As we approach the end of the year, we know that the hospital and clinic keep on rolling, so here is a CXR and pulmonary differential based #RadiologyRounds if you’re on for the holiday blocks A woman in her 50s has hypoxemia after being admitted with a femur fracture
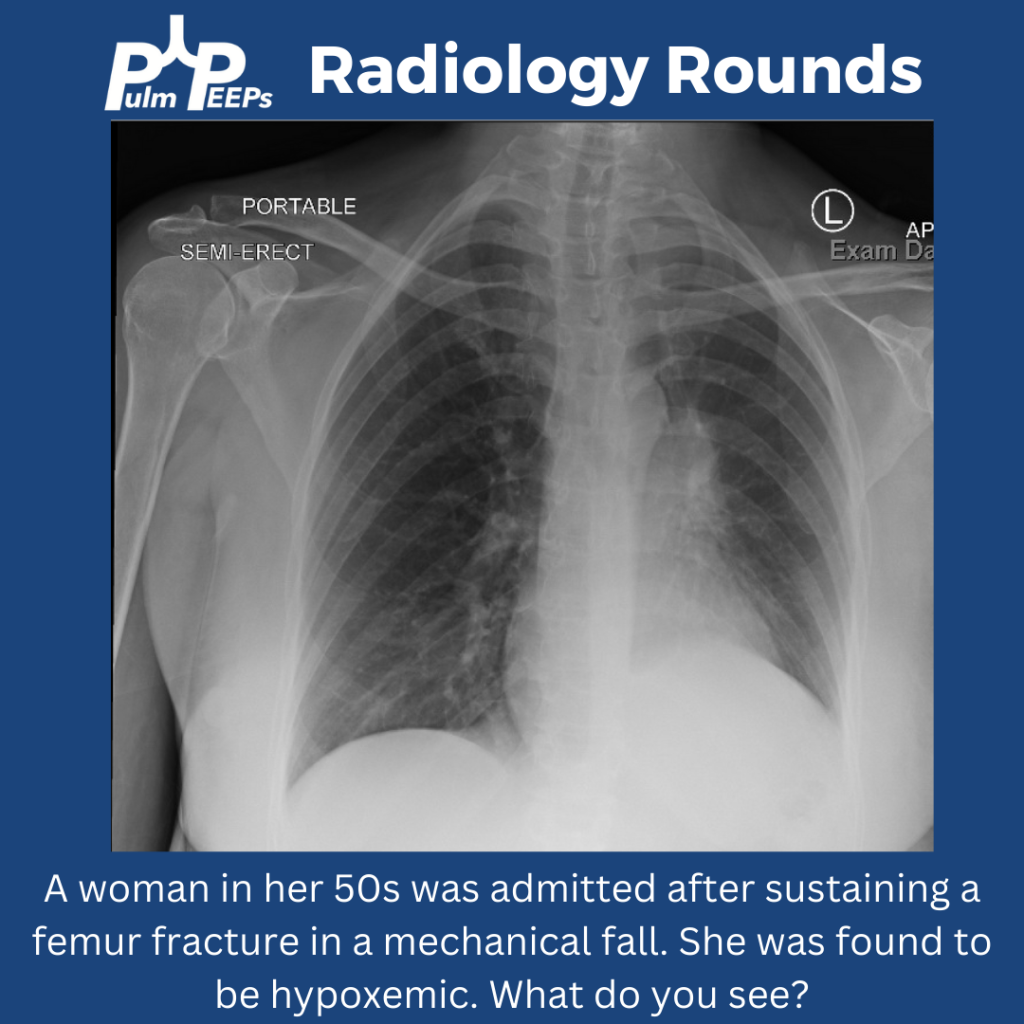
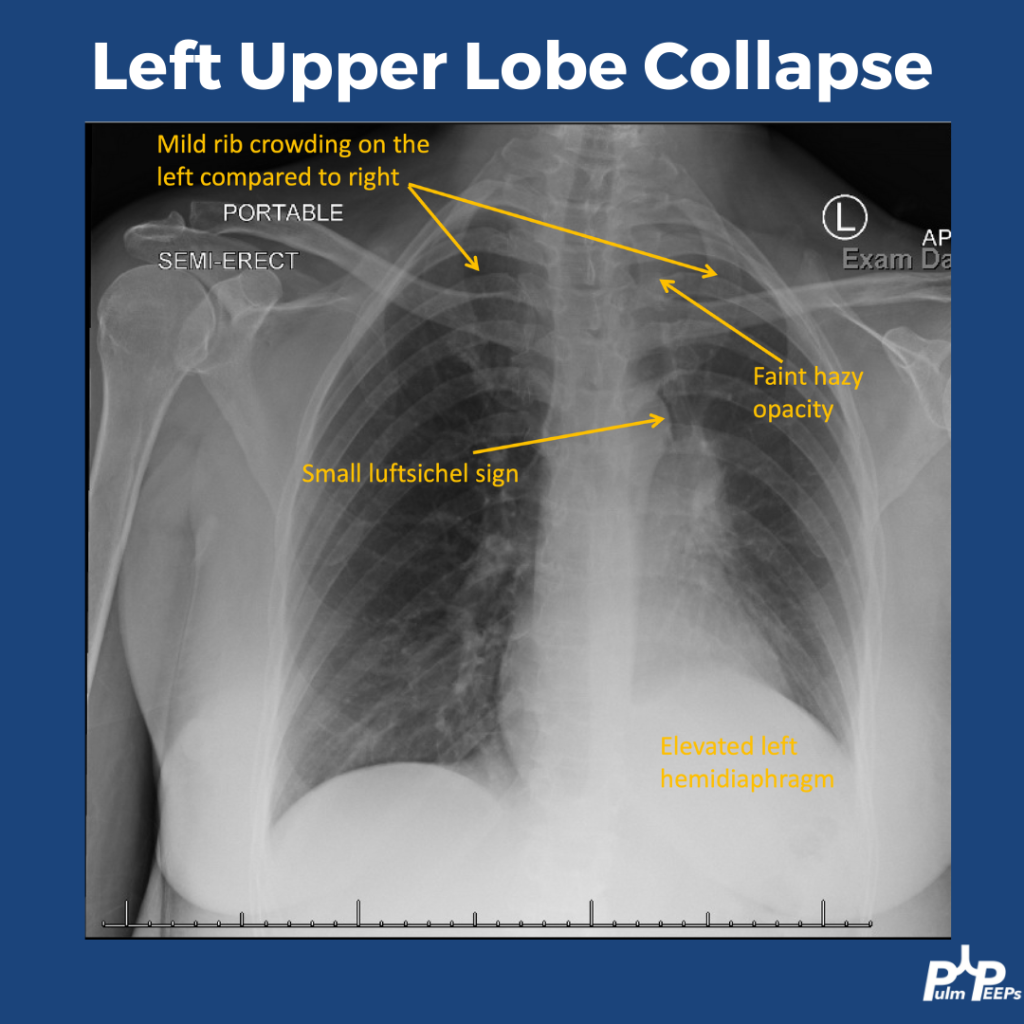
The CXR shows signs of a left upper lobe collapse. The upper lungs should be the most lucent, with