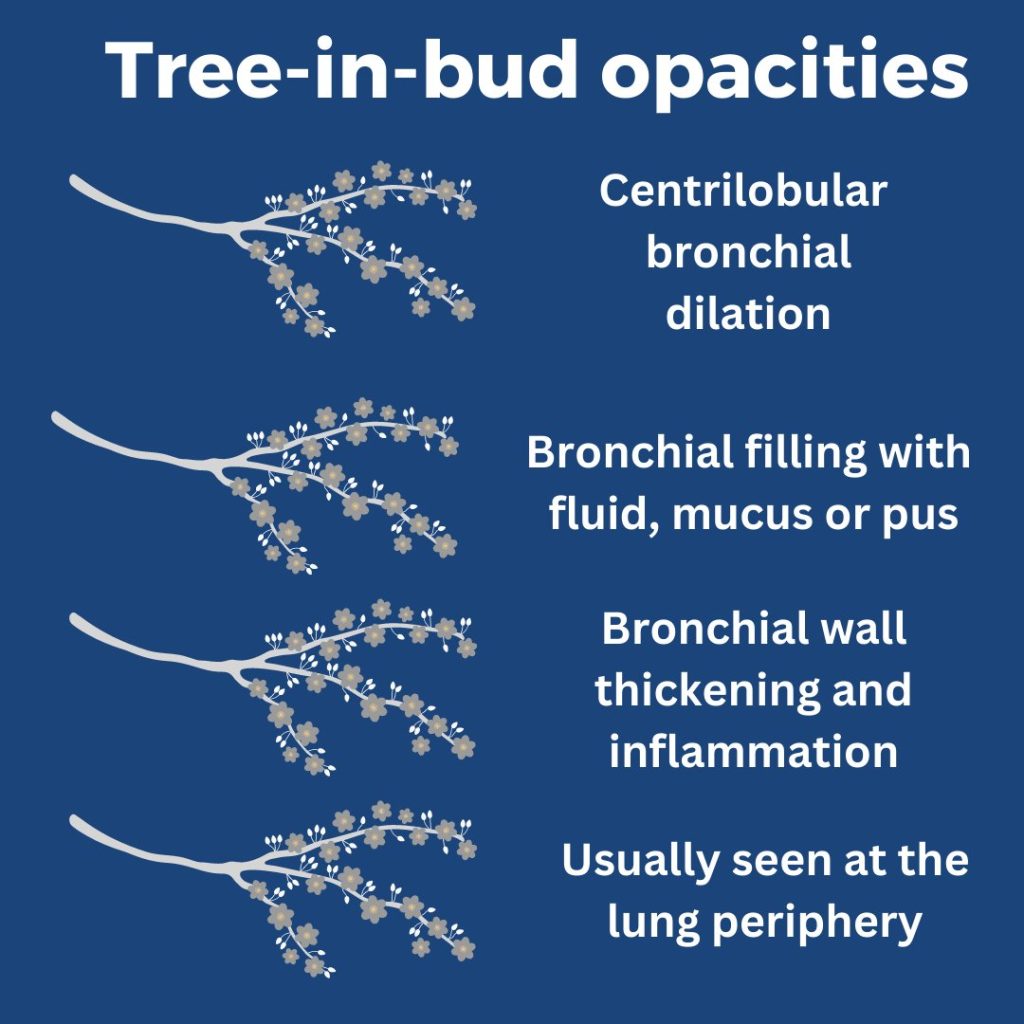
What are tree-in-bud opacities? They are findings seen on CT chest suggesting bronchial dilation, inflammation, and bronchial filling with fluid, mucus, or pus that can be caused by infections and non-infectious etiologies.
He had sputum and AFB cultures sent and his AFB smear was positive. He was ultimately diagnosed with disseminated TB and started on RIPE therapy.
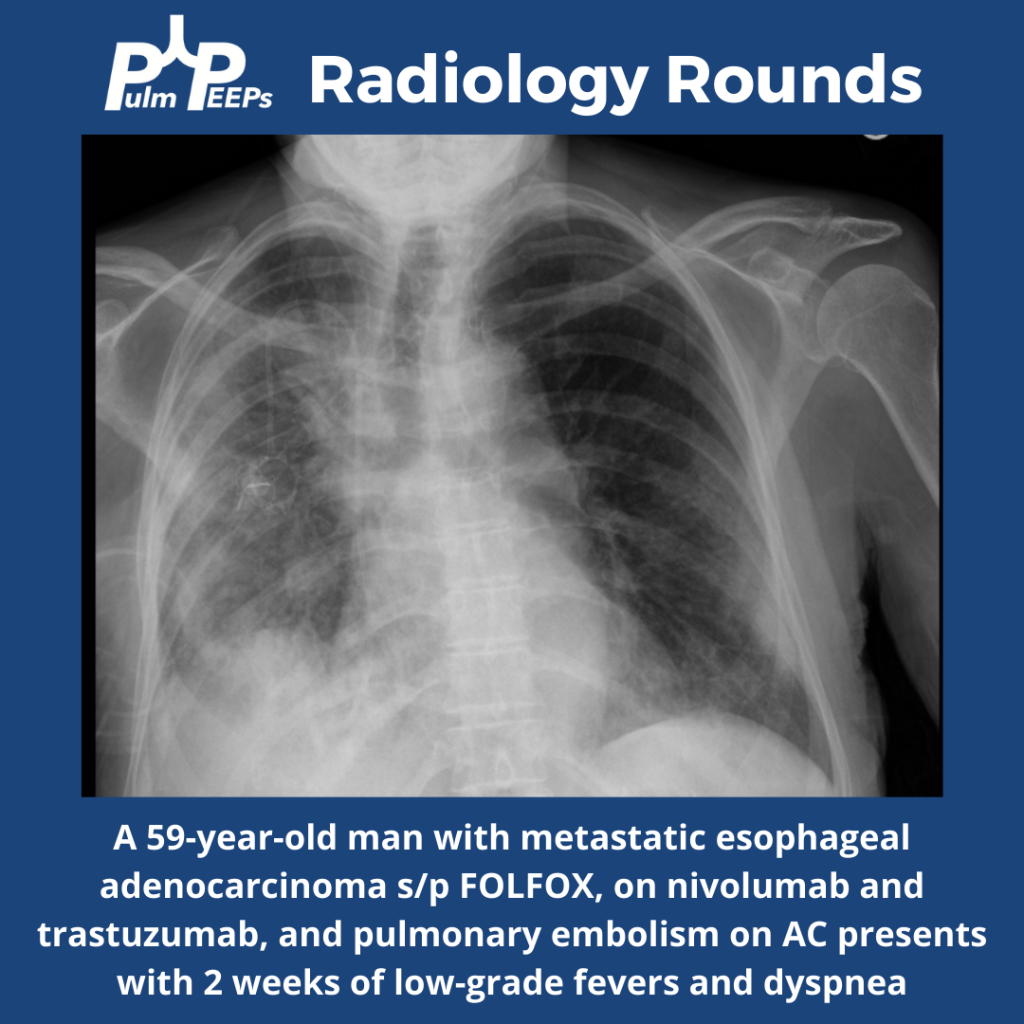
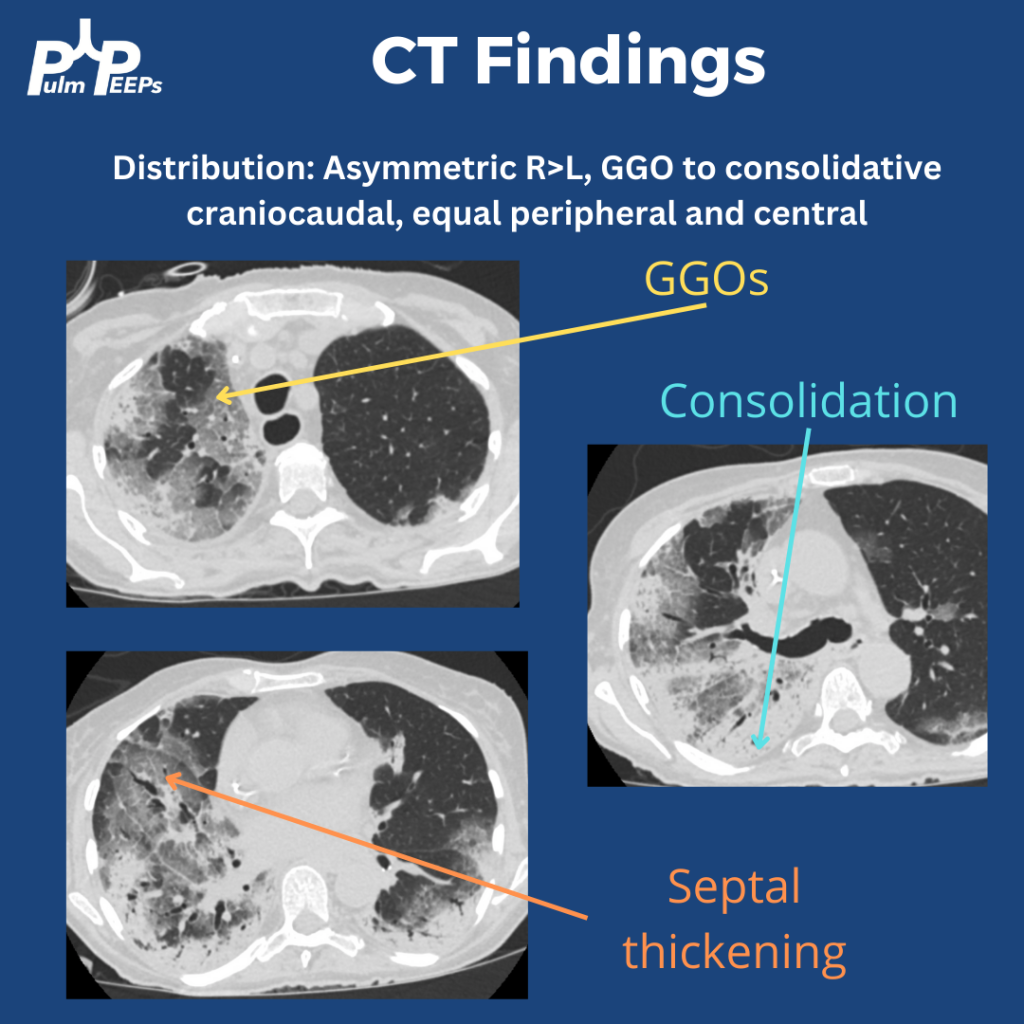
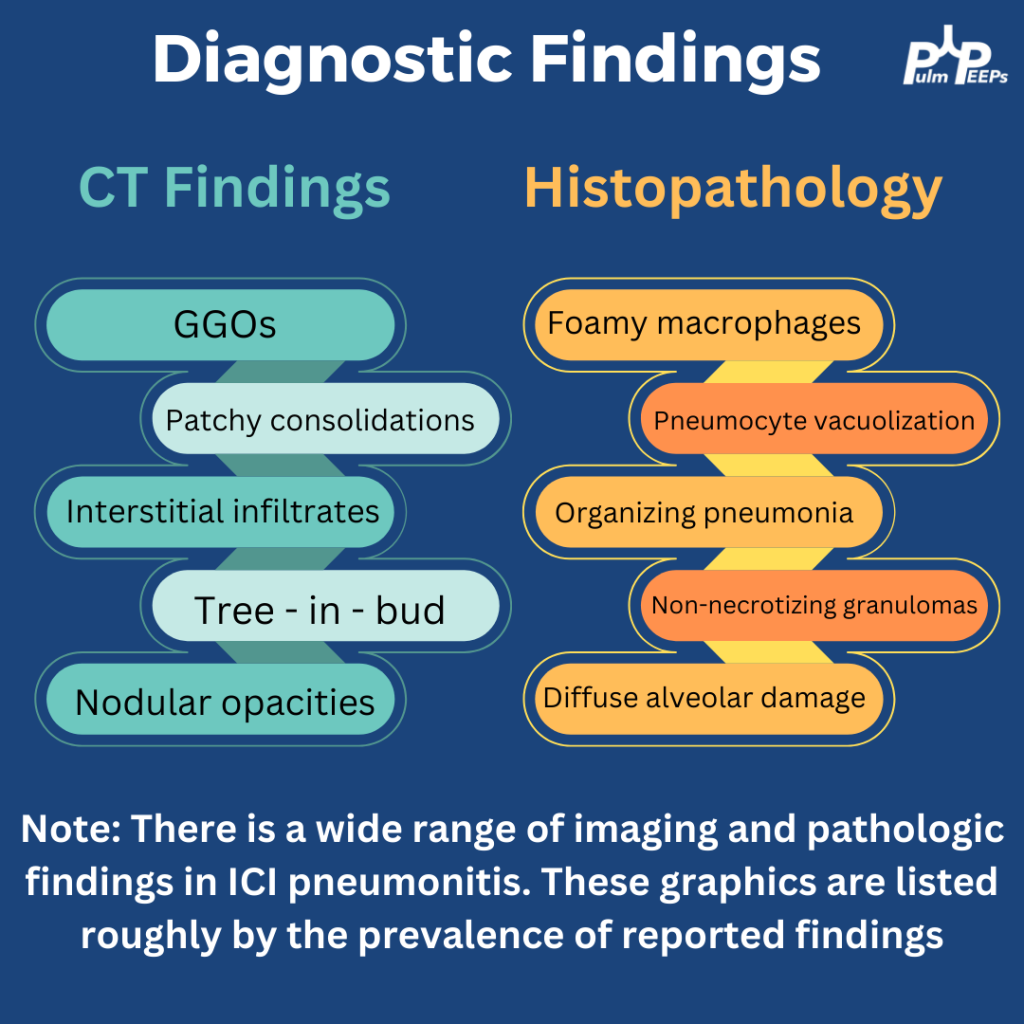
A middle-aged man with metastatic esophageal cancer presents with 2 weeks of low-grade fevers and more recently progressive dyspnea. His exam is notable for late inspiratory crackles throughout the right lung.
