Today we’re visiting the University of New Mexico for another interesting entry in our Fellows’ Case Files.
Meet Our Guests
Neel Vahil is a second-year internal medicine resident at the University of New Mexico. He completed medical school at New York Medical College and is planning on applying to pulmonary critical care fellowship programs.
Ishan Patel is a third year PCCM fellow at the University of New Mexico and will be pursuing a second fellowship in clinical informatics this year. He completed medical school and residency in Internal Medicine at Oregon Health & Science University. His fellowship research has focused on clinical outcomes of intensivist-led ECMO programs.
Dr. Lucie Griffin completed her internal medicine residency and PCCM fellowship at the University of New Mexico and is currently the Director of the Albuquerque VA medical intensive care unit.
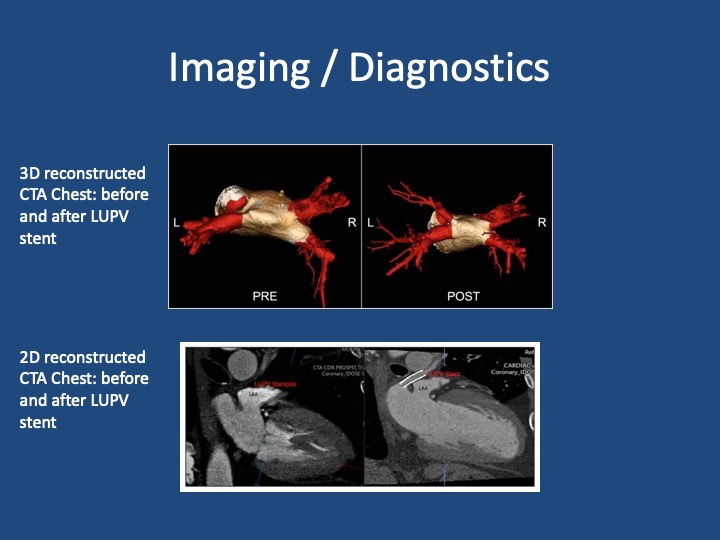
Case Presentation
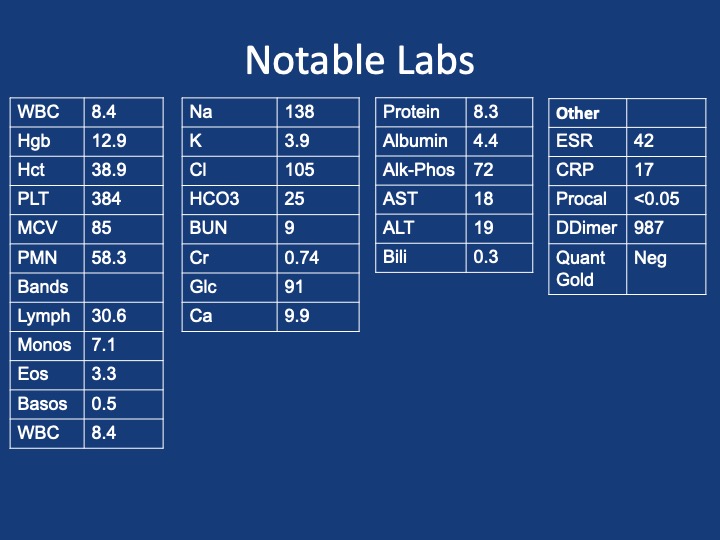
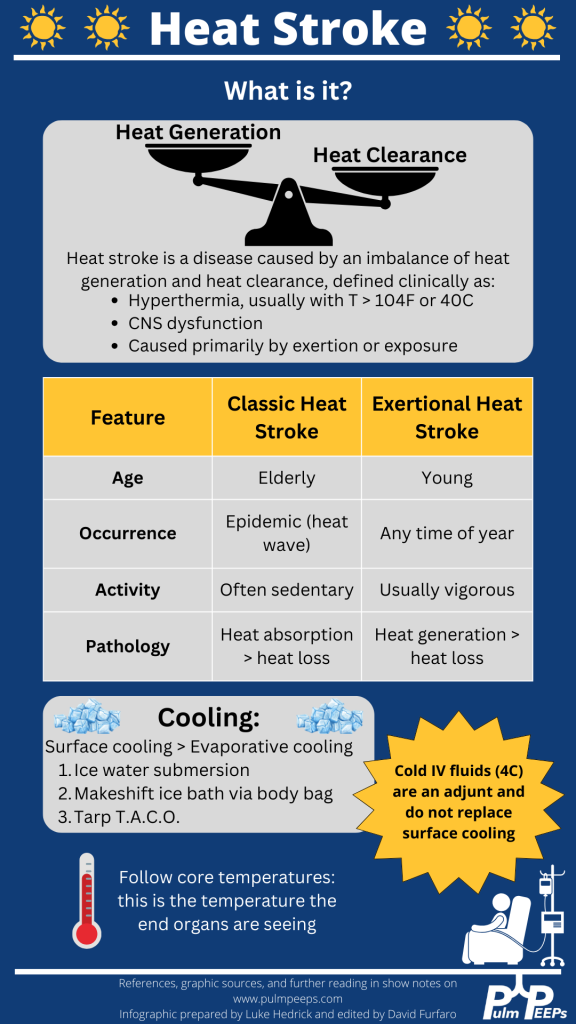