increased opacity as you go down. LUL collapse can be subtle, but you can see increased haziness at the lung apex. There is also rib crowding and left hemidiaphragm elevation. You can also see a small luftsichel sign. Luftsichel sign is a thin strip of air that can be seen between the collapsed LUL and the superior mediastinum created by the still-aerated superior segment of the lower lobe. The collapse is better appreciated on CT.
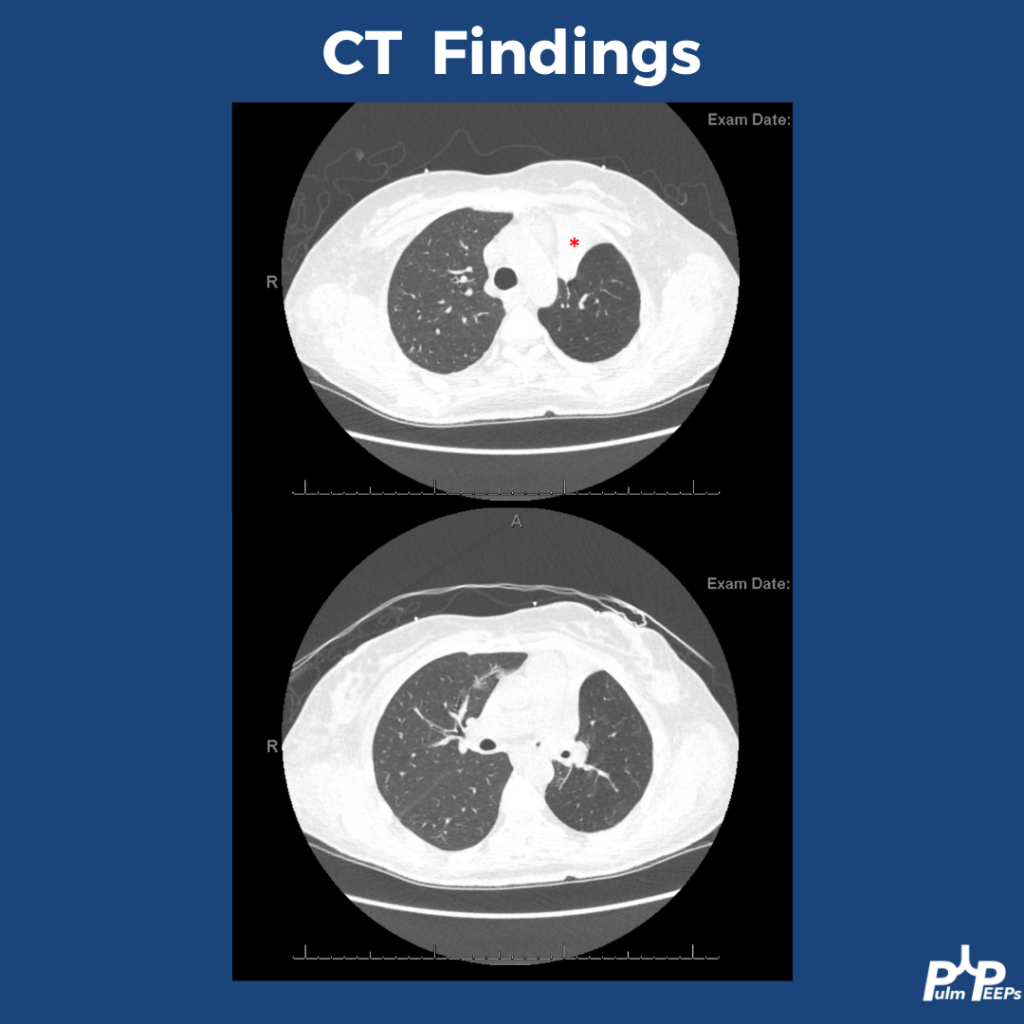
Bronchoscopy was performed to investigate the etiology of the lobar collapse. On the bronchoscopy there was an endobronchial lesion completely occluding the left upper lobe bronchus. The mass was biopsied and sent for histopathology
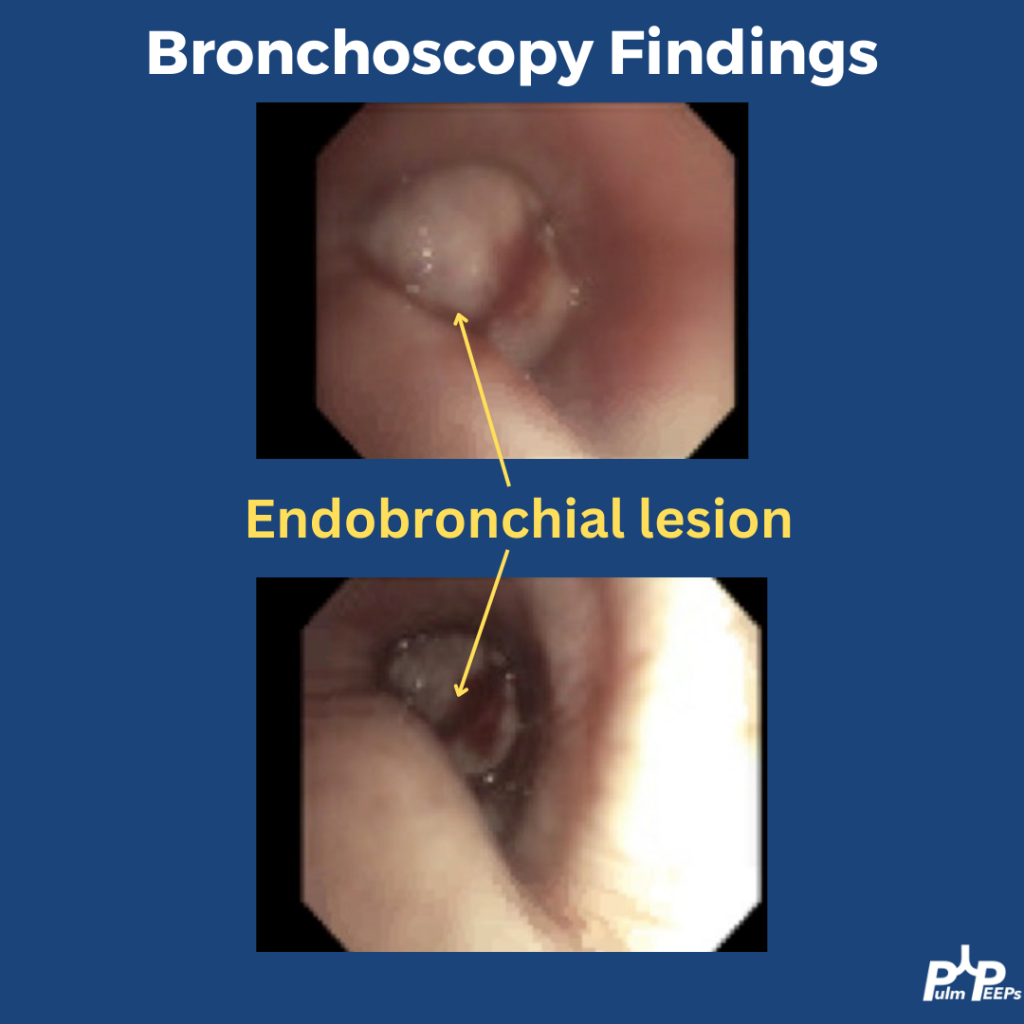
Endobronchial lesions can be malignant or benign, and within malignancy then can be primary or secondary. This patient had no clinical signs