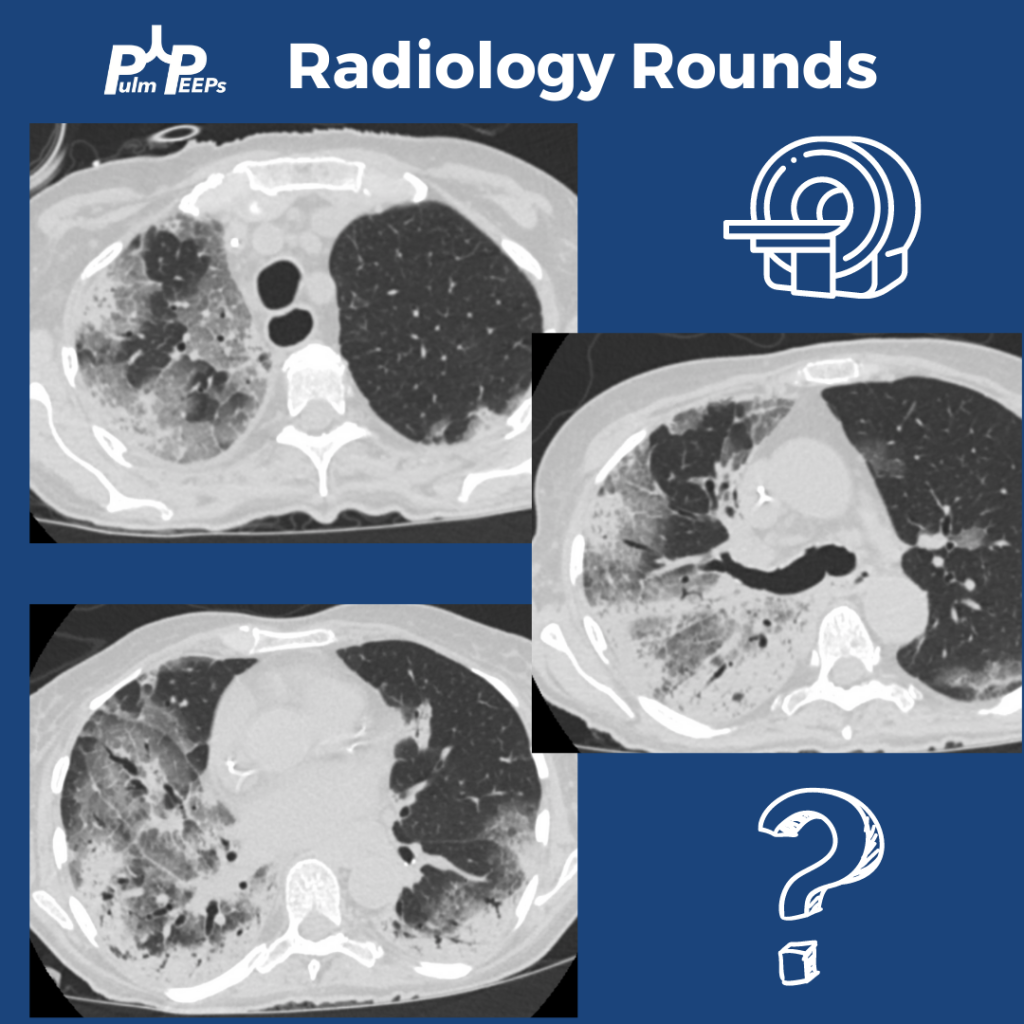
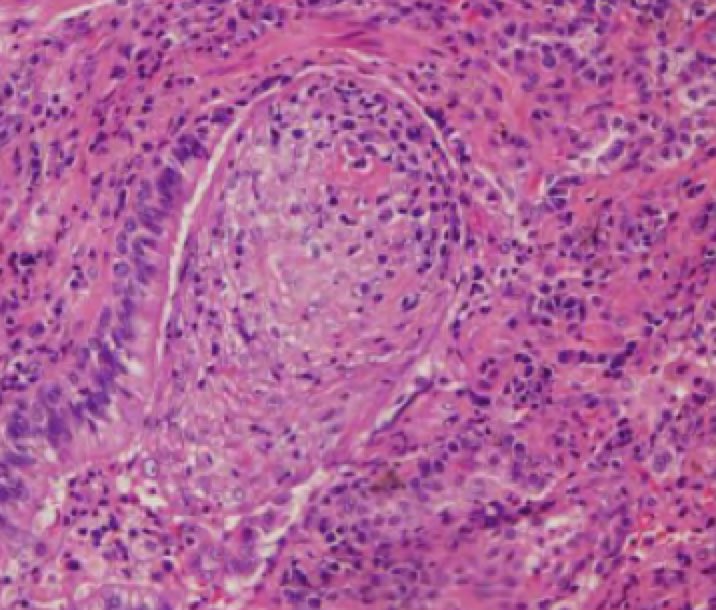
A bronchoscopy was performed and an expanded infectious panel was sent and all were negative, as were serum infectious studies (e.g. histoplasmosis ag, urine legionella etc). A trans bronchial biopsy showed plugs of granulation tissue filling the alveolar spaces
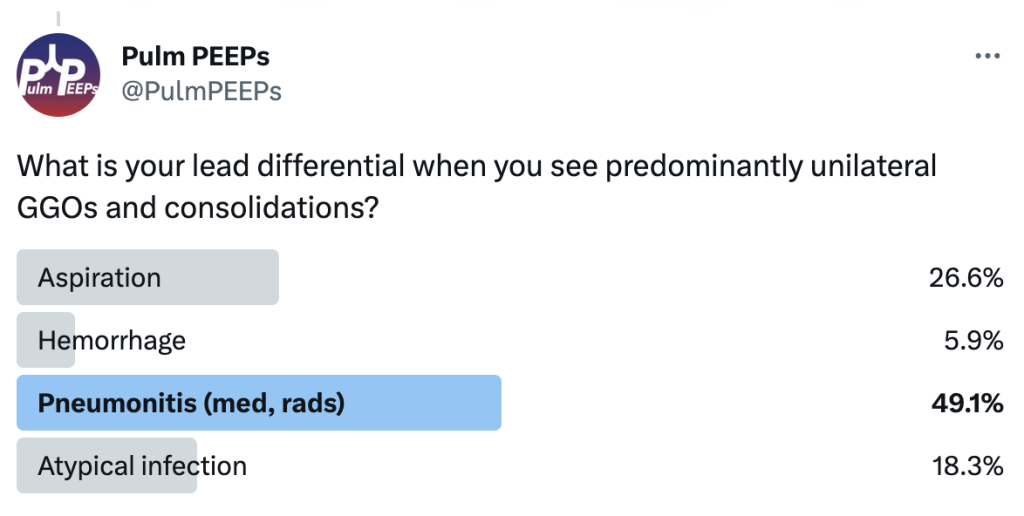
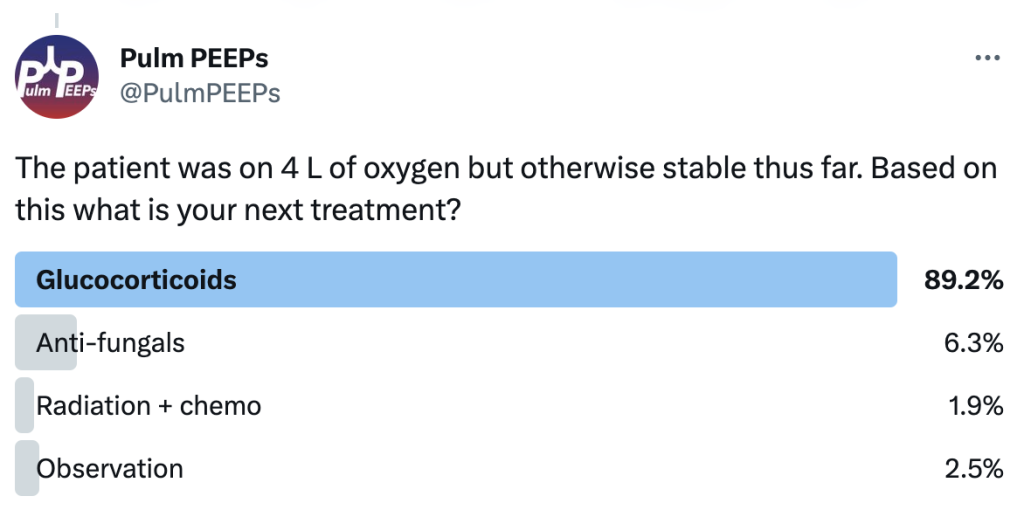
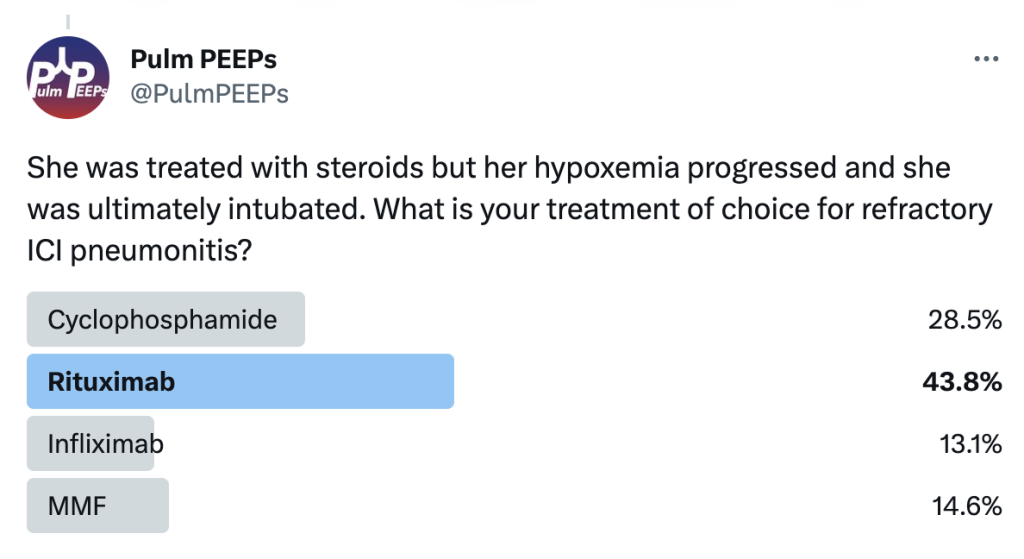
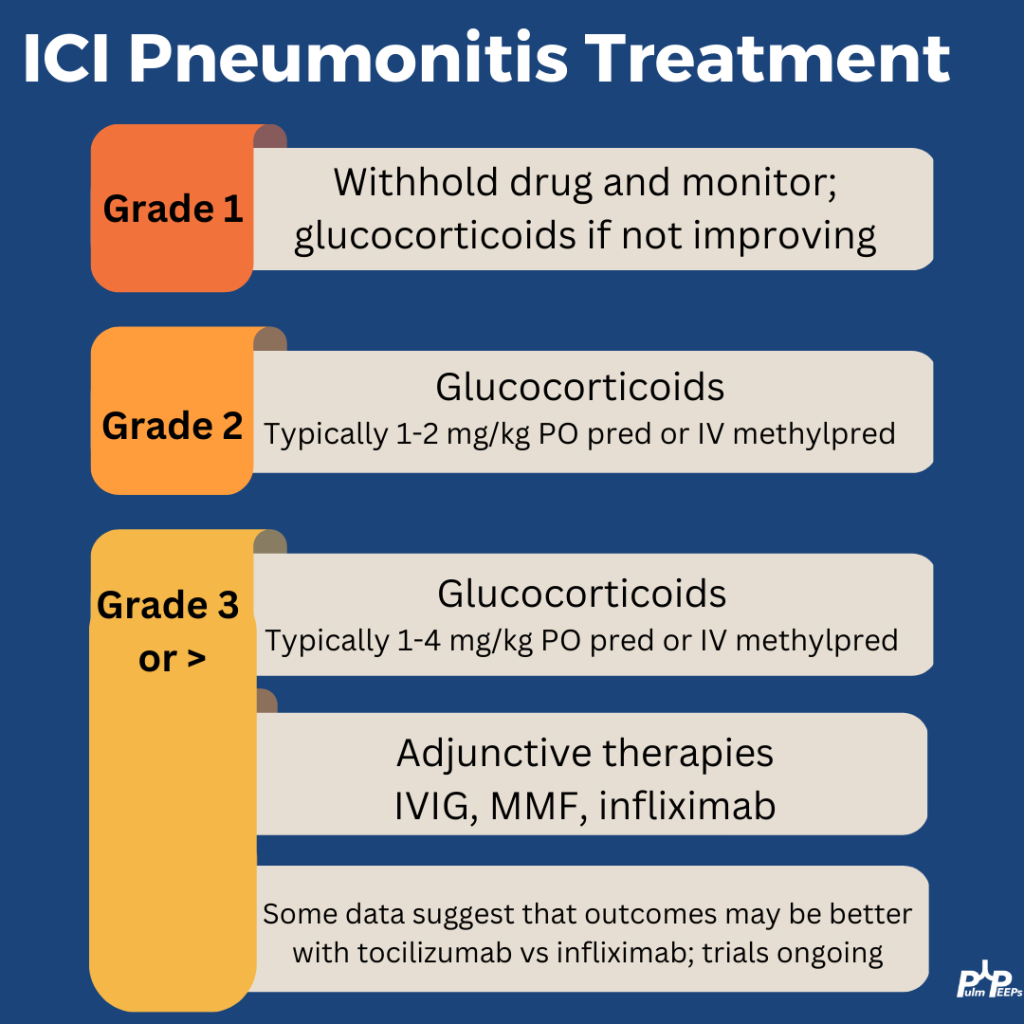
He was treated with steroids but her hypoxemia progressed and she was ultimately intubated. What is your treatment of choice for refractory ICI pneumonitis?
Severe ICI is rare and the treatment for steroid refractory disease is still based on small series and case reports This patient was treated with high-dose steroids (2mg/kg), IVIG, MMF, and tocilizumab. With that, he improved after 10 days intubated and was weaned to room air.
Today’s #RadiologyRounds is a reminder that pulmonary care extends beyond the lungs! Although we’ll have a CT chest too
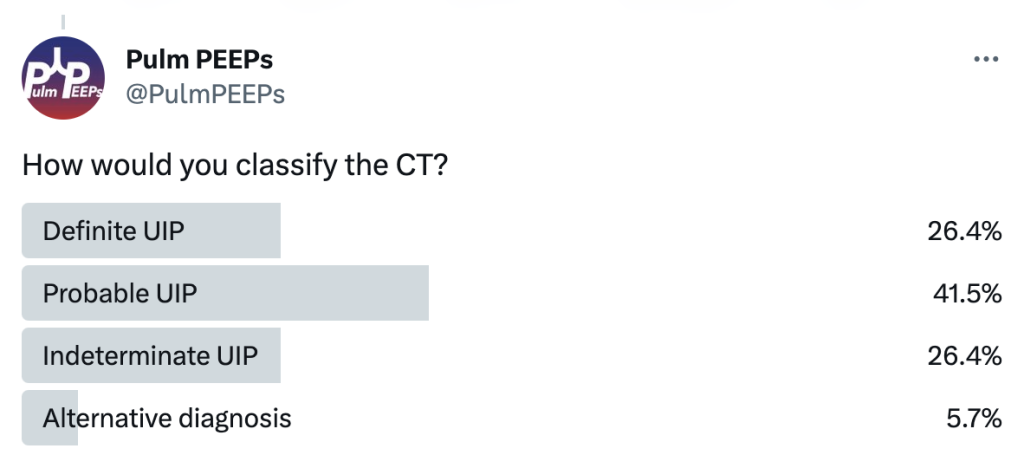
A 70-year-old woman with a diagnosis of seronegative RA presents with progressive dyspnea. PFTs show a moderate restrictive defect and moderately reduced DLCO. Here is the CT scan:
The CT was interpreted as indeterminate for UIP / fibrosing NSIP. The basilar and subpleural fibrosis and honeycombing are consistent with UIP, but with reticular nodular infiltrates and pleural effusions that are less consistent. In reviewing her history: RF, CCP, and anti-SCL70 were all negative. On hand exam, she had MCP enlargement, some PIP synovitis, and slight R hand ulnar deviation. She did not have clear telangiectasias. She had a history of GERD. She denied Raynauds. She had significant skin thickening over her legs and limited ankle mobility. X-rays were obtained:
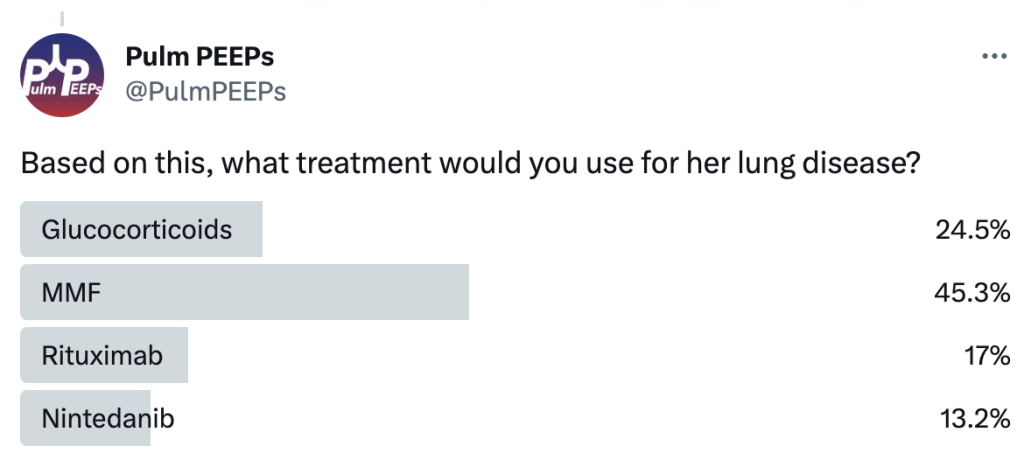
This showed severe dystrophic calcifications and no bony erosions. This degree of extensive dystrophic calcifications is consistent with scleroderma and the patient was felt to have limited scleroderma, and possibly an overlap syndrome
The patient was started on MMF as the initial agent based on the Scleroderma Lung Study II (SLSII): https://pubmed.ncbi.nlm.nih.gov/27469583/ Glucocorticoids were avoided given the risk of scleroderma renal crisis with steroids. An anti-fibrotic was also considered but not started as 1st line.
For “#RadiologyRounds” today, we won’t be looking at any imaging, but we’ll be looking at some vent wave forms and examining dysynchrony! This is a re-booted @david_furfaro Tweetorial. I hope you enjoy and this is an open invitation for all dysynchrony waveforms!
