Today on Pulm PEEPs, we are joined by two pioneers in the field of post-intensive care outcomes and delirium research. Drs. Dale Needham and Wes Ely talk to us all about the Post Intensive Care Syndrome (PICS) and cover everything from how it was first recognized, to the impact it has, and, most importantly, what we can do to prevent it. This is a huge topic in the field of critical care and we’re thrilled to be delving into it with such knowledgeable guides.
Meet Our Guests
Wes Ely is the Grant W. Liddle Chair in Medicine and a Professor of Medicine at Vanderbilt University Medical Center. He is also the Associate Director of Aging Research at the VA Tennessee Valley Geriatric Research and Education Clinical Center and the co-director of the Critical, Illness, Brain Dysfunction and Survivorship Center. He has published 100s of manuscripts on critical illness survivorship and delirium. He also published a book called “Every Deep-Drawn Breath” about his and his patients’ experiences in the ICU and about the ramifications of critical illness. All net proceeds for the book are going to the CIBS Center Endowment for Survivorship
Dale Needham is a Professor of Medicine at Johns Hopkins, where he is also the Medical Director of the Critical Care Physical Medicine and Rehabilitation Program and the Director of the Outcomes After Critical Illness and Surgery Group. He is the author of 100s of publications focusing on post-ICU outcomes and has received numerous research grants from the NIH and other organizations.
Key Learning Points
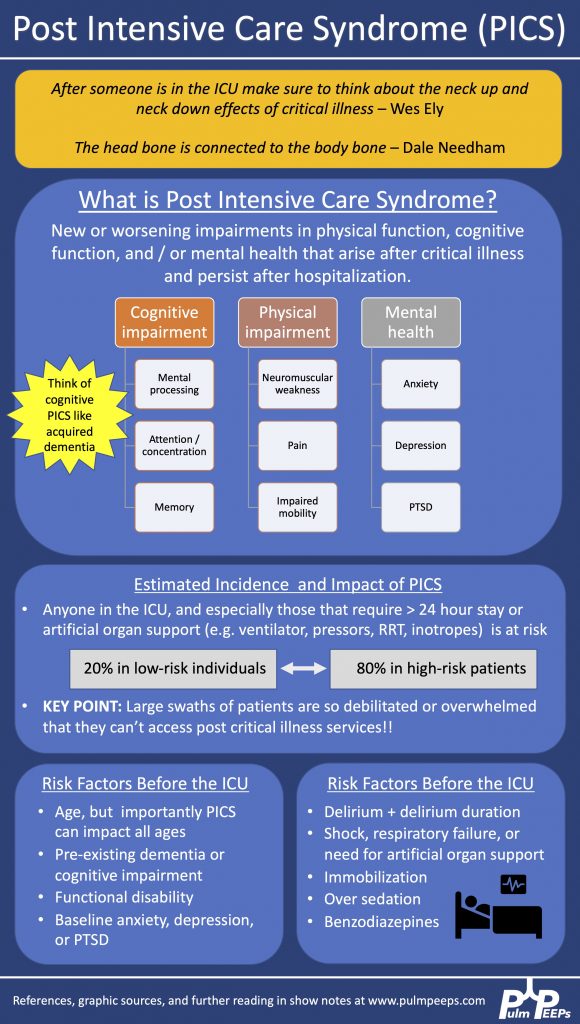
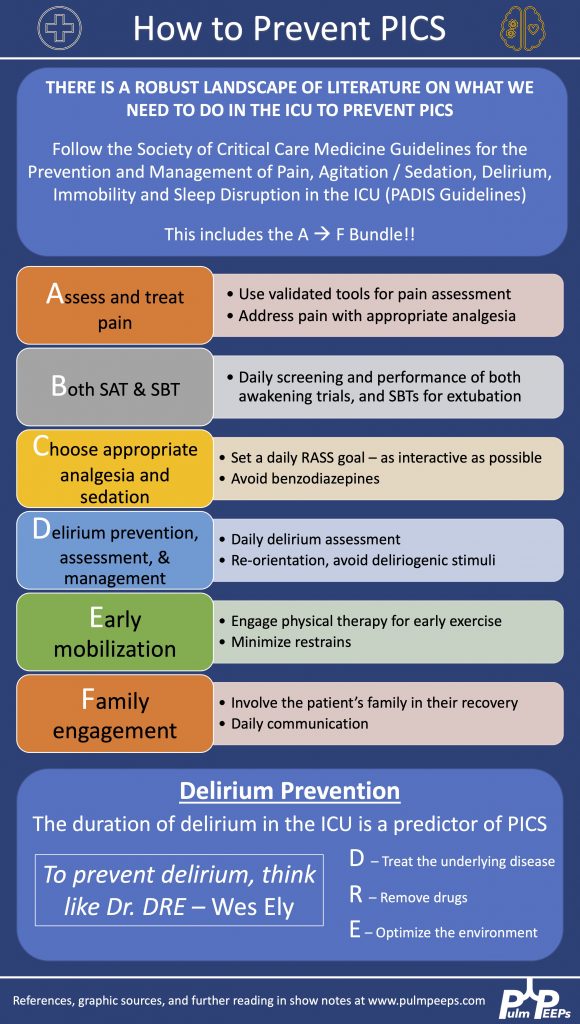
Visit our website www.pulmpeeps.com to see the key learning points from this episode summarized in two infographics.
