Furf and Monty are back today with another Pulm PEEPs Pearls episode, and discussing the use of methylene blue for patients with septic shock. They review the clinical scenarios when this comes up, the mechanism, some key data, and some take aways, all in 15 minutes! Let us know any other topics you’d like covered on the show and make sure to like, give us 5 stars, and subscribe wherever you’re listening to this podcast.
This episode was prepared in conjunction with George Doumat MD. Goerge is an internal medicine resident at UT Southwestern and joined us for a Pulm PEEPs – BMJ Thorax journal club episode. He is now acting as a Pulm PEEPs Editor for the Pulm PEEPs Pearls series.
Key Learning Points
Clinical context: when does methylene blue even come up?
This is not a first-line sepsis drug.
It’s considered in catecholamine-refractory vasoplegic septic shock, typically when:
Norepinephrine is at high dose
Vasopressin is on board
Often a 3rd or 4th vasopressor is being used (e.g., phenylephrine, angiotensin II)
The phenotype is strongly vasodilatory/vasoplegic (warm, distributive shock) rather than primarily cardiogenic.
Mechanism of action (why it might help)
Methylene blue:
Inhibits inducible nitric oxide synthase and guanylate cyclase.
Blunts excess nitric oxide and cyclic GMP–mediated vasodilation, which are key in vasoplegic sepsis.
Practical translation:
It restores vascular tone and can make the vasculature more responsive to catecholamines.
It’s also used in post-CPB vasoplegia (e.g., after cardiac surgery, especially in patients on ACE inhibitors) and has migrated from that world into ICU sepsis practice.
Typical dosing strategy (as described in the episode)
If there’s a response, consider a continuous infusion or repeat bolus.
Key nuance: unlike other pressors that start as drips, methylene blue is often trialed as a bolus first to see if it’s doing anything.
What does the evidence suggest?
Most data are from small, single-center, heterogeneous studies, so evidence quality is low. Meta-analyses and systematic reviews (through ~2024–25) suggest:
Hemodynamics
Can increase MAP (roughly 1–10 mmHg across studies).
May shorten total vasopressor duration (one meta-analysis ~30 hours less, though this is not definitive).
Secondary physiologic effects
Some small improvements in PaO₂/FiO₂ (P/F) ratio in certain studies.
Clinical outcomes
Possible reduction in hospital length of stay (≈ up to 2 days in some pooled analyses).
Some signal toward lower short-term mortality, but:
Studies are small
Heterogeneous
Evidence is very low certainty
Bottom line:
There’s a repeatable signal that methylene blue:
Raises MAP
Helps reduce catecholamine requirements
But hard clinical outcomes (mortality, LOS, ventilator days) remain uncertain.