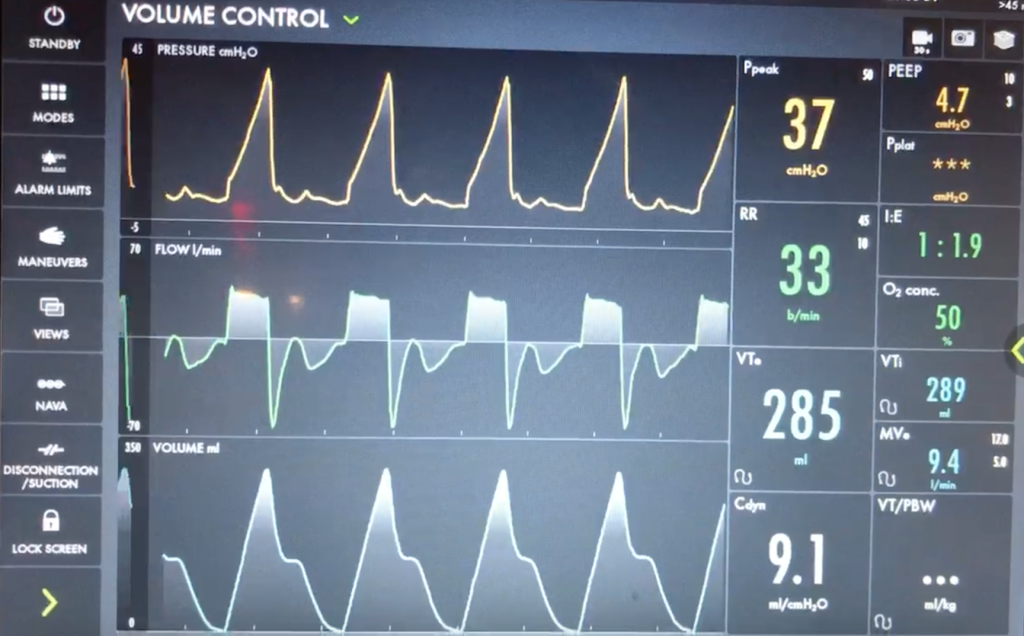
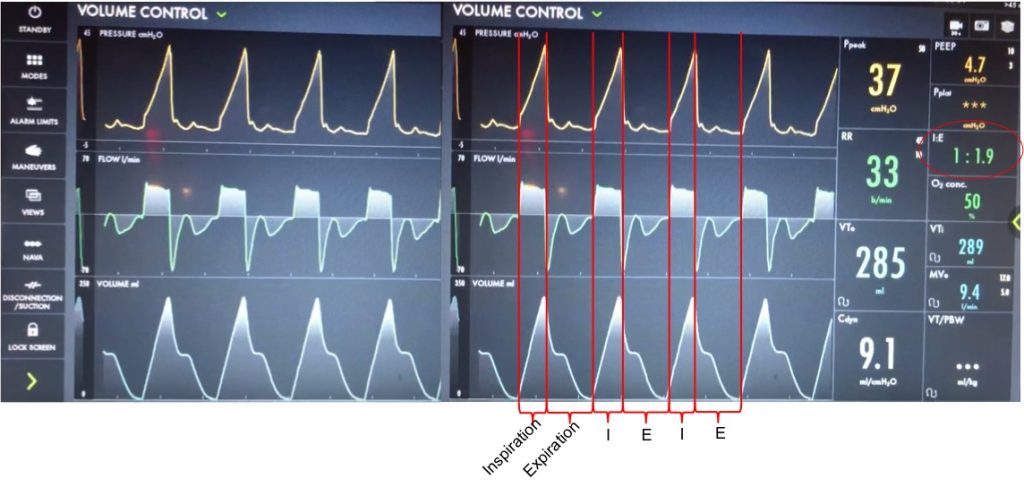
A 40s M is intubated for ARDS. In order to maintain lung protective ventilation, he was on high does of propofol, fentanyl and midazolam. His sedation is being weaned slightly now, and the RN calls for vent dysynchrony. His ventilator looks like this
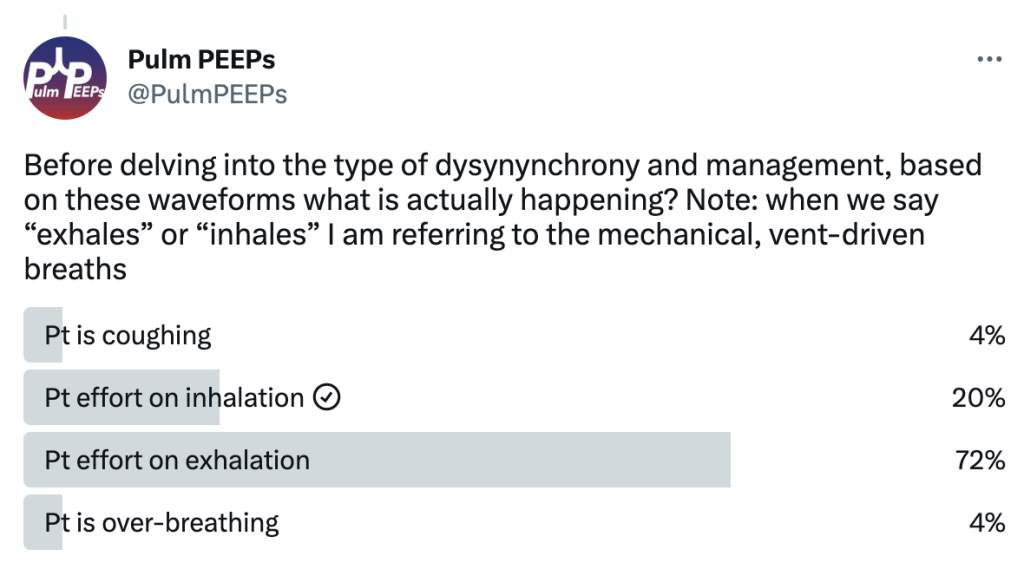
Before delving into the type of dysynynchrony and management, based on these waveforms what is actually happening? Note: when we say “exhales” or “inhales” I am referring to the mechanical, vent-driven breaths
Let’s take a look at the waveforms and identify the phase of breathing. This is VC with a square flow waveform, so as a set volume is delivered, the flow is at a constant rate, and the pressure is measured. Expiration is about 2x as long as inspiration (determined by I time or flow rate)
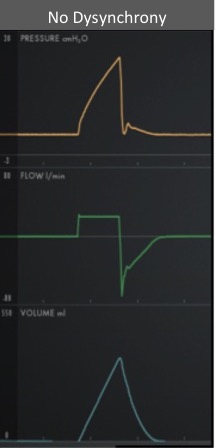
With a passive patient (no dysynchrony) after inspiration, the volume curve should show a smooth decrease with exhalation, the pressure curve should flatten to the set PEEP, and the flow will be negative and gradually return to 0 as the patient exhales
In our case, you can see simultaneous dysynchrony in all three waveforms during exhalation (red arrows) vs normal (orange lines). There is a pressure negative deflection; the flow quickly rises to 0 before returning to negative; and the volume curve plateaus as exhalation pauses
Putting this together, it means that during expiration there is an inspiratory effort. The patient is trying to inhale, which causes a negative pressure deflection, and a pause in air flowing out of the lungs. If this effort triggered a breath, there could be breath stacking. Notice that the same pattern occurs after every breath, and clinically we said the patient was still heavily sedated. This combination of findings is a type of dysynchrony called REVERSE TRIGGERING or ENTRAINMENT.
You could consider whether this dysynchrony was an ineffective effort, but the trigger sensitivity was low, and the pattern and consistent timing after inspiration is more consistent with reverse triggering.
The change in pressure and flow of a ventilator-initiated, mandatory breath stimulates an inspiratory effort from the patient. Theories differ on if this is mediated by the diaphragm or central respiratory center. This can start during the ventilator-delivered breath, or afterwards in exhalation, as with our patient.
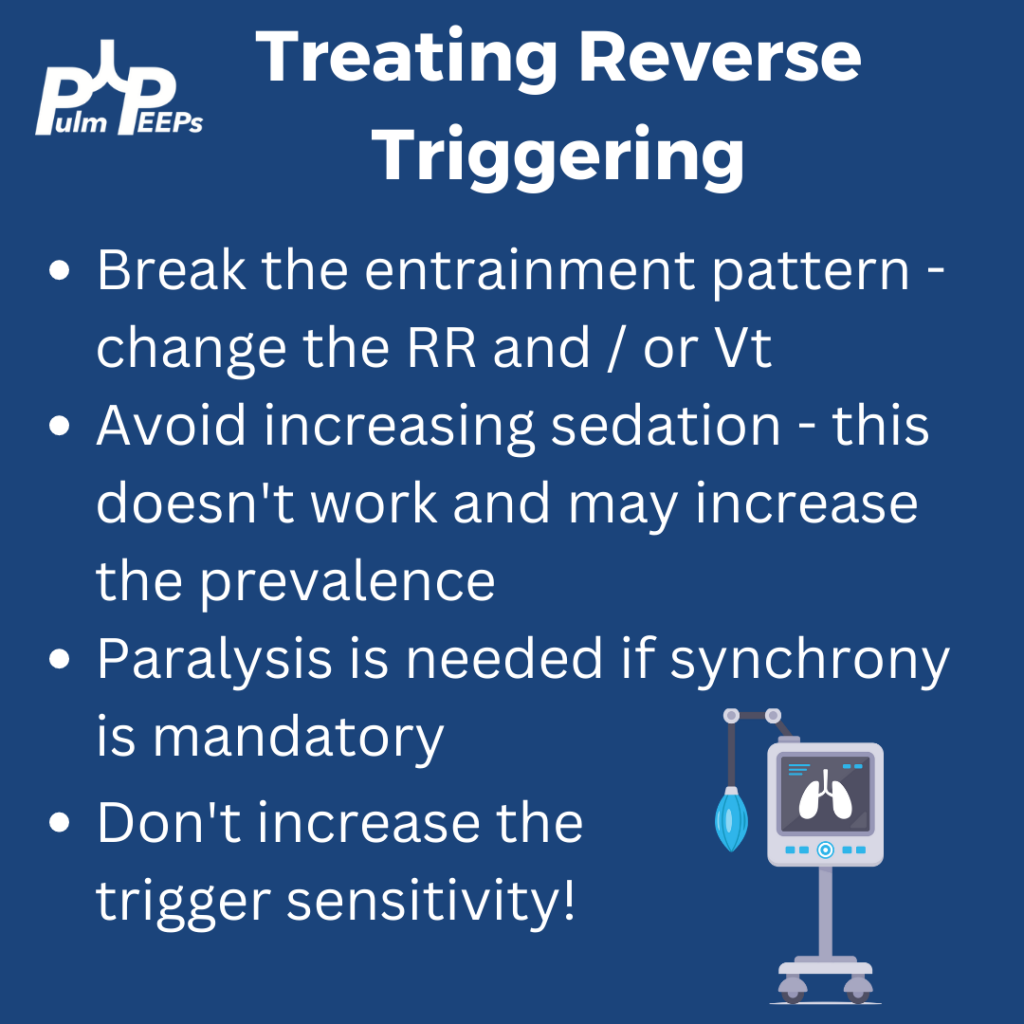
Reverse triggering often occurs in heavily sedated patients, and is defined by a stable, repetitive pattern (i.e. it is not voluntary, but reflex mediated). It can also occur in anoxic brain injury. Treating it involves breaking the pattern and avoiding harmful therapies. It can even be induced in healthy patients but this is much less clinically relevant, and is rare.
DO NOT just increase the trigger sensitivity of the vent. This can stop breath stacking but does not prevent dysynchrony and it can cause harmful changes in transpulmonary pressure. For this patient, sedation was lightened slightly, and the respiratory rate decreased and the pattern of reverse triggering ultimately broke without the need for paralysis.