References and links for further reading
- Devlin JW, Skrobik Y, Gélinas C, et al. Executive Summary: Clinical Practice Guidelines for the Prevention and Management of Pain, Agitation/Sedation, Delirium, Immobility, and Sleep Disruption in Adult Patients in the ICU. Critical Care Medicine. 2018;46(9):1532-1548. doi:10.1097/CCM.0000000000003259
- Ely EW. The ABCDEF Bundle: Science and Philosophy of How ICU Liberation Serves Patients and Families. Crit Care Med. 2017;45(2):321-330. doi:10.1097/CCM.0000000000002175
- Mikkelsen ME, Still M, Anderson BJ, et al. Society of Critical Care Medicine’s International Consensus Conference on Prediction and Identification of Long-Term Impairments After Critical Illness. Crit Care Med. 2020;48(11):1670-1679. doi:10.1097/CCM.0000000000004586
- Needham DM, Sepulveda KA, Dinglas VD, et al. Core Outcome Measures for Clinical Research in Acute Respiratory Failure Survivors. An International Modified Delphi Consensus Study. Am J Respir Crit Care Med. 2017;196(9):1122-1130. doi:10.1164/rccm.201702-0372OC
- Needham DM, Wozniak AW, Hough CL, et al. Risk Factors for Physical Impairment after Acute Lung Injury in a National, Multicenter Study. Am J Respir Crit Care Med. 2014;189(10):1214-1224. doi:10.1164/rccm.201401-0158OC
- Semler MW, Bernard GR, Aaron SD, et al. Identifying Clinical Research Priorities in Adult Pulmonary and Critical Care. NHLBI Working Group Report. Am J Respir Crit Care Med. 2020;202(4):511-523. doi:10.1164/rccm.201908-1595WS
- Spruit MA, Holland AE, Singh SJ, Tonia T, Wilson KC, Troosters T. COVID-19: Interim Guidance on Rehabilitation in the Hospital and Post-Hospital Phase from a European Respiratory Society and American Thoracic Society-coordinated International Task Force. Eur Respir J. Published online August 13, 2020:2002197. doi:10.1183/13993003.02197-2020
- Turnbull AE, Sepulveda KA, Dinglas VD, Chessare CM, Bingham CO, Needham DM. Core Domains for Clinical Research in Acute Respiratory Failure Survivors: An International Modified Delphi Consensus Study. Crit Care Med. 2017;45(6):1001-1010. doi:10.1097/CCM.0000000000002435
- Ward DS, Absalom AR, Aitken LM, et al. Design of Clinical Trials Evaluating Sedation in Critically Ill Adults Undergoing Mechanical Ventilation: Recommendations From Sedation Consortium on Endpoints and Procedures for Treatment, Education, and Research (SCEPTER) Recommendation III. Crit Care Med. 2021;49(10):1684-1693. doi:10.1097/CCM.0000000000005049
- Ozga D, Krupa S, Witt P, Mędrzycka-Dąbrowska W. Nursing Interventions to Prevent Delirium in Critically Ill Patients in the Intensive Care Unit during the COVID19 Pandemic—Narrative Overview. Healthcare. 2020;8:578. doi:10.3390/healthcare8040578
Podcast: Play in new window | Download
Subscribe: Apple Podcasts | Spotify | Amazon Music | Android | iHeartRadio | Podcast Index | RSS