Safety profile & important adverse effects
Things to watch for:
Methemoglobinemia
Serotonin syndrome
Especially in patients on SSRIs, though in life-threatening refractory shock the hosts still lean toward using it with caution.
Pulse oximeter artifact
Can distort SpO₂ readings.
Urine discoloration
Blue/green urine—benign but striking.
Notably:
Methylene blue is both a treatment for and a potential cause of methemoglobinemia, depending on context and dosing.
Guidelines & where it fits in practice
Surviving Sepsis Campaign 2021:
Does not recommend methylene blue for routine use in septic shock.
No major critical care society includes it in standard septic shock bundles or protocols.
The hosts frame methylene blue as:
A rescue therapy, not guideline therapy.
Something to consider only in refractory vasoplegic shock, ideally with:
Today, we’re virtually visiting the University of Virginia for another Fellows’ Case Files. This is a fantastic case that covers ARDS, the infectious work up of an immunosuppressed patient, and the evaluation of undifferentiated shock. Please let us know what you think of the episode and always feel free to reach out with interesting cases!
Meet Our Guests
John Popovich completed his residency training and chief year at UVA and has stayed on there for his pulmonary and critical care fellowship.
Tim Scialla is an associate professor of medicine at UVA. He completed his residency and fellowship at Johns Hopkins Hospital where he was also an ACS. His clinical and research focuses are advanced airways disease. He is also the program director of the PCCM fellowship.
Matt Freedman completed his residency training at Virginia Commonwealth University and is currently a second year fellow at University of Virginia.
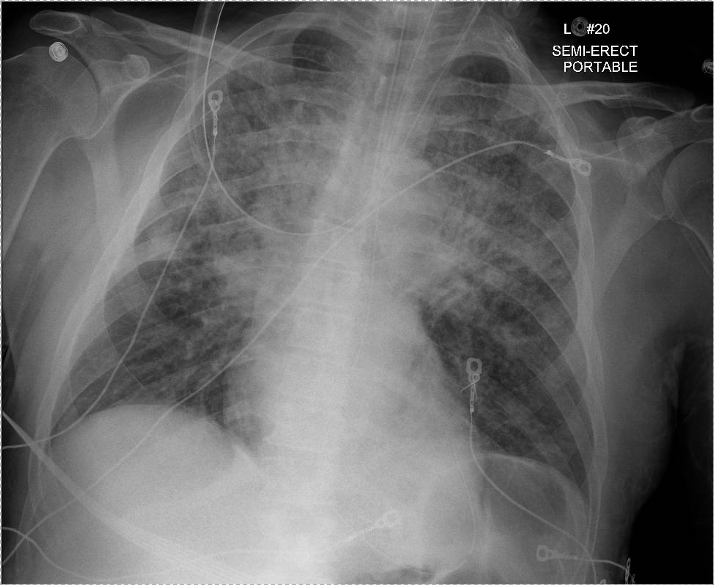
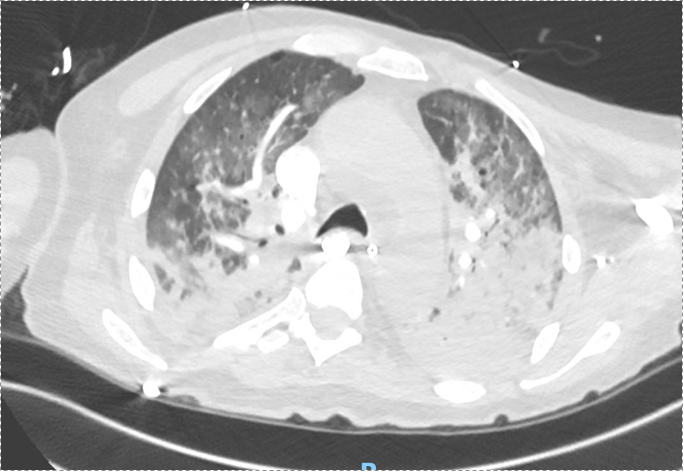
Case Presentation
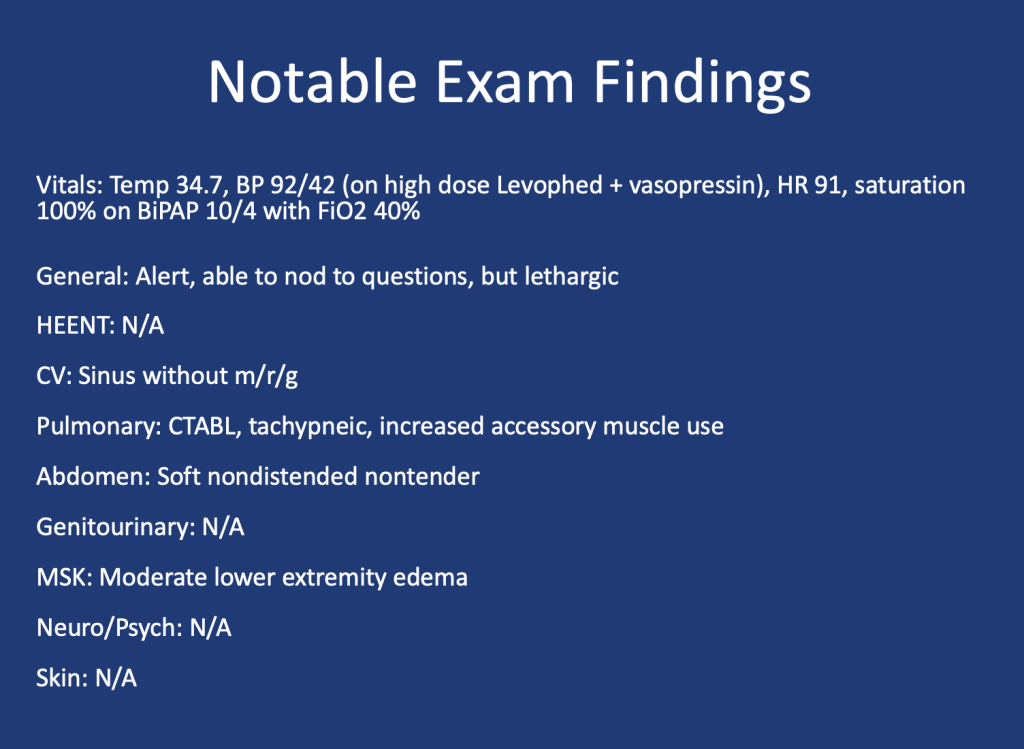
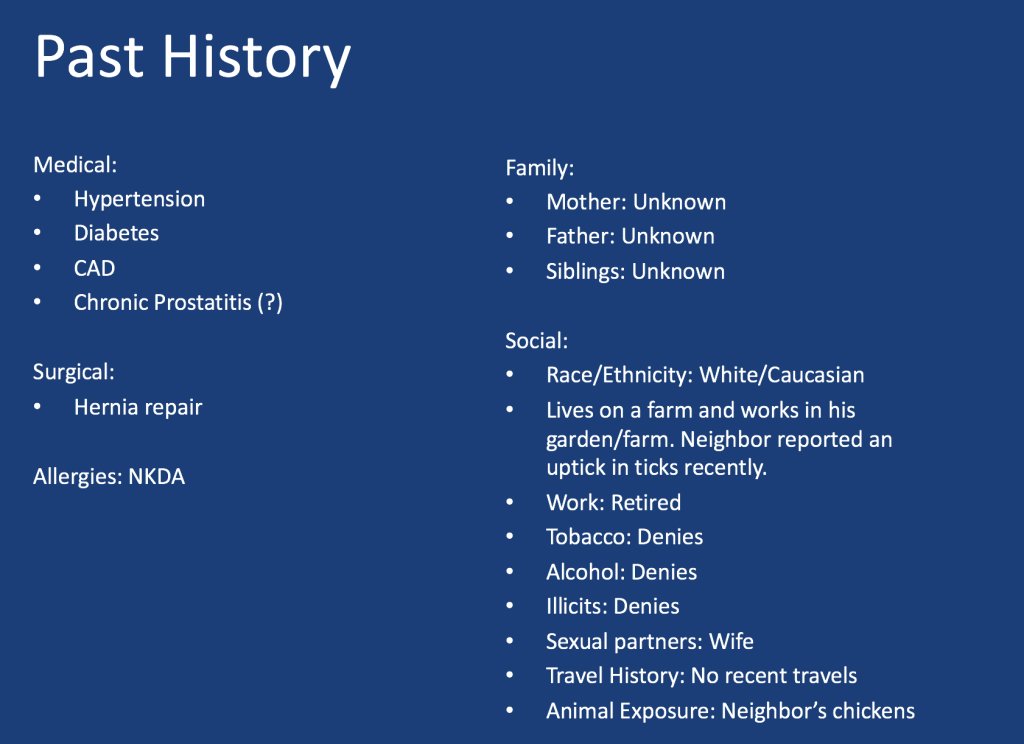
Patient: 52-year-old male with psoriasis, HIV/AIDS (CD4 count: 71), presenting with progressive shortness of breath, fever, non-productive cough, and weight loss.
We are excited to be back with a Rapid Fire Journal Club. Today’s episode is hosted by PulmPEEPs Associate Editor, Luke Hedrick, and will delve into the ANDROMEDA-SHOCK trial published in JAMA in 2019.
Meet our Guests
Jose Meade Aguilar is a second year Internal Medicine resident at Boston University Medical Campus (BUMC).
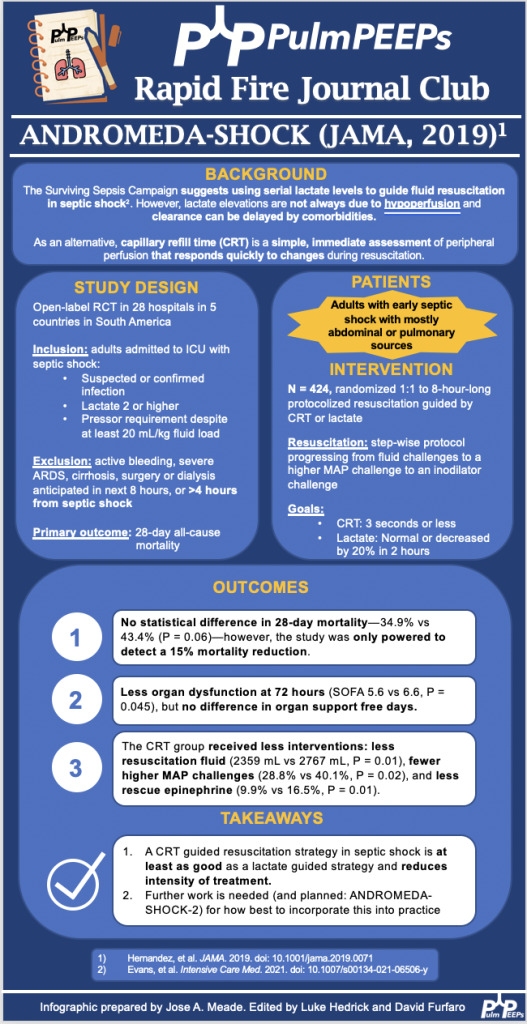
Article and Reference
Today the discussion highlights the ANDROMEDA-SHOCK trial (JAMA, 2019) which evaluated whether resuscitation guided by capillary refill time (CRT) is superior to lactate-guided resuscitation in reducing mortality in patients with septic shock.