It is Tuesday #RadiologyRounds time! We are in a pleural state of mind here at Pulm PEEPs. This is another great case authored by rockstar-associate editor @TessLitchman
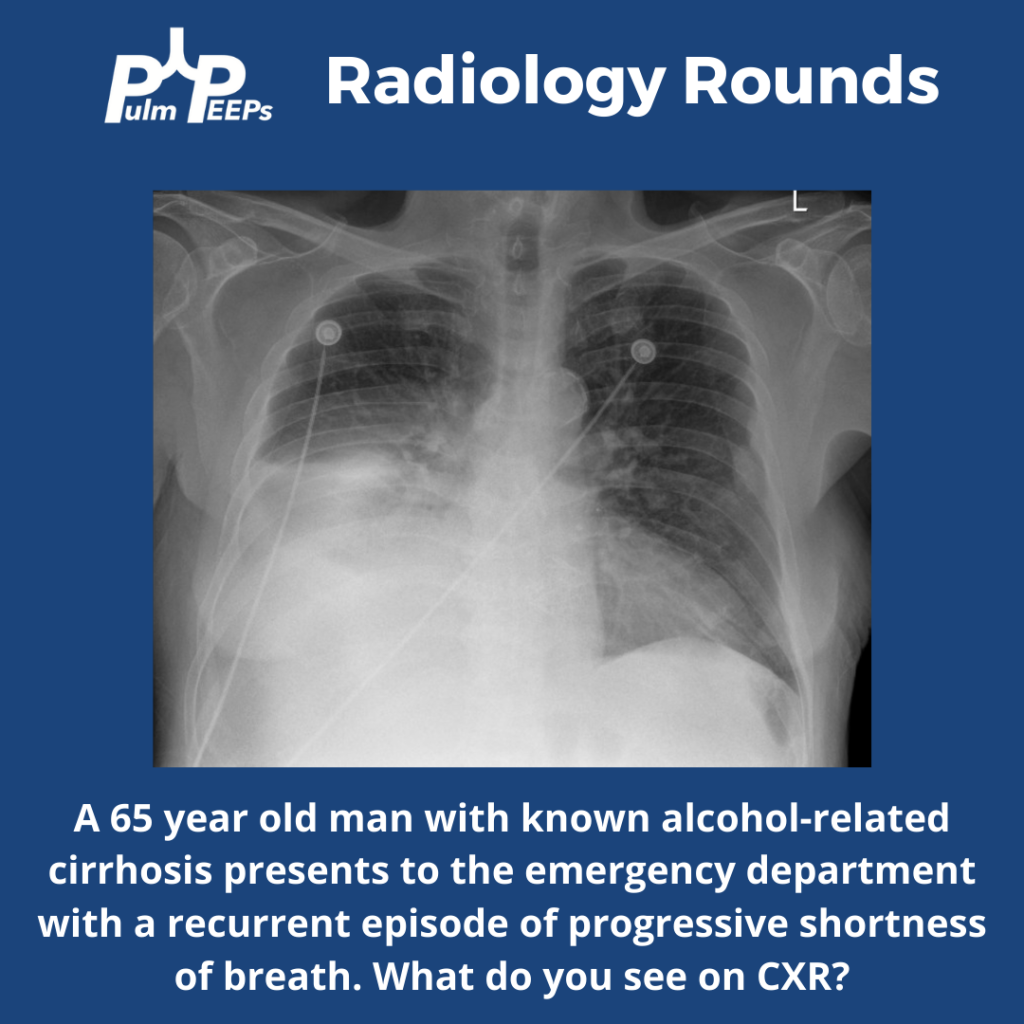
A 65-year-old man with cirrhosis presents to the ED with progressive shortness of breath:
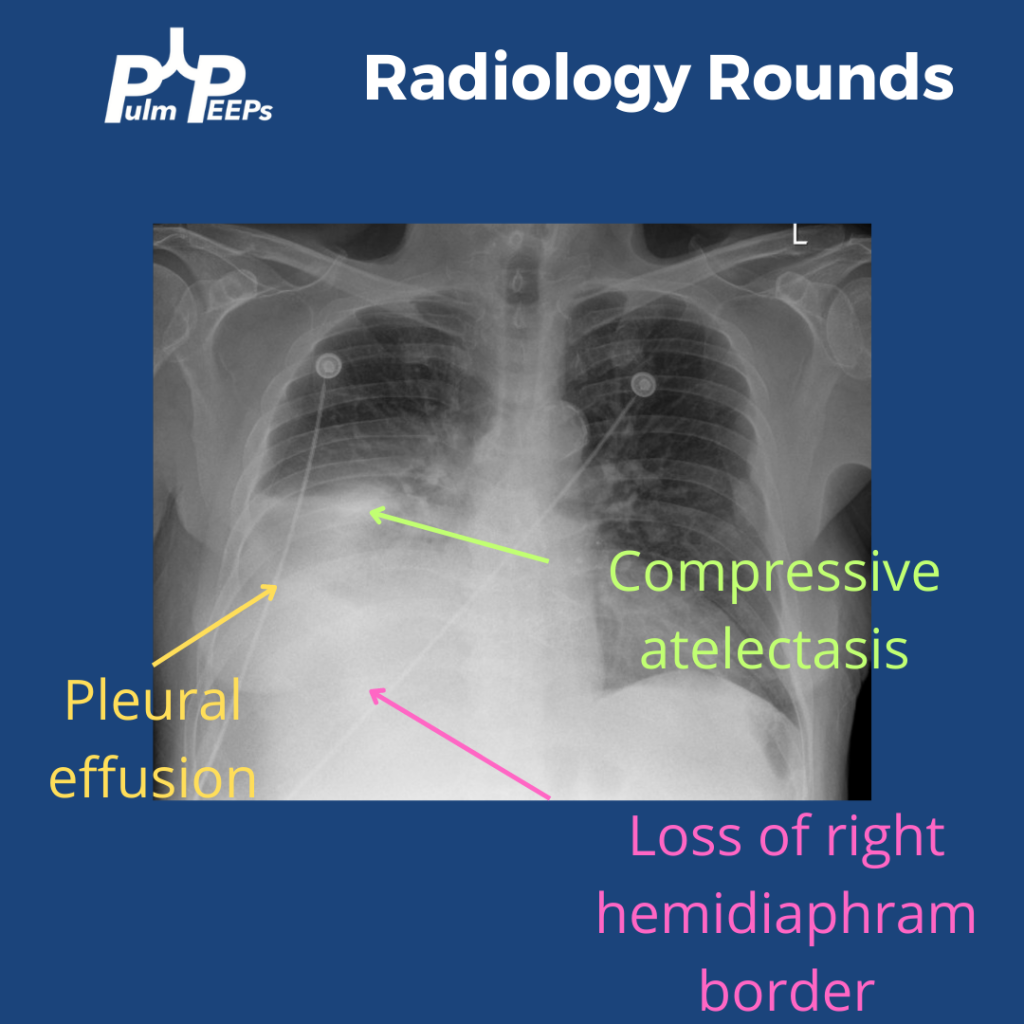
The CXR has a right lower opacity decreasing in density that is silhouetting the right hemi-diaphragm without signs of volume loss on the right concerning for pleural effusion. There is also associated atelectasis adjacent to the effusion
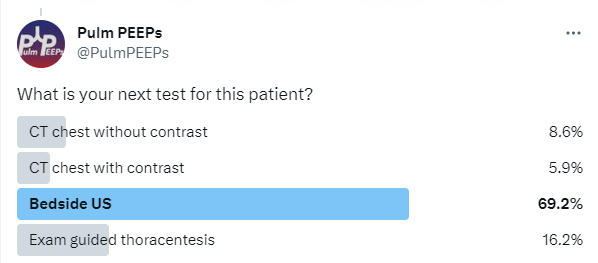