of pneumonia and no clear reason to mucus plug so malignancy was top of the differential. Here are differential considerations:
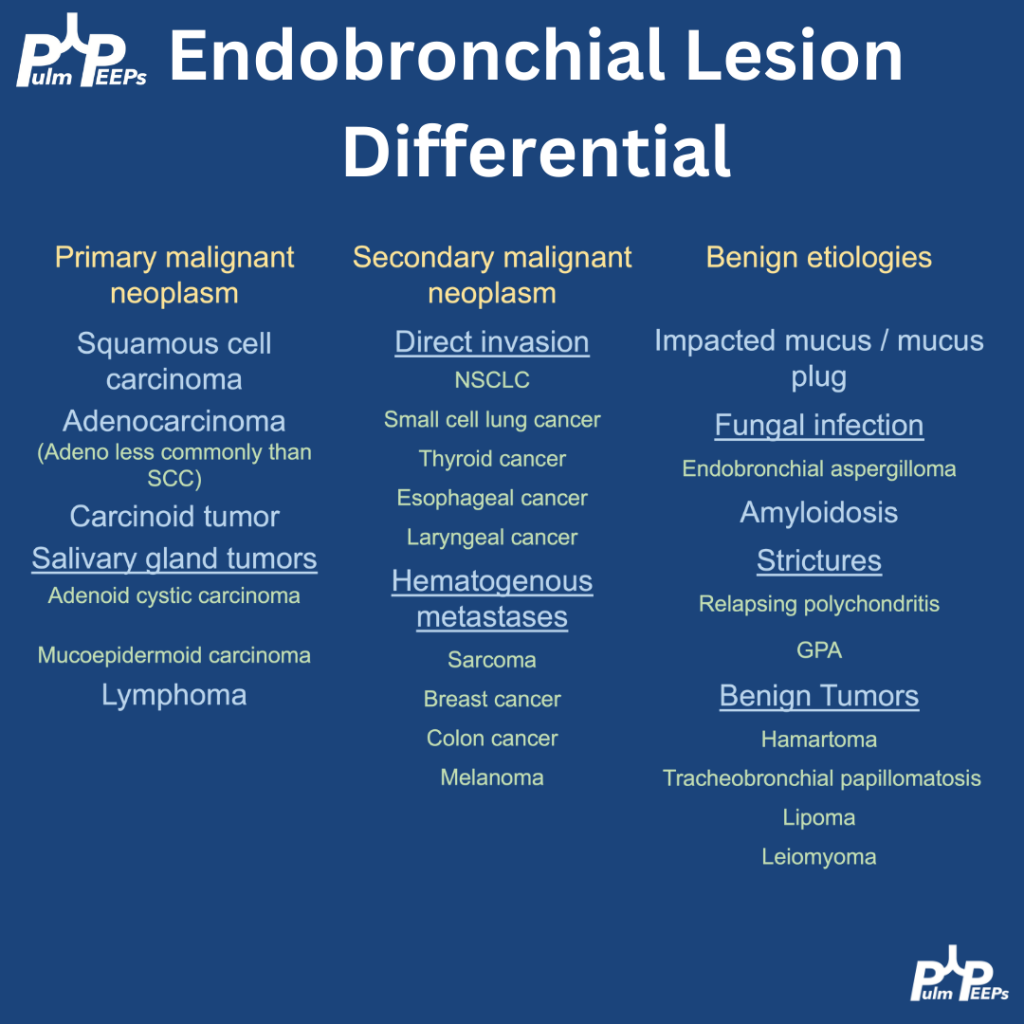
The pathology returned positive for a carcinoid tumor, which can typically arise as endbronchial lesions. PET/CT showed only local disease (femur fracture unrelated), and she is planned for rigid bronchoscopy with laser therapy and corecath ablation for definitive resection.