Today we’re back with another stop on our Fellows’ Case Files journey and making our way to the University of Rochester. Tune in to hear about this fascinating case and learn some key teaching points along the way.
Meet Our Guests
Dr. Shiv Patel completed his IM residency and a Chief year at the California Pacific Medical Center- Van Ness Campus and is currently a second-year PCCM fellow at the University of Rochester.
Dr. Mary Anne Morgan is an Associate Professor of Medicine and the Fellowship Program Director for the PCCM Fellowship at the University of Rochester. Her clinical interests range from the care of critically ill patients in the ICU to the diagnosis and management of rare lung disease in her role as Director of the University of Rochester LAM Clinic. She loves unwrapping clinical reasoning with trainees, exploring issues around communication and teamwork in the ICU, and is excited about curriculum revitalization in the growing URMC PCCM fellowship program.
Case Presentation
A 75 y.o. female with a history of Hypertension, Hyperlipidemia, and Type 2 Diabetes presented for evaluation of hypoglycemia and generalized fatigue. She had felt poorly for about a week with symptoms of back pain, generalized weakness, and dyspnea, all of which acutely worsened on the day of presentation.
She was found to be hypoglycemic with a blood glucose level in the to 40’s. Initial vital signs included a heart rate of 56, blood pressure of 70/40, respiratory rate of 30, and temperature of 28.5 degrees Celsius.
Key Learning Points
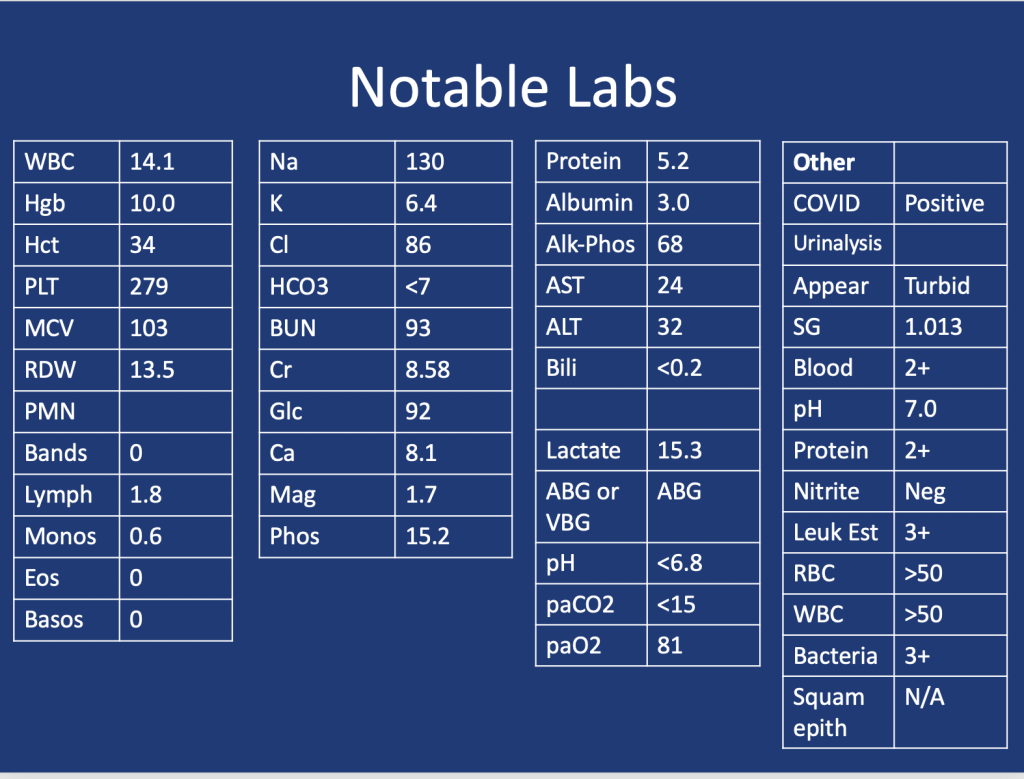
Lactic Acidosis: Type A, Type B and Type D
Type A: Typically secondary to conditions that impair oxygen delivery (respiratory failure, PE) to tissues or decrease tissue perfusion (severe anemia, shock). Patients typically present with hypotension, tachycardia, tachypnea, altered mental status, and signs of organ dysfunction.
Type B: Typically secondary to conditions that directly affect cellular metabolism or lactate clearance and characterized by the presence of hyperlactatemia without evidence of tissue hypoperfusion or hypoxia. Conditions associated include liver dysfunction (e.g., liver failure, cirrhosis), malignancies (especially hematological malignancies), medications/toxins (e.g., metformin, cyanide poisoning), inborn errors of metabolism, and mitochondrial disorders.
Type D: Less common presentation and can be seen in patients with short gut syndrome.
References
1.Blough B, Moreland A, Mora A Jr. Metformin-induced lactic acidosis with emphasis on the anion gap. Proc (Bayl Univ Med Cent). 2015 Jan;28(1):31-3. doi: 10.1080/08998280.2015.11929178. PMID: 25552792; PMCID: PMC4264704.
2.Callelo et al. Extracorporeal Treatment for Metformin Poisoning: Systematic Review and Recommendations From the Extracorporeal Treatments in Poisoning Workgroup. DOI: 10.1097/CCM.0000000000001002
3.Friesecke, S., Abel, P., Roser, M. et al. Outcome of severe lactic acidosis associated with metformin accumulation. Crit Care14, R226 (2010). https://doi.org/10.1186/cc9376
We’re starting off 2024 with a bang!! Today we’re hosting another expert Roundtable discussion and we’re joined by internationally recognized experts in the field. We’ll tackle everything from teaching about sepsis, to how to incorporate guidelines into education and practice, to future research directions in the field. This is a can’t-miss discussion. Let us know what you think and other sepsis questions you have!
Meet Our Guests
Dr. Derek Angus is a Professor at the University of Pittsburgh where he holds the Mitchell P. Fink Endowed Chair in Critical Care Medicine and is the Chair of the Department of Critical Care Medicine. He is a world-renowned researcher in a range of critical care topics including sepsis, has hundreds of publications, and has led numerous NIH-funded studies.
Dr. Hallie Prescott is an Associate Professor in Pulmonary and Critical Care Medicine at the University of Michigan. She is the Co-Chair of the Surviving Sepsis Campaign Guidelines and is also an internationally recognized expert due to her research in improving sepsis outcomes. She has been recognized by both medical journals and professional societies for her outstanding contributions to the field.
Summary of Episode Discussion Topics
1. Sepsis Guidelines and Education
Surviving Sepsis Guidelines: Stressed as essential reading for professionals in pulmonary and critical care. They provide a structured approach to sepsis management.