What is your next step for this patient?
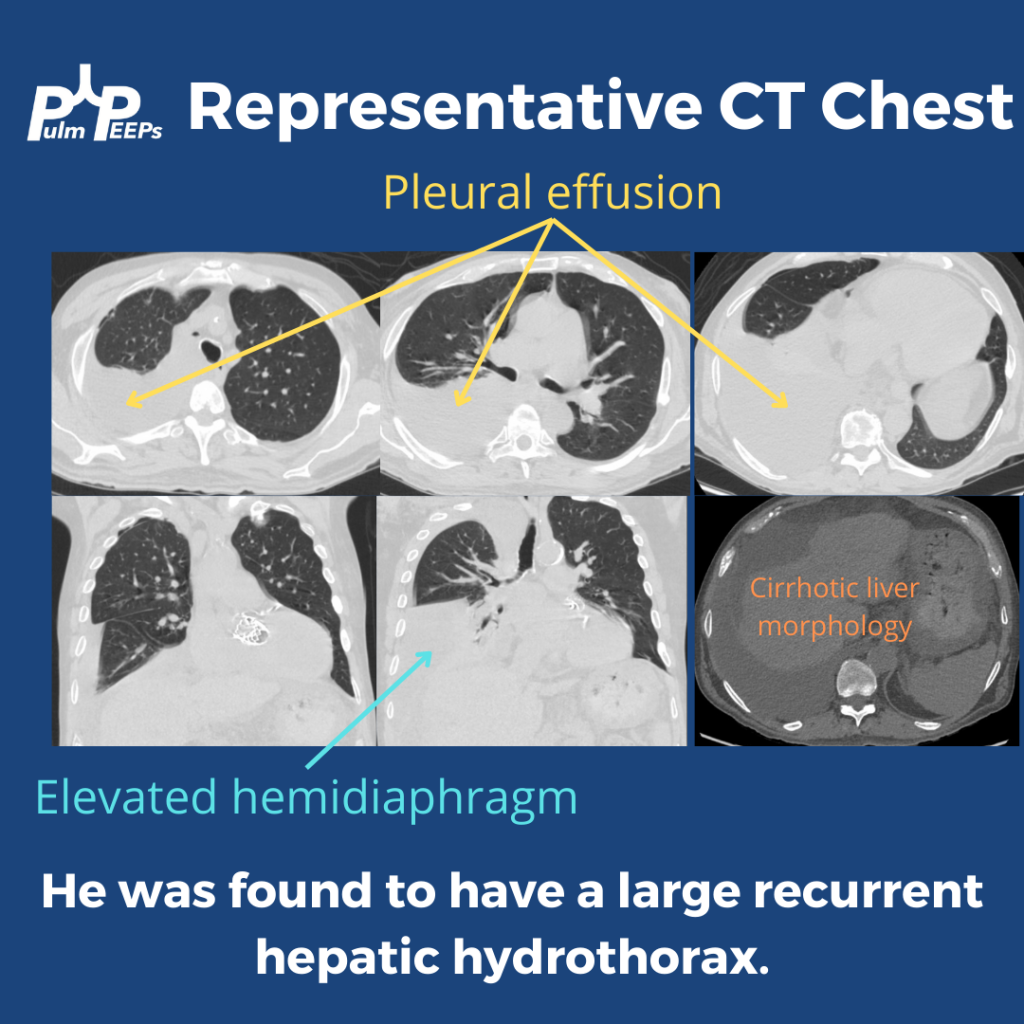
This patient had a bedside POCUS revealing a simple pleural effusion and abdominal ascites. He also had a CT scan performed:
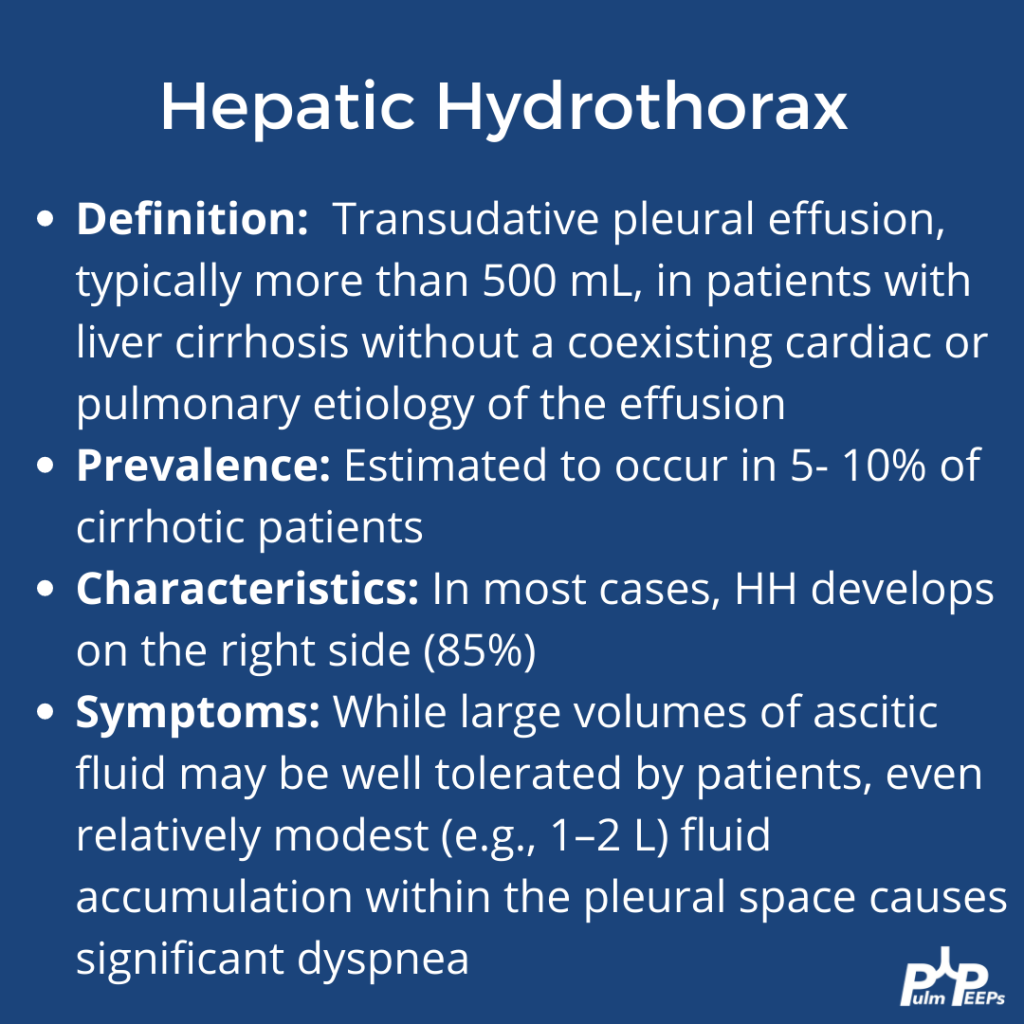
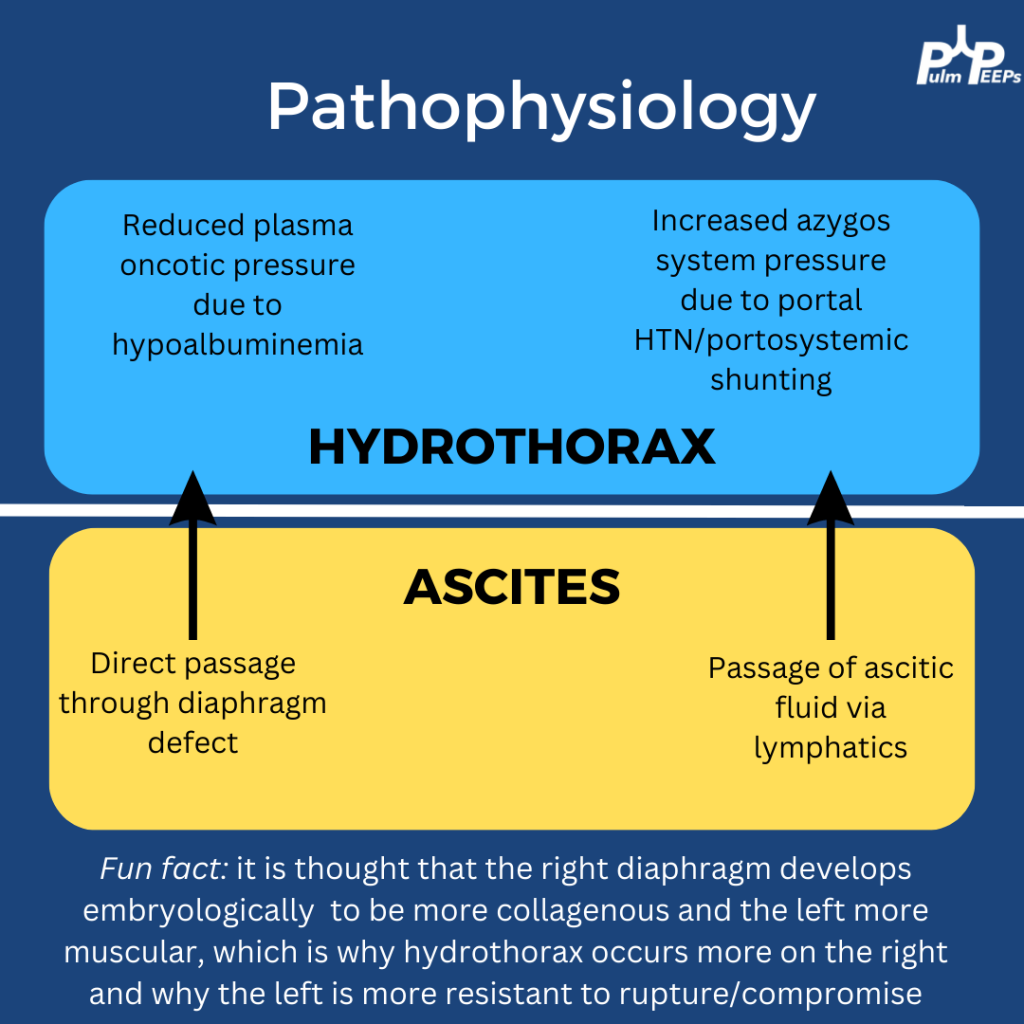
Based on his imaging and history, the most likely diagnosis on the differential was a hepatic hydrothorax. Here is some more information on hepatic hydrothoraces:
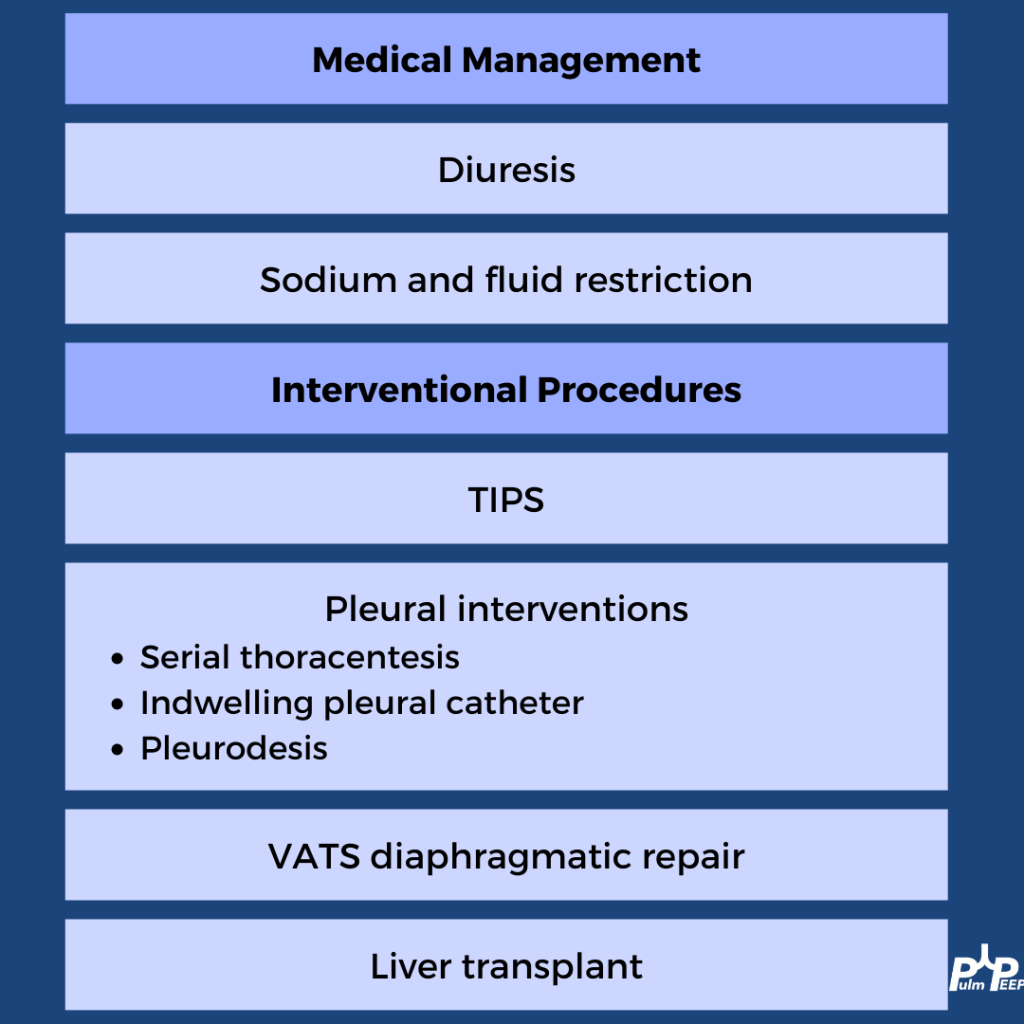
A transudative effusion was confirmed on thoracentesis, and no other clear etiologies were identified The treatment of hepatic hydrothorax should always start with medical management of volume overload in cirrhosis. Pleural procedures can be used for disease that is refractory
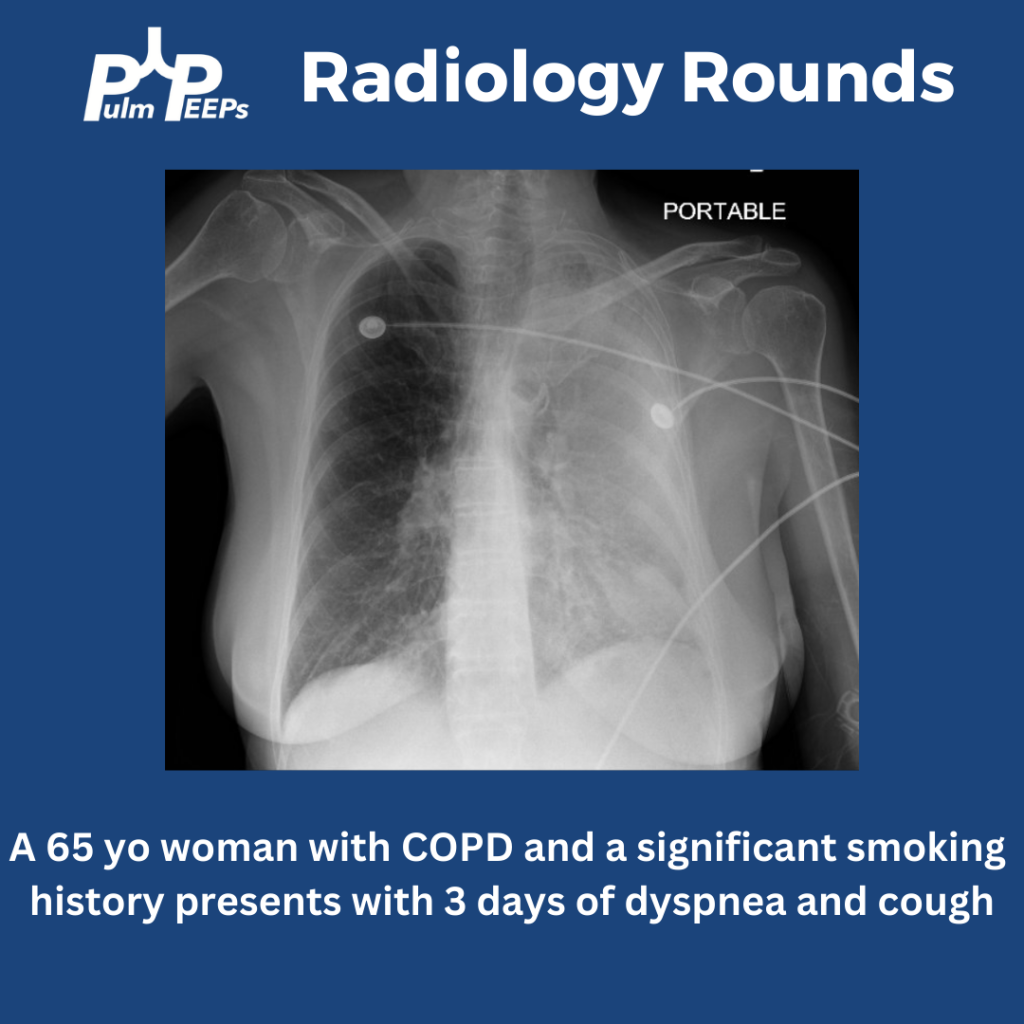
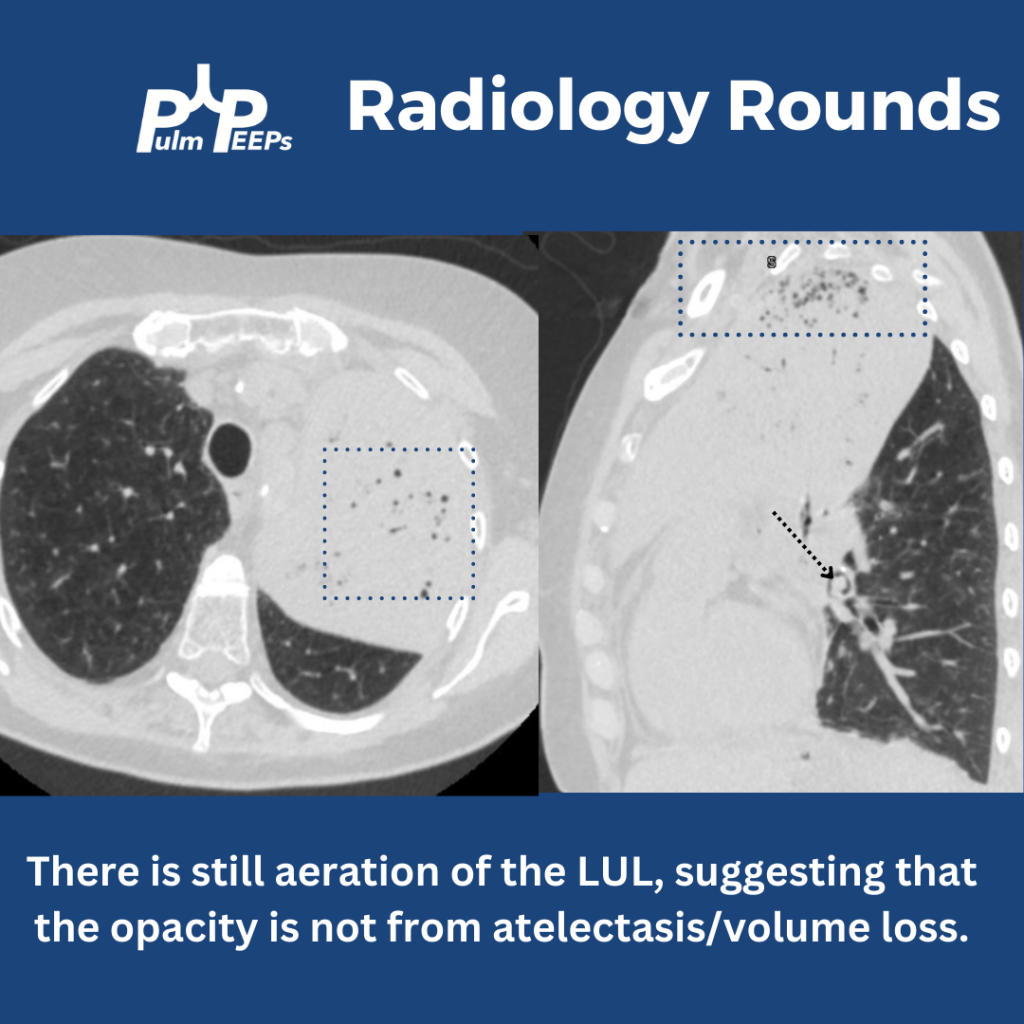
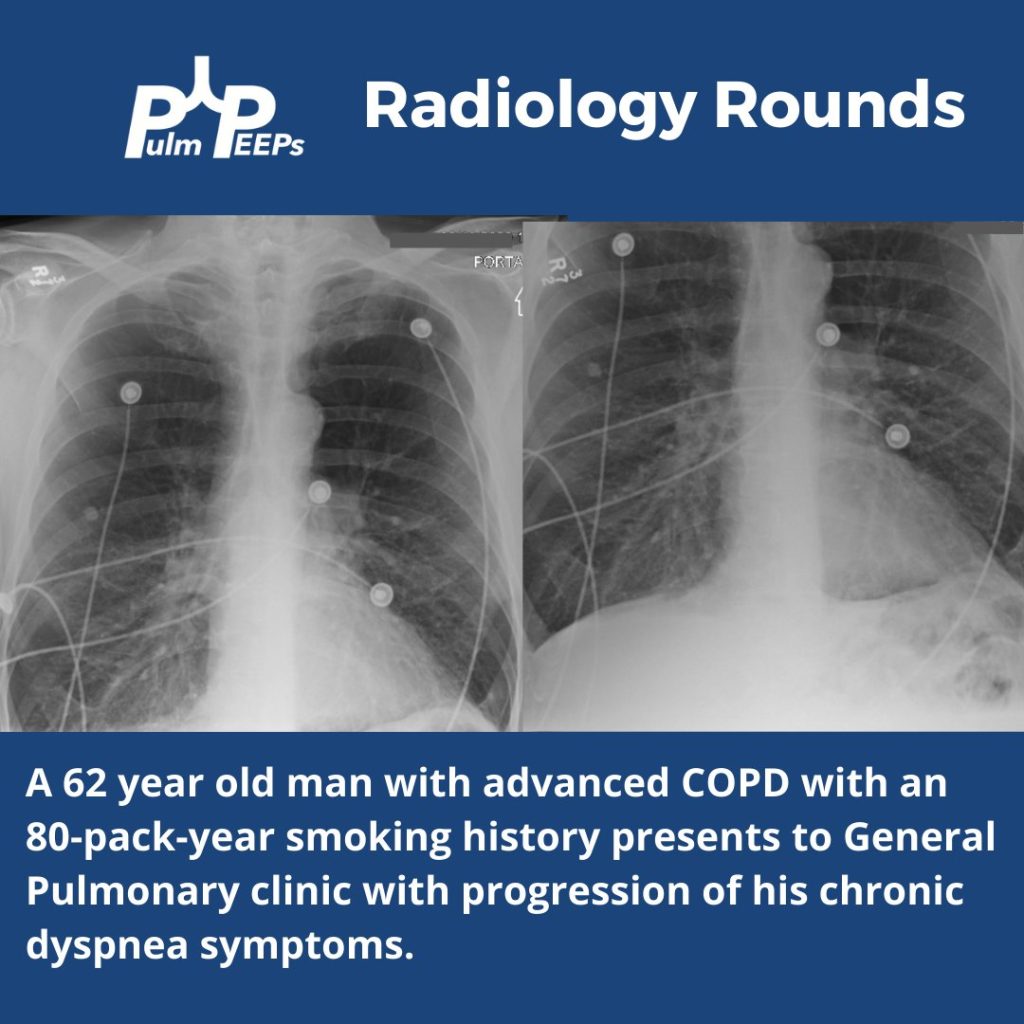
A portable film is obtained on a 65 yo woman with COPD presenting with progressive dyspnea and cough.
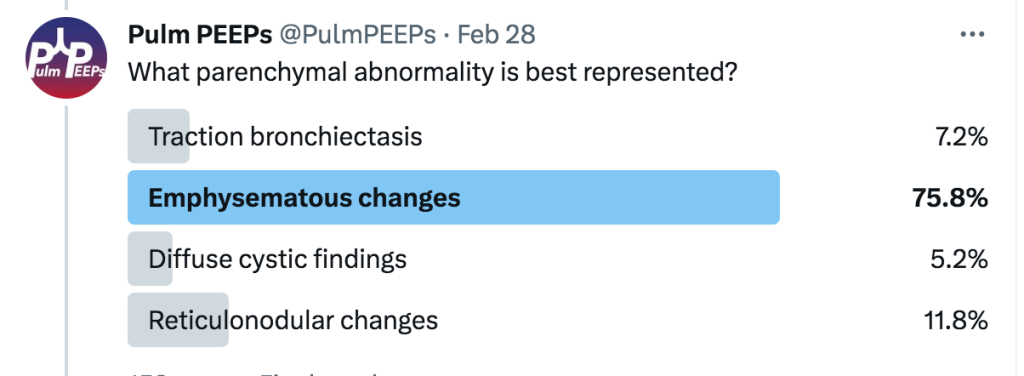
The image shows near complete opacification of the left lung. There is no ipsilateral or contralateral tracheal deviation which you would expect with atelectasis or a large pleural effusion, respectively. A CT chest is obtained to better visualize the parenchyma.