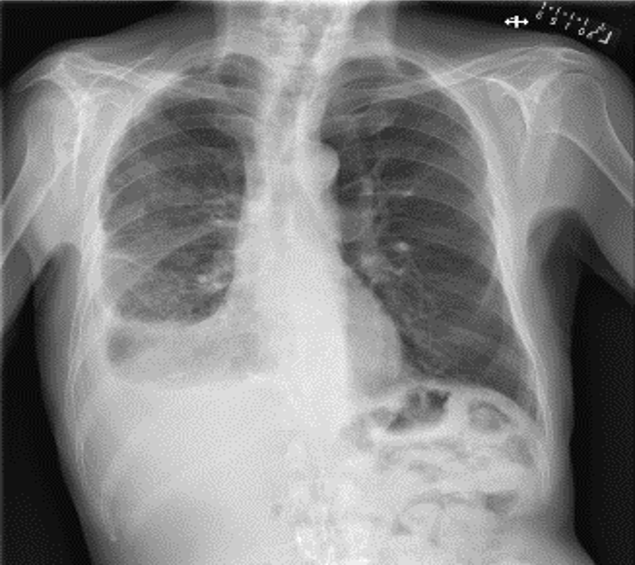
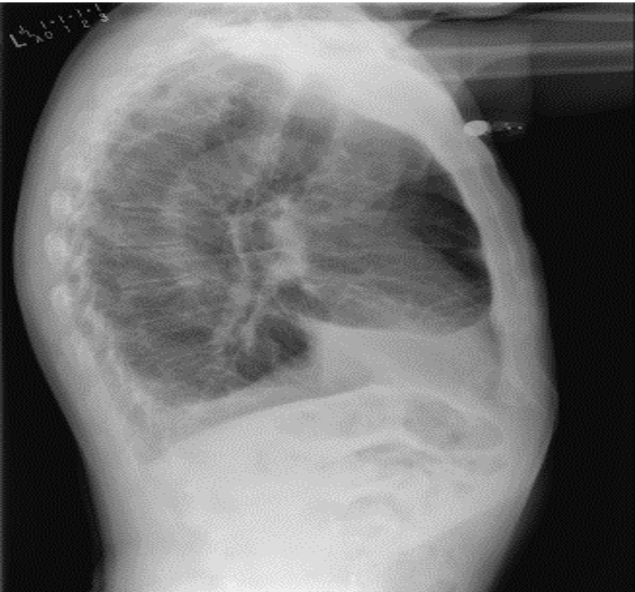
A 69 year old male veteran who presents with 6 weeks of weight loss, cough, and malaise. He has ongoing tobacco use, and history of rheumatoid arthritis on HCQ and weekly MTX with etanercept, which he had stopped taking in the three prior months. Vitals: Afebrile, mildly tachycardic to 101, BP of 93/59, saturating appropriately on room air without any signs of respiratory distress
Key Learning Points
References and Further Reading
Komarla A, Yu GH, Shahane A. Pleural effusion, pneumothorax, and lung entrapment in rheumatoid arthritis. J Clin Rheumatol. 2015;21(4):211-215.
Boddington MM, Spriggs AI, Morton JA, Mowat AG. Cytodiagnosis of rheumatoid pleural effusions. J Clin Pathol. 1971;24(2):95-106.
Balbir-Gurman A, Yigla M, Nahir AM, Braun-Moscovici Y. Rheumatoid pleural effusion. Semin Arthritis Rheum. 2006;35(6):368-378
Podcast: Play in new window | Download
Subscribe: Apple Podcasts | Spotify | Amazon Music | Android | iHeartRadio | Podcast Index | RSS