Teaching Approaches: Transition from during-rounds teaching to focused, separate teaching sessions for trainees. Emphasizes the need to go beyond guidelines to include discussions on seminal articles, management strategies, and areas lacking robust data.
2. Clinical Skills and Decision Making in Sepsis Care
Early Recognition and Polypharmacy: Highlighted the need for timely sepsis identification and caution against excessive polypharmacy.
Mental Models in Care: Encourages building comprehensive mental models for understanding sepsis, stressing the importance of not just treating symptoms but understanding underlying causes.
3. Implementation of Sepsis Guidelines
Guideline Application in Bedside Care: Discusses the challenge of applying guidelines while considering patient-specific factors.
Fluid Resuscitation Practices: Identifies fluid resuscitation as a key area for improvement, with a shift towards more conservative approaches.
Overcoming Institutional Barriers: Addresses the fear of causing harm as a significant barrier to guideline implementation and emphasizes the need for balanced decision-making.
4. Advances in Sepsis Care and Prevention
Pre-Hospital Sepsis Management: Explores the role of early intervention in community settings and the potential of wearables for early detection.
Paramedic Role in Early Antibiotic Administration: Underlines the importance of starting antibiotics in the ambulance for suspected sepsis cases.
5. Recovery and Post-Discharge Care
Post-Discharge Initiatives: Focuses on improving handoffs from ICU to ward and from hospital to home. Highlights the importance of medication reconciliation and clear communication with primary care.
Challenges in Continuity of Care: Discusses the need for clear documentation and communication during patient transitions to ensure continuity of care.
6. Future Directions in Sepsis Treatment and Research
Phenotyping for Targeted Treatment: The potential of identifying patient subgroups through phenotyping for more effective, tailored treatments.
Adaptive Trial Designs: Advocates for large-scale adaptive platform trials that can test multiple interventions across diverse patient populations.
7. Personal Involvements and Perspectives
Experts’ Current Work: The panelists share their ongoing projects and research in sepsis care, reflecting a commitment to advancing the field through comprehensive and adaptive approaches.
We are extremely excited to be hosting this episode in collaboration with CardioNerds! We have known Amit and Dan for many years, and they have been huge supporters of Pulm PEEPs, so it is an honor to address a topic we’re all interested in together.
We are joined by experts in the field today to discuss acute, decompensated right ventricle failure in patients with Pulmonary Arterial Hypertension (PAH). This topic can be quite intimidating, so we hope this will serve as a valuable guide for anyone who encounters a patient like this in the ICU.
Meet Our Guests
Leonid “Leon” Mirson is an internal medicine resident at the Johns Hopkins Hospital Osler Medical Residency and an Associate Editor here at Pulm PEEPs. He was born in Ukraine and moved to Philadelphia in early childhood with his family. He received his undergraduate degree from the University of Pittsburgh where he studied biomedical engineering and received his medical degree from the University of Pittsburgh School of Medicine. His current interests include pulmonary and critical care medicine with a focus on pulmonary hypertension as well as medical education. He is a rising PCCM fellow at the University of Pennsylvania.
Bhavya Varma completed her medical school at the University of Pittsburgh, her internal medicine residency at Johns Hopkins, and is a rising Cardiology fellow at NYU. She is interested in medical education and has done work with CardioNerds during her residency.
Mardi Gomberg-Maitland is a Professor of Medicine at George Washington University. She serves as the Medical Director of the Pulmonary Hypertension Program at George Washington Hospital. She completed her medical degree at Albert Einstein College of Medicine, completed her residency at the Weill-Cornell Medical Center, and completed her fellowship in cardiovascular diseases at Mount Sinai Medical Center. Her research focus is on understanding the epidemiology of pulmonary hypertension and the development of novel therapeutics and biomarkers. Dr. Gomberg-Maitland is internationally known for her work, she has had extensive grant funding and has published over 150 articles, abstracts, reviews, and chapters.
Rachel Damico is a pulmonologist and an Associate Professor of Medicine at Johns Hopkins Hospital, where she is also the Associate Director of the physician-scientist training program. Dr. Damico received her medical degree and doctoral degree in Molecular and Cellular biology from the University of Pennsylvania. She completed her residency in the Osler Internal Medicine training program and continued on as a PCCM fellow at Johns Hopkins. She has quickly achieved an international reputation in the field of pulmonary vascular biology and both basic and translational research, as well as clinical excellence, in Pulmonary Arterial Hypertension.
Patient Presentation
A 21-year-old woman with a past medical history notable for congenital heart disease (primum ASD and sinus venosus with multiple surgeries) complicated by severe PAH on home oxygen, sildenafil, ambrisentan, and subcutaneous treprostinil is presenting with palpitations, chest pain, and syncope. She presented as a transfer from an outside ED where she arrived in an unknown tachyarrhythmia and had undergone DCCV due to tachycardia into the 200s and hypotension. On arrival at our hospital, she denied SOB but did endorse nausea, leg swelling, and poor medication adherence. Her initial vitals were notable for a BP of 80/50, HR 110, RR 25, and saturating 91% on 5L O2. On exam, she was uncomfortable appearing but mentating well. She had cool extremities with 1-2+ LE edema. Her JVP was 15cm H2O. She has an RV Heave and 2/6 systolic murmur. Her lungs were clear bilaterally. Her labs were notable for Cr 2.0, an anion gap metabolic acidosis (HCO3 = 11), elevated lactate (4.1), elevated troponin to 14, and a pro-BNP of ~5000. Her CBC was unremarkable. Her EKG demonstrated 2:1 atrial flutter at a rate of 130.
Key Learning Points
Diagnosing RV failure in patients with PH:
RV dysfunction and RV failure are two separate entities. RV dysfunction can be measured on echocardiography, but RV failure can be thought of as a clinical syndrome where there is evidence of RV dysfunction and elevated right sided filling pressures.
RV failure is a spectrum and can present with a range of manifestations from evidence of R sided volume overload and markers of organ dysfunction, all the way to frank cardiogenic shock. Most patients with RV failure are not in overt shock.
One of the first signs of impending shock in patients with RV failure is the development of new or worsening hypoxemia. Patients with decompensated RV failure approaching shock often do not present with symptoms classic for LV low flow state. Instead, hypoxia 2/2 VQ mismatching may be the first sign and they can be otherwise well appearing. Particularly because patients with PH tend to be younger, they can often appear compensated until they rapidly decompensate.
Causes of decompensation for patients with RV dysfunction and PH:
Iatrogenesis (inadvertent cessation of pulmonary vasodilators by providers, surgery if providers are not familiar with risks of anesthesia), non-adherence to pulmonary vasodilators (either due to affordability issues or other reasons), infections, arrhythmias (particularly atrial arrhythmias), and progression of underlying disease.