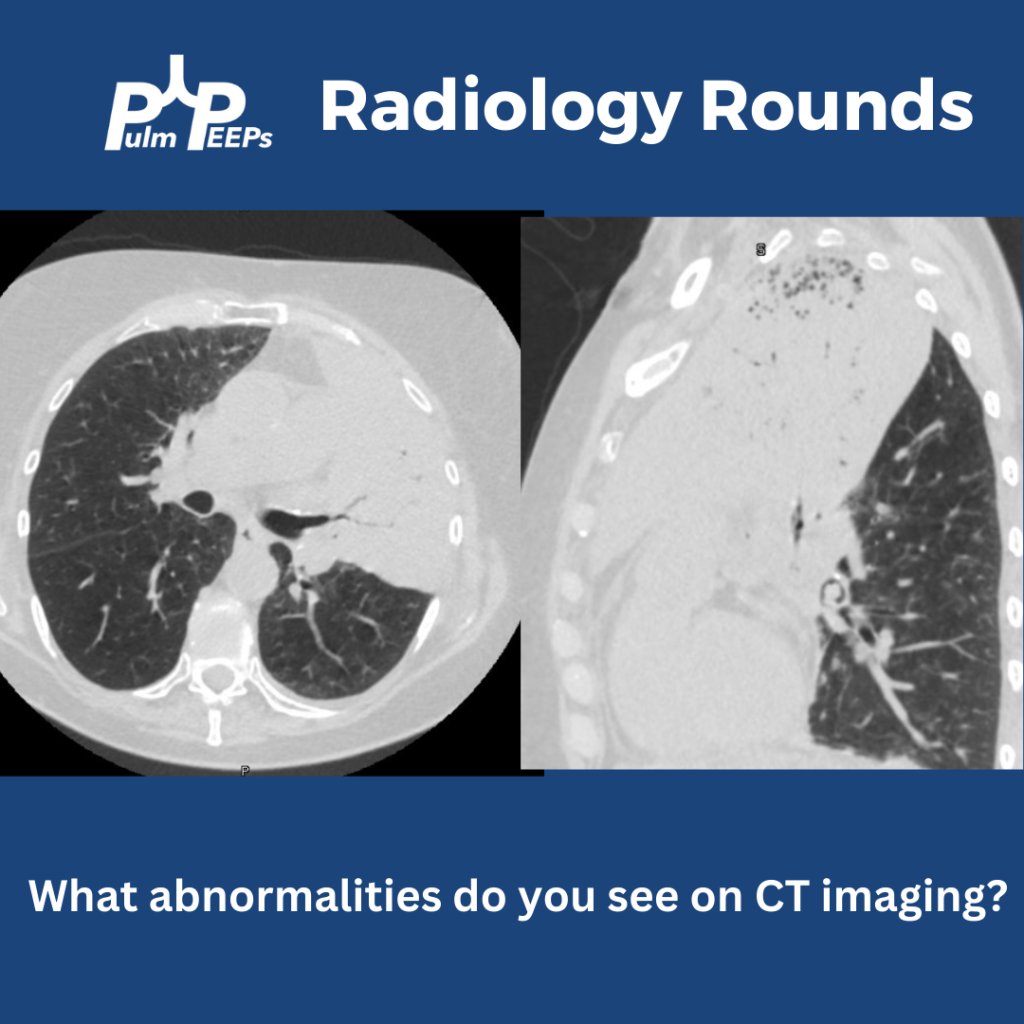
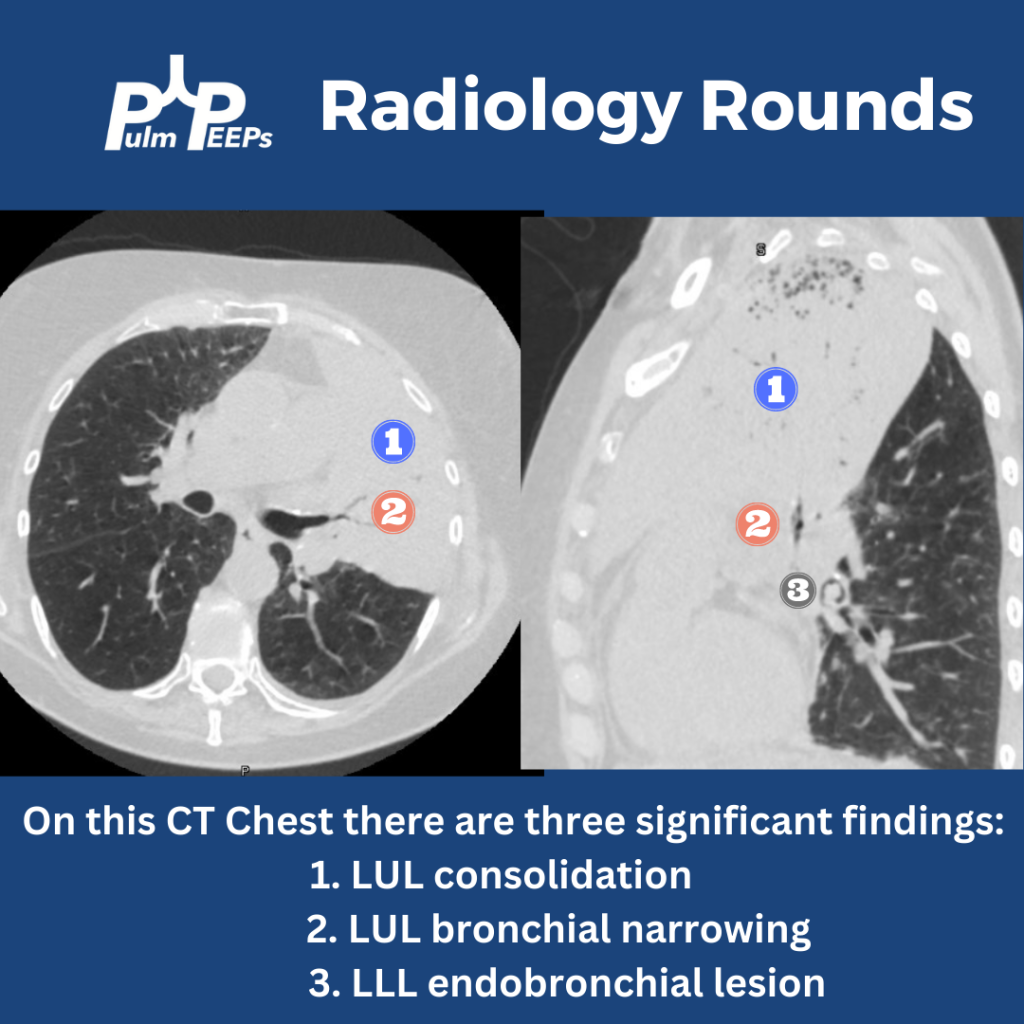
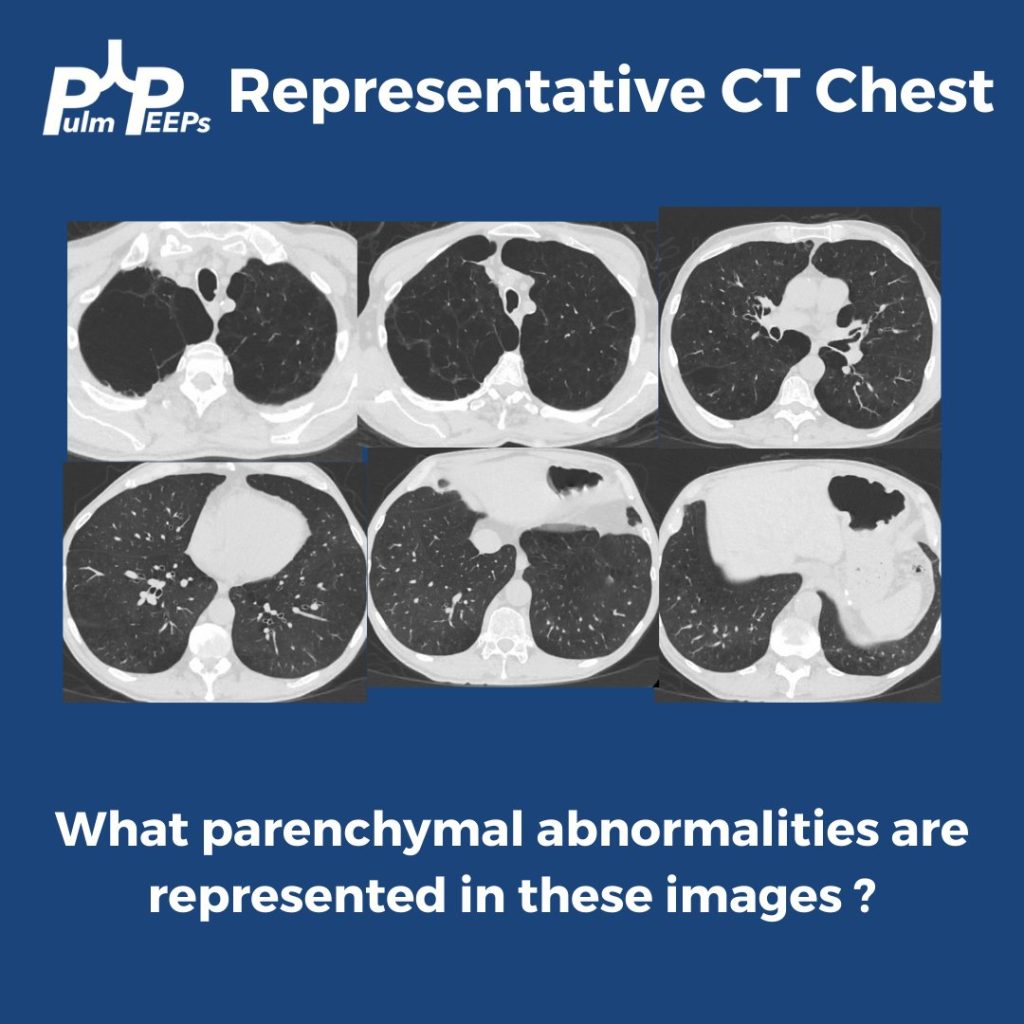
The CT chest shows all three findings as noted below.
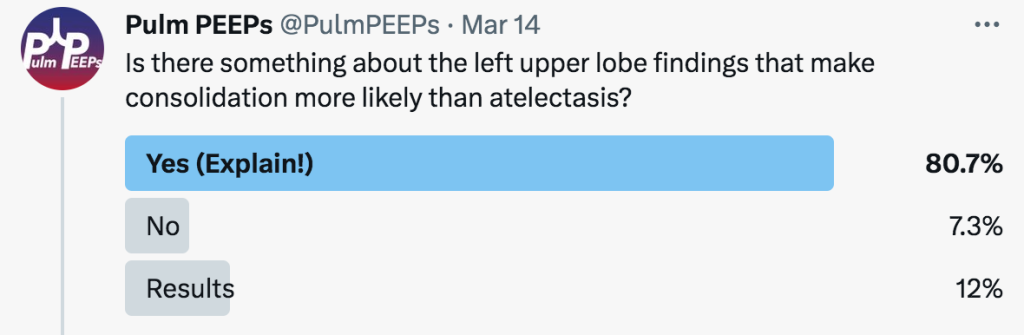
Yes! There is still aeration in some of the upper lobe, which would not be the case if this were caused by profound atelectasis. Also, atelectasis of such a large territory of the lung would usually cause traction on surrounding structures.
Having seen the CT, can you explain why the x-ray showed aeration in the inferior, left hemithorax? This is from the overlap of the left upper and lower lobes when viewed anteriorly. The sagittal view of the CT demonstrates this nicely.