Patients with atrial arrhythmias (atrial flutter or atrial fibrillation) and pulmonary hypertension do not tolerate the loss of the atrial kick well as it contributes a significant amount to their RV filling and impacts their cardiac output. It is often difficult to determine if the atrial arrhythmia is a cause or effect of decompensated RV failure, but its presence is associated with a worse prognosis. Efforts should be made to re-establish normal sinus rhythm in patients with decompensated RV failure and atrial arrhythmias.
A patient’s home PH medications should never be stopped for any reason upon admission unless on the basis of recommendations by a pulmonary hypertension provider as this is often a cause of decompensation inpatient
Interpreting findings on echocardiogram:
Echo is a useful screening tool. When interpreting evidence of RV dysfunction, it is important to look at the global picture and not just one measurement.
RVSP, though commonly reported, may be of limited value when evaluating for decompensation. It’s a function of blood pressure, heart rate, and cardiac output. RVSP may even decline as shock worsens.
TAPSE is useful as a marker of RV dysfunction if it is reduced, but it is difficult to follow over time and only gives information about cardiac function around the annulus; it may be normal even when apical RV function is depressed. RV fractional area of change may be more useful for global RV function. It is important to pay attention to the RV size overall, the degree of TR, and the presence of effusion all of which are associated with RV dysfunction.
Tips regarding the interpretation of invasive hemodynamics:
Cardiac output by thermodilution is the standard way to calculate PVR. Despite the degree of TR that is typically present, it is thought to be a better representation of cardiac output than the estimated Fick calculation.
Our experts agree that routine monitoring of invasive hemodynamics for acute decompensated RV failure is likely not helpful and has significant risks. A good external volume exam or CVP off a central venous catheter + central venous saturation will likely be all you need to navigate a patient with shock secondary to RV failure. A right heart catheterization (should be only done under fluoroscopy for patients with large RVs) may be helpful if the etiology of shock is unclear.
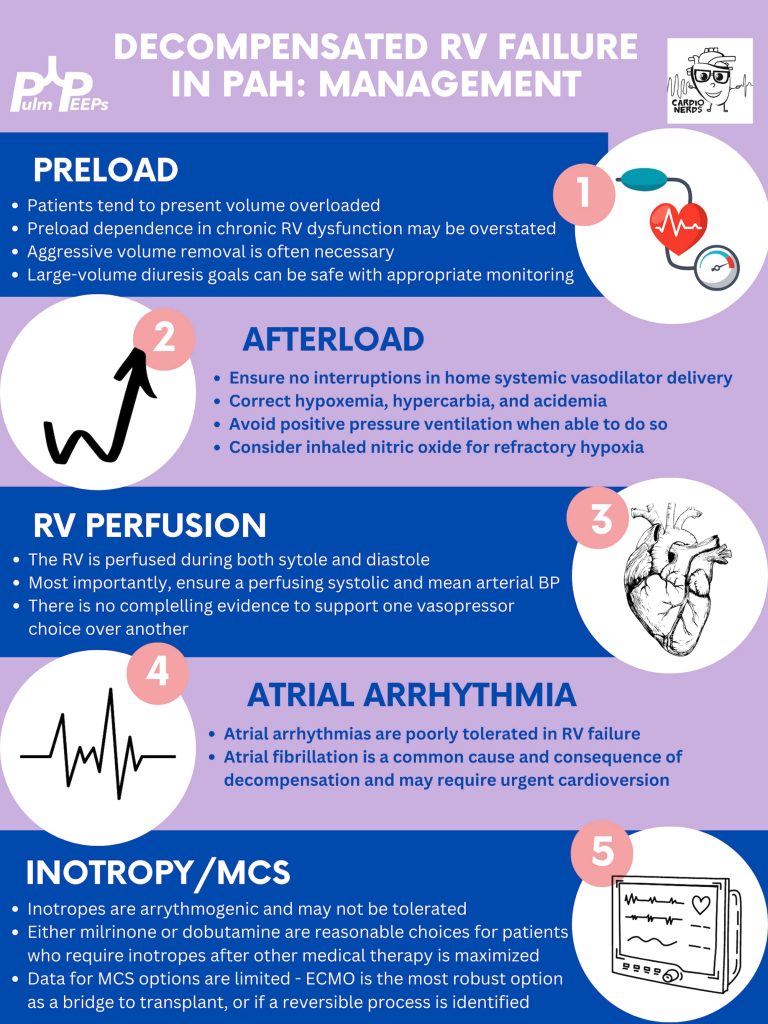
Management of decompensated RV failure in patients with pulmonary hypertension
Managing preload is of utmost importance, perhaps the most important tenant of management of decompensated RV failure. The overwhelming majority of patients with PH and decompensation are volume overloaded, it is exceptionally rare that someone would be dry. Furthermore, the myth that the RV is “preload responsive” is only true in the setting of acute RV injury (eg. RV infarction) and not so in patients with acute on chronic RV dysfunction. It is important to optimize preload in someone in decompensated RV failure and it is safe to do this more rapidly than traditionally taught. Exact goals varied between our experts, but anywhere from 2-4L net negative per day is reasonable especially if the patient is hemodynamically tolerating the fluid removal. If the patient is not responding to diuretics, hemodialysis with ultrafiltration may be necessary to optimize the patient.
Afterload is the next tenant of management. Optimizing the following parameters will reduce the patient’s pulmonary vascular resistance and reduce afterload to the right ventricle.
— Avoiding hypoxic pulmonary vasoconstriction, liberalize the patient’s O2 goal
— Avoid permissive hypercapnia and academia in this patient population
— Do not withhold a patient’s pulmonary vasodilator until discussion with the PH team. If stopped inadvertently, restart this medication immediately. For patients with malfunctioning pumps, there is a phone number on the back that you can call for rapid troubleshooting. Sildanefil can be given IV if a patient is NPO.
— Inhaled nitric oxide can improve oxygenation and reduce afterload
— Intubation and mechanical ventilation greatly increase PVR and are poorly tolerated. Exacting care must be taken to titrate PEEP and tidal volume, and avoid intubation when possible.
— Starting a new systemic pulmonary vasodilator in decompensated RV failure may be considered under close guidance from the pulmonary hypertension team
Management of atrial arrhythmias:
As above, patients with severe pulmonary hypertension do not tolerate loss of sinus rhythm well. If they are decompensated, every effort should be made to re-establish normal sinus rhythm.
Management of RV perfusion:
Unlike the LV, the RV is perfused during BOTH systole and diastole. Maintaining effective coronary perfusion to the RV is essential in RV failure. For this reason, the systemic systolic pressure (as well as the mean arterial pressure) should be kept high enough to ensure that the RV is able to perfuse. There is no great body of evidence as to which pressor works best. Norepinephrine, vasopressin, and even phenylephrine are all reasonable choices to maintain appropriate perfusing blood pressure.
Inotropy:
Patients in shock and RV failure do not always require inotropes, but if they do it’s often a sign of a grim prognosis. Either dobutamine or milrinone is reasonable, but the negative effects of these drugs (arrhythmias, tachycardia, and systemic hypotension) may limit their uses.
Mechanical circulatory support:
Limited options are available. Balloon pumps and Impella devices have limited roles except in expert centers, and ECMO remains the standard of care. ECMO (either V-V or V-A) may have utility as a bridge to recovery if a reversible cause is identified, or a bridge to transplant if the patient is on the transplant list.
Goals of care:
The prognosis of a patient admitted to the ICU with acute on chronic decompensated RV failure is guarded, with very high mortality rates even if not in shock
It is important for the patient’s longitudinal pulmonary hypertension provider to discuss the prognosis and goals of care ahead of time but this is not always possible. If they are admitted, early discussions regarding code status and prognosis are essential. It may be helpful to bring in the patient’s longitudinal pulmonary hypertension doctor into these discussions if possible.
Join us as we head to Indiana University! Listen in as we discuss another great case and hear teaching points from our amazing guests.
Meet our Guests
Parth Savsani is currently an internal medicine resident at Indiana University School of Medicine. He received his undergraduate degree from the University of Wisconsin-Madison and his medical degree from the University of Illinois College of Medicine. He enjoys medical education and was selected to be the VA chief resident next year.
Maria Srour is a Pulmonary and Critical Care Fellow at Indiana University School of Medicine. She completed her internal medicine residency at Saint Louis University where she was also a chief resident, and received her medical degree from IU. She works in global health to improve care for sepsis patients in low resources settings, and is currently pursuing her MPH.
Laura Hinkle is a Indiana University die hard and has been there from her since medical school through residency and fellowship, and is now an Assistant Professor of Clinical Medicine and the Associate Program Director for the Pulmonary and Critical Care Medicine Fellowship. She will be taking over as the Program Director July 1, 2023. She is a dedicated educator and is the Key Clinical Educator for Pulmonary and Critical Care, and the Director of the Clinical Transitions Curriculum. Additionally, she is working on a Master’s Degree in Education through the University of Cincinnati.
Case Presentation
A male in her early 60s is transferred from a neighboring facility with a 1 week history of fatigue and lethargy. Three days prior to presentation he developed dyspnea and increased weakness with a near fall at home. HIs family also reported recent fevers, chills, dyspnea, and diarrhea. On his way to seek evaluation, he developed slurred speech without any other focal abnormalities.
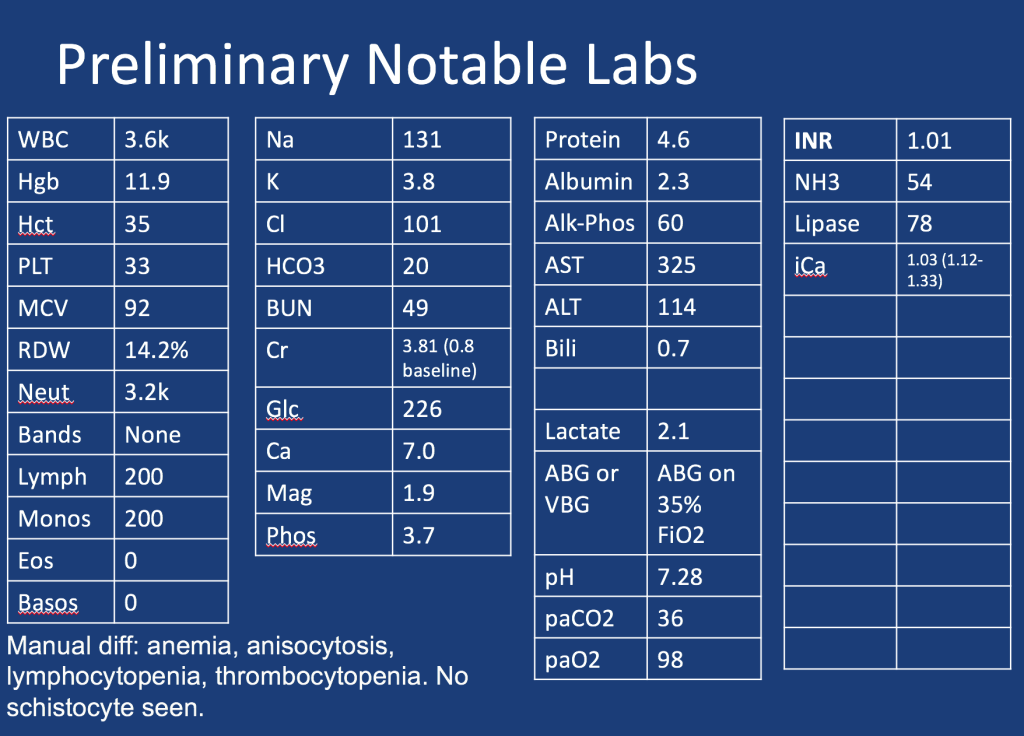
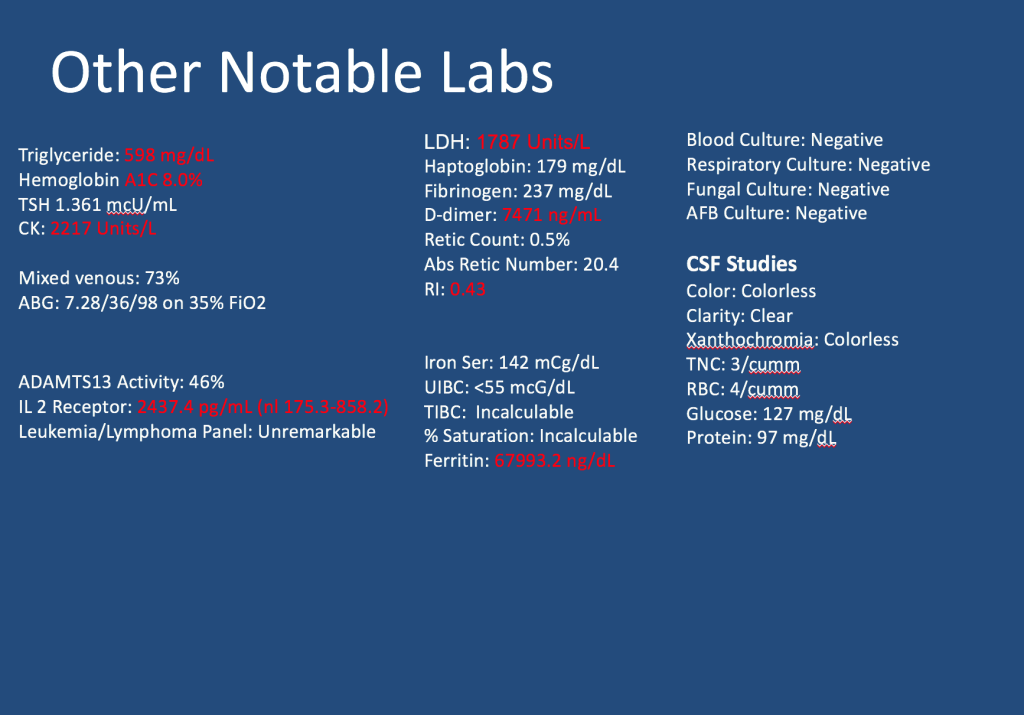
Additional information is summarized as below:
Follow along our episode to hear the final diagnosis and key teaching points from the case!
Welcome back to our Pulm PEEPs Fellows’ Case Files series! We are joined this week by a fellow and the program director from the Harvard combined PCCM fellowship at Massachusettes General Hospital and Beth Israel Deaconess Medical Center. Listen in for a great learning case and let us know on Twitter, if you have a great case to share!
Meet our Guests
Brian Rosenberg is a third year fellow at the Harvard MGH/BI program. He completed his undergraduate degree at Harvard, received his MD from Yale where he also got a PhD in cell biology, and then did his internal medicine residency at Columbia University Medical Center in NYC.
Asha is an Assistant Professor Medicine at Beth Israel Deaconess Medical Center and Harvard Medical School, and is the Program Director of the Harvard MGH/BI combined fellowship. She is also the Director of the Pulmonary Consult Service at BIDMC, was a Rabkin Fellow in Medical Education and has received multiple leadership and teaching awards
This week on Pulm PEEPs, we have another great case episode. We’re switching up the format a bit, and instead of introducing our guests in the beginning, we’ll bring them in consultants as we need to. Luckily, we’re joined by Pulm PEEPs Associated Editor Luke Hedrick to walk us through the case. Let us know your thoughts and if you have any other pearls to add!
Meet Our Guests
Rakhi Naik an Associate Professor of Medicine at Johns Hopkins Hospital and the Associate Director for the Hematology / Oncology Fellowship program. She also has a Masters in Health Sciences from the Johns Hopkins Bloomberg School of Public Health. She has expertise in an array of non-malignant hematology disorders and focuses specifically on sickle cell in her research. She is also an outstanding and dedicated educator and serves as the Chair of the American Society of Hematology Hematology-Focused Training Program Consortium to develop innovative training pathways for non-malignant heme.
Patient Presentation
A 60-year-old woman with a past medical history of hypertension, diabetes, stage 4 chronic kidney disease, COPD, HFpEF, chronic pain on methadone, hyperparathyroidism s/p parathyroidectomy that was c/b hypothyroidism now on thyroid hormone replacement, and a recent admission for nonconvulsive status epilepticus is brought to an outside hospital by EMS with encephalopathy and shaking.
When EMS gets her to the other hospital her GCS was 5, so she was intubated for airway protection and started on fentanyl and midazolam drips. Details of labs and imaging are scarce, but we know that she had a CT head that was normal, a CXR with a report of pulmonary edema, and labs with a Cr of 2.4, serum bicarbonate of 14, and a pH from a VBG of 7.1 with pCO2 of 38.
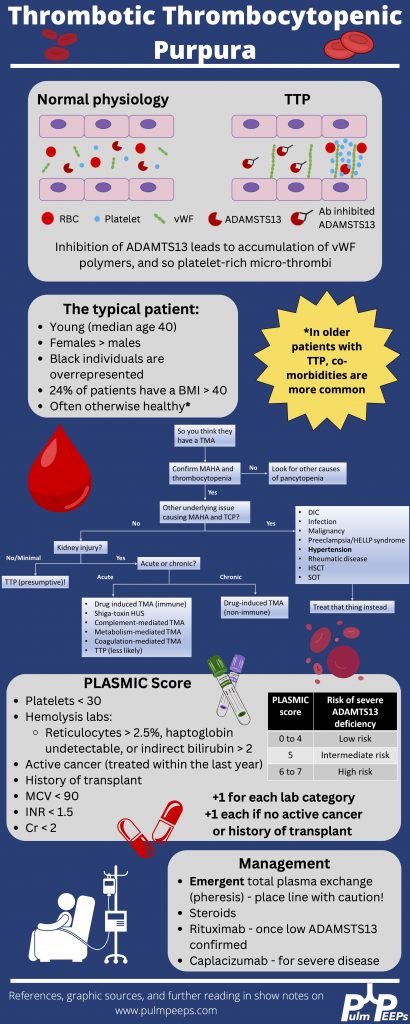
Key Learning Points
*Spoilers ahead* The infographic below highlighting key points gives away the diagnosis in this case so if you want to work through the case on your own, we recommend listening to the episode first.
We’re very excited for the second episode in our Pulm PEEPs Fellows’ Case Files series! For a reminder, the purpose of this series is to highlight and amplify the incredible clinical work that is done by pulmonary and critical care fellows, share fascinating cases, and assemble a diverse network of pulmonary and critical care educators. This week, we’re visiting the Pacific Northwest and headed to the University of Washington to meet two passionate educators, and hear about an incredible teaching case.
Meet Our Guests
Robin Stiller is a third-year pulmonary and critical care fellow at the University of Washington. Robin completed internal medicine residency training at the University of Washington and her clinical and research interests include procedural education and curriculum development.
Başak Çoruh Associate Professor of Medicine at the University of Washington School of Medicine and is the Program Director for the Pulmonary and Critical Care Fellowship. She completed her fellowship and the Teaching Scholars Program at UW. Başak has received numerous teaching and mentoring awards throughout her career and has leadership roles with ATS, CHEST as well as the APCCMPD.
Patient Presentation
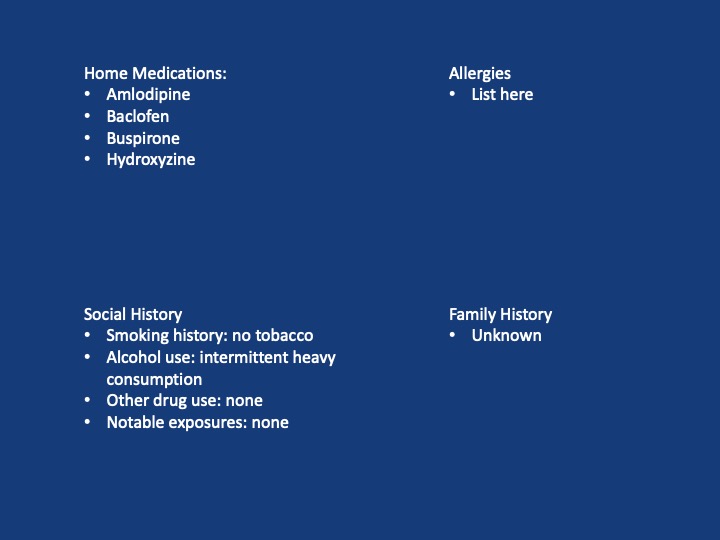
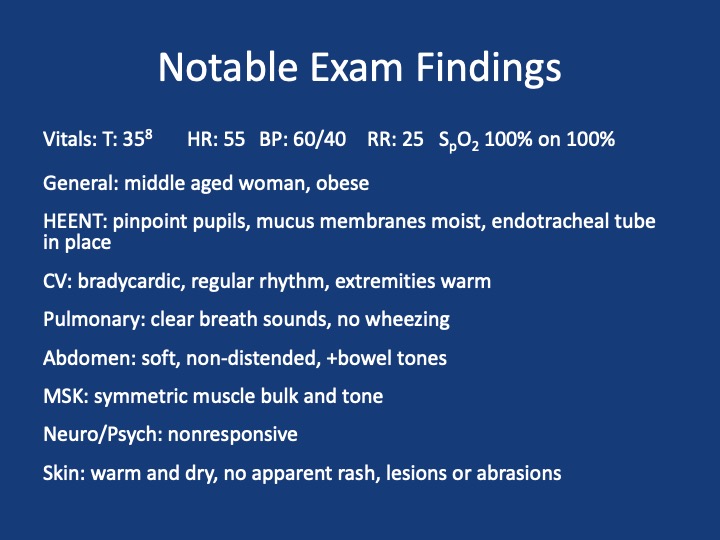
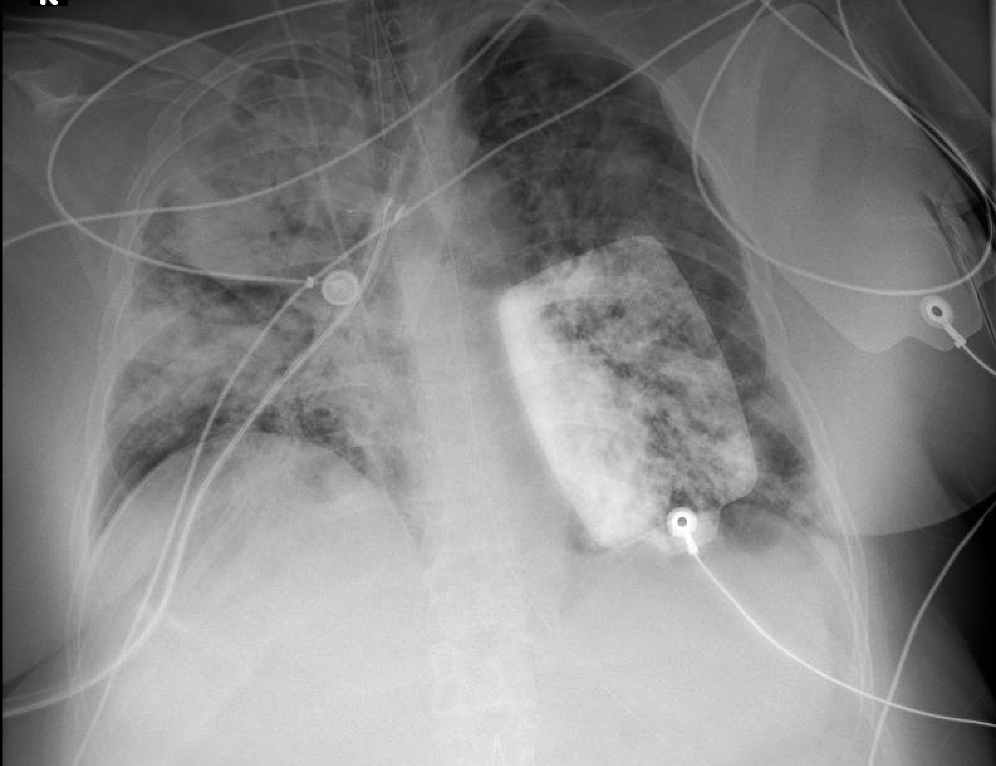
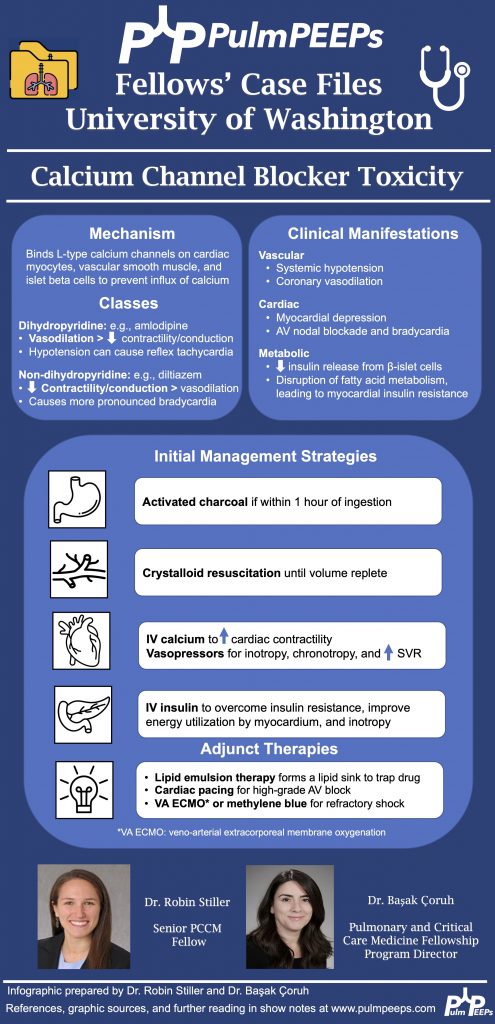
A 56-year-old woman with a history of alcohol use and depression presents after being found down at home by her boyfriend with an unknown downtime. She was found to be unresponsive and in the supine position. Her physical exam did not show any obvious trauma but the paramedics did note vomitus on her face. She received 1 L of crystalloids in the field and was intubated and brought to the ED for further management. A bag of pill bottles was found and brought with her. Her home medications include amlodipine, baclofen, buspirone, and hydroxyzine.
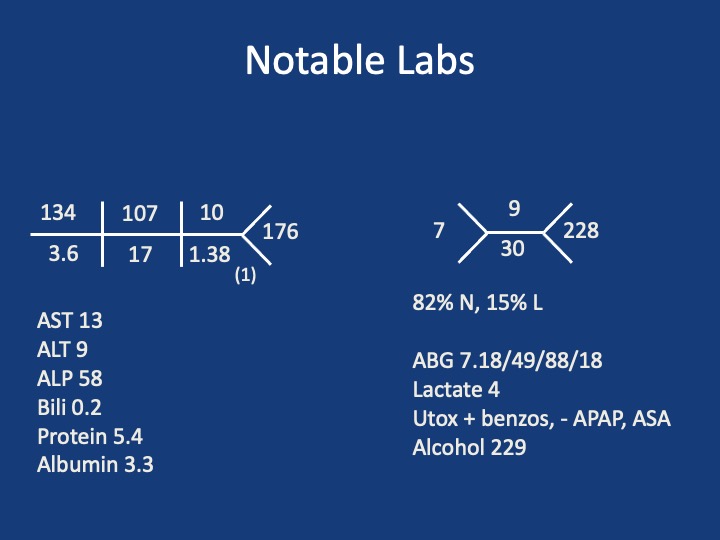
Key Learning Points
**Spoilers Ahead** If you want to think through the case on your own we advise listening to the episode first before looking at